 2023, Vol. 44
2023, Vol. 44文章信息
- 王淑琳, 张向辉, 木拉提, 郭恒, 何佳, 热米娜, 王馨平, 马儒林, 郭淑霞.
- Wang Shulin, Zhang Xianghui, Mulatibieke, Guo Heng, He Jia, Remina, Wang Xinping, Ma Rulin, Guo Shuxia
- 甘油三酯葡萄糖乘积指数及结合肥胖指标与心血管疾病关联的前瞻性队列研究
- Prospective cohort study of the association of cardiovascular disease with triglyceride glucose index and triglyceride glucose-related indicators
- 中华流行病学杂志, 2023, 44(12): 1943-1949
- Chinese Journal of Epidemiology, 2023, 44(12): 1943-1949
- http://dx.doi.org/10.3760/cma.j.cn112338-20230416-00242
-
文章历史
收稿日期: 2023-04-16




2. 国家卫生健康委中亚高发病防治重点实验室, 石河子 832000
2. National Health Commission Key Laboratory of Prevention and Treatment of Central Asia High Incidence Diseases, Shihezi 832000, China
心血管疾病(CVD)是严重威胁人类健康的主要疾病,在全球慢性非传染性疾病死因构成比中居于首位,约占总死亡人数的1/3[1]。我国CVD患病率呈持续增高趋势,因CVD导致的疾病负担不断加重[2]。因此,早期识别和控制危险因素对CVD预防具有重要意义。胰岛素抵抗(IR)在CVD发生、发展中发挥着重要作用[3]。近年来,有学者提出由FPG和TG计算所得的甘油三酯葡萄糖乘积指数(TyG)是评估IR的简易替代指标[4]。与传统的IR标志物相比,TyG计算方法简单、成本低、易测量。已有研究采用TyG预测CVD的发生[5-7]。TyG结合肥胖指标[TyG-BMI、TyG-腰围身高比(WHtR)]在代谢性疾病研究中受到越来越多的关注,但CVD相关研究较少[8-9]。此外,作为IR替代指标的TyG可作为肥胖和CVD关联的重要中介因素[10-11]。
新疆生产建设兵团维吾尔族人群CVD发病率高,但针对TyG及结合肥胖指标相关研究较少[12]。本研究基于前瞻性队列研究探讨TyG及结合肥胖指标与CVD的发病风险关联及肥胖指标(BMI、WHtR)与CVD发病关联中TyG的潜在中介效应,为CVD防治提供参考和科学依据。
对象与方法1. 研究对象:采用典型抽样方法抽取维吾尔族人群聚集的新疆生产建设兵团第三师51团作为调查现场,随机抽样方法抽取51团的5个连队(6、8、11、12、13连)居住≥1年的14 321名≥18岁维吾尔族人群作为调查对象。2016年8-9月开展基线调查,于2019、2020、2021和2022年随访,随访调查内容与基线保持一致。排除317名流动人口、孕妇和无法参与调查者,694名基本信息不完整者,对13 310名研究对象开展基线调查。排除961名基线患冠心病及卒中患者、516名失访者(失访率为3.88%),最终纳入11 833名研究对象数据分析。研究对象均签署知情同意书,本研究通过石河子大学医学院第一附属医院伦理委员会审查(批准文号:KJ2023-121-01)。
2. 资料收集:①问卷调查:接受规范培训的人员对调查对象进行问卷调查,调查内容包括个人基本信息、生活行为习惯、个人及家族疾病史等。②体格检查:采用标准化方法测量身高、体重、腰围、臀围、血压等指标;采用身高体重测量仪测量身高和体重;采用软尺测量腰围;采用电子血压计[HBP-9020,欧姆龙(中国)有限公司]测量血压两次并取平均值。③实验室检测:采集调查对象晨起空腹肘静脉血5 ml,采用OLYMPUS 2007全自动生化仪检测FPG、TG、TC、LDL-C、HDL-C等生化指标。
3. CVD诊断标准:研究主要结局事件为随访期间新发冠心病[《国际疾病分类》第10版(ICD-10):I20~I25]或卒中(ICD-10:I60~I64,I69)[13]。通过问卷调查、当地医院病案记录、社保信息及死亡登记获取新发结局事件数据。若同一研究对象发生多次结局事件,则以第一次结局事件发生时间为终点事件。自我报告结局事件者需提供县级及以上医院临床诊断证明。
4. 相关指标定义:①高血压[14]:SBP≥140 mmHg(1 mmHg=0.133 kPa)和(或)DBP≥90 mmHg,或既往有高血压史,在过去2周内服用抗高血压药物。②吸烟[15]:持续或累计吸烟≥6个月。③饮酒[16]:每月饮酒次数≥2次。④BMI(kg/m2)分组[17]:< 18.5、18.5~、24.0~、≥28.0分别为偏瘦、体重正常、超重、肥胖。⑤锻炼频率[18]:经常锻炼(运动次数≥3次/周,锻炼时间≥30 min/次);偶尔锻炼(运动次数 < 3次/周,锻炼时间 < 30 min/次);几乎不锻炼(运动次数 < 1次/周)。
5. 相关指标计算:①WHtR=腰围(cm)/身高(cm);②TyG=ln[TG(mg/dl)×FPG(mg/dl)/2];③TyG-BMI=TyG×BMI;④TyG-WHtR=TyG×WHtR。
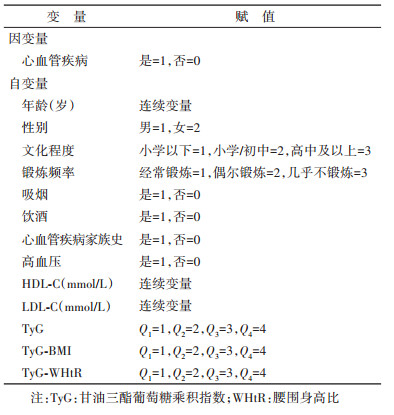
6. 统计学分析:研究对象基本特征以频数和构成比描述,组间比较采用χ2检验。采用Kaplan-Meier法估计TyG、TyG-BMI和TyG-WHtR各四分位数组CVD累积发病率,并用log-rank检验进行组间比较。采用Cox比例风险回归模型分析各指数与CVD发病风险关联,单因素分析中P < 0.05的协变量及传统危险因素纳入多因素Cox比例风险回归模型,赋值见表 1。采用弗雷明汉CVD风险评分模型(Framingham模型)评价TyG、TyG-BMI和TyG-WHtR的增量预测价值[19]。根据曲线下面积(AUC)、净重新分类指数(NRI)和整体鉴别指数(IDI)评估各指数加入是否可以改善模型预测能力。采用Imai等[20]提出的中介分析方法计算肥胖与CVD发病关联中TyG的中介效应。采用SPSS 26.0和R 4.1.2软件进行统计学分析。双侧检验,检验水准α=0.05。
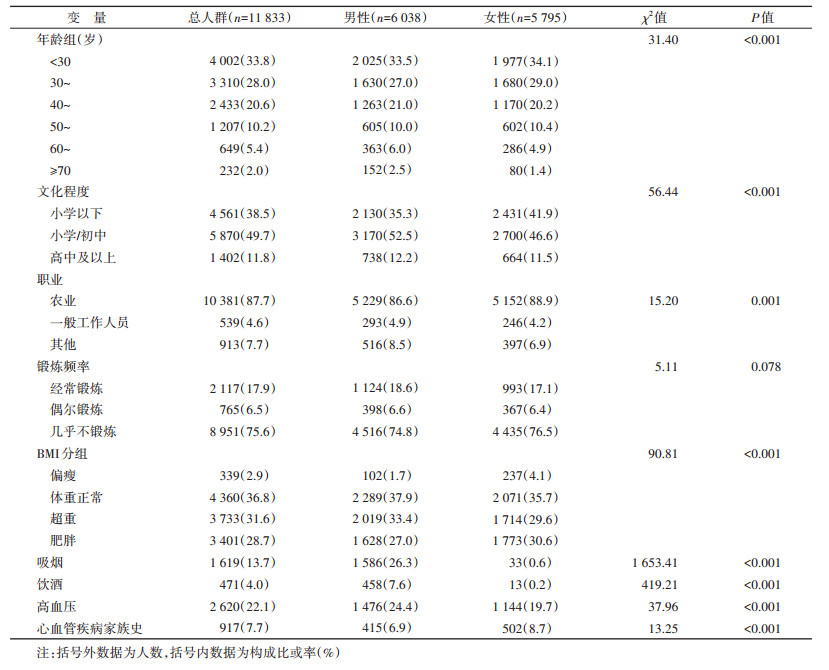
1. 基本情况:共纳入研究对象11 833名,年龄(37.00±13.67)岁,男性6 038名(51.0%)。年龄 < 30岁人数占比最高(33.8%)。文化程度小学以下4 561名(38.5%)、小学/初中5 870名(49.7%),高中及以上1 402名(11.8%)。10 381名从事农业工作,占比最高(87.7%)。相较于女性,男性吸烟、饮酒和高血压占比更高,肥胖和CVD家族史占比更低(均P < 0.001)。男性与女性锻炼频率差异无统计学意义(P > 0.05)。见表 2。
2. CVD发病情况描述:队列中位随访时间5.67年,新发CVD 1 288名,累积发病率为10.9%,发病密度20.50/1 000人年。随TyG及TyG-BMI、TyG-WHtR四分位数升高,CVD累积发病率呈上升趋势(log-rank检验,均P < 0.001)。见图 1。在随访(5.31±1.13)年期间,TyG的Q1~Q4组CVD累积发病率为6.9%、9.8%、12.2%和14.7%;TyG-BMI为4.7%、8.4%、12.3%和18.1%;TyG-WHtR为3.9%、7.6%、12.7%和19.3%。

|
| 注:TyG:甘油三酯葡萄糖乘积指数;WHtR:腰围身高比 图 1 TyG、TyG-BMI、TyG-WHtR四分位数组心血管疾病累积发病率 |
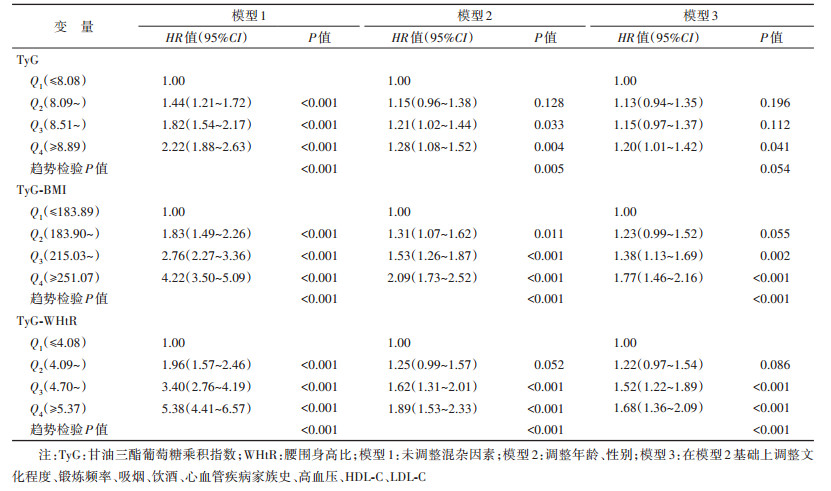
3. TyG及结合肥胖指标与CVD发病风险关联分析:多因素Cox比例风险回归分析显示,与Q1组相比,TyG、TyG-BMI和TyG-WHtR的Q4组CVD发病风险分别增加20%(HR=1.20,95%CI:1.01~1.42)、77%(HR=1.77,95%CI:1.46~2.16)和68%(HR=1.68,95%CI:1.36~2.09)。模型3中TyG-BMI、TyG-WHtR与CVD发病关联呈正相关(趋势检验P < 0.001),TyG与CVD发病风险无明显线性趋势(趋势检验P=0.054)。见表 3。
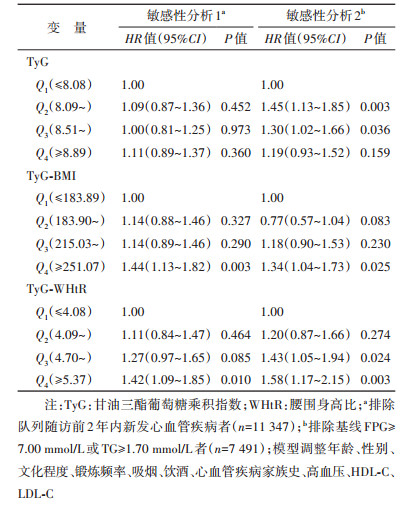
4. TyG及结合肥胖指标与CVD发病风险的敏感性分析:排除队列随访前2年内新发CVD者,TyG-BMI、TyG-WHtR的Q4组与CVD发病风险呈正相关,TyG与CVD发病无统计学关联;排除基线FPG≥7.00 mmol/L或TG≥1.70 mmol/L者,TyG的Q2、Q3组与CVD发病风险呈正相关、Q4组与CVD发病无统计学关联,TyG-BMI的Q4组与CVD发病风险呈正相关、TyG-WHtR的Q3、Q4组与CVD发病风险呈正相关。见表 4。
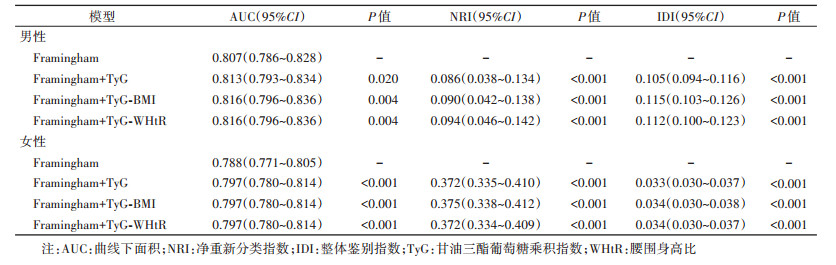
5. TyG及结合肥胖指标对CVD发病风险的预测价值:Framingham模型分别加入TyG、TyG-BMI、TyG-WHtR后,AUC、NRI、IDI均有提升。见表 5。
6. TyG在肥胖与CVD发病风险关联的中介分析:调整年龄、性别、文化程度、锻炼频率、吸烟、饮酒、CVD家族史、高血压、HDL-C、LDL-C因素后,TyG是肥胖(BMI、WHtR)与CVD关联的潜在中介变量。BMI、WHtR与CVD发病关联中,通过TyG介导的中介效应比例分别为10.55%和11.50%(均P < 0.001)。见表 6。

IR是驱动CVD的重要危险因素,由其引起的血管内皮损伤、动脉粥样硬化斑块形成等都会促进CVD的发生发展。高胰岛素-正葡萄糖钳夹试验是评估IR的金标准,但该方法检测过程复杂,价格昂贵,难以在大规模调查中广泛应用。近几年提出的结合FPG和TG的TyG计算简单、易测量,已被证实可用作IR的有效替代指标[7]。CVD相关研究中,TyG常被应用[21]。BMI和WHtR是一类简单、易得的评价全身性和腹型肥胖的指标,TyG与BMI和WHtR结合后用于代谢性疾病的研究较为多见,但CVD相关研究中较少见。
中国新疆生产建设兵团维吾尔族人群CVD发病密度处于较高水平,高于China-PAR项目报道的5.08/1 000人年、开滦队列报道的5.17/1 000人年[22-23]。多项代表性队列研究已证实TyG与CVD发病风险的关联。样本量超40万的英国生物银行队列研究发现,与Q1组相比,TyG的Q4组CVD发生风险增加19%(HR=1.19,95%CI:1.14~1.25)[24]。Sánchez-Íñigo等[7]的10年随访研究结果表明,TyG与高加索人群CVD发病显著相关,是CVD发病风险的独立预测因子。开滦队列研究发现,无传统CVD危险因素的健康个体中,随TyG水平的增加,CVD发病风险增加,Q4组CVD发生风险较Q1组高60%(HR=1.60,95%CI:1.35~1.90)[25]。本研究结果显示,TyG及结合肥胖指标均为CVD发病的独立危险因素,其中以TyG-BMI与CVD关联最强;TyG-BMI的Q4组CVD发病风险较Q1组明显增加,高于英国生物银行及开滦队列研究报告的结果。因此,中国新疆生产建设兵团维吾尔族人群中可将TyG-BMI作为评估CVD发病风险的重要参考指标之一。
Framingham模型是世界范围内被广泛使用的CVD风险预测模型,模型内的预测因子包括年龄、SBP、HDL-C、TC、吸烟状况和糖尿病史[19]。为进一步评估TyG、TyG-BMI和TyG-WHtR对CVD发病风险的预测价值,本研究将各指标分别加入Framingham模型后发现新模型AUC、NRI和IDI均有显著提升。Sánchez-Íñigo等[7]在Framingham模型中加入TyG后,模型预测能力提升。开滦队列研究发现,将TyG添加至具有传统危险因素的模型后,新模型对CVD的预测能力有了明显的改善[26]。本研究结果与上述既往研究保持一致。
现有研究已阐明肥胖与IR关联的内在机制,IR在CVD和继发性高胰岛素血症相关的体重增加中均起到关键作用[27]。本研究结果显示,肥胖与CVD发病关联中,TyG具有部分中介效应。这一结果提示肥胖会导致血脂及代谢产物异常增多,引起IR,提高CVD发病风险。研究认为,腹型肥胖和IR的关系较全身性肥胖更为密切,但本研究未见TyG在全身性肥胖(以BMI衡量)、腹型肥胖(以WHtR衡量)与CVD发病关联的中介效应比例存在明显差异,分析原因主要为腹型肥胖导致IR主要途径是内脏脂肪堆积,但常用于评价腹型肥胖的腰高比等指标并不能精准区分皮下脂肪和内脏脂肪[28-29]。此外,新疆地区的肥胖问题较为严重,应重点关注肥胖人群健康,在健康管理中强调控制体重,阻止或延缓CVD的发生发展[30-31]。
本研究存在局限性。首先,CVD是一种多病因、发病时间漫长的疾病,后期需延长随访时间对研究结果做进一步验证;其次,本研究未考虑TyG及结合肥胖指标随访期间动态变化对新发CVD的影响,后期研究还需考虑TyG动态变化对结局事件的影响;最后,本研究分析范围局限于新疆生产建设兵团维吾尔族人群,应慎重将研究结论外推。
综上所述,TyG及结合肥胖指标水平升高与新疆生产建设兵团维吾尔族人群CVD发病风险显著相关,其中以TyG-BMI与CVD关联最为密切。大规模流行病学调查工作中,监测TyG-BMI对早期识别CVD高风险人群具有重要意义。
利益冲突 所有作者声明无利益冲突
作者贡献声明 王淑琳:现场调查、数据分析、文章撰写;张向辉、木拉提:现场调查、数据分析;何佳、热米娜、王馨平、马儒林:现场调查、数据整理;郭恒、郭淑霞:现场调查、研究设计、论文修改、经费支持
| [1] |
Roth GA, Mensah GA, Fuster V. The global burden of cardiovascular diseases and risks: a compass for global action[J]. J Am Coll Cardiol, 2020, 76(25): 2980-2981. DOI:10.1016/j.jacc.2020.11.021 |
| [2] |
张梦妮, 李茂婷, 职心乐, 等. 1990-2019年中国动脉粥样硬化心血管病疾病负担变化及其危险因素分析[J]. 中华流行病学杂志, 2021, 42(10): 1797-1803. DOI:10.3760/cma.j.cn112338-20201208-01390 Zhang MN, Li MT, Zhi XY, et al. Trends of a burden on atherosclerotic cardiovascular disease and its related risk factors in China, 1990 to 2019[J]. Chin J Epidemiol, 2021, 42(10): 1797-1803. DOI:10.3760/cma.j.cn112338-20201208-01390 |
| [3] |
Nigro J, Osman N, Dart AM, et al. Insulin resistance and atherosclerosis[J]. Endocr Rev, 2006, 27(3): 242-259. DOI:10.1210/er.2005-0007 |
| [4] |
Simental-Mendía LE, Rodríguez-Morán M, Guerrero- Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects[J]. Metab Syndr Relat Disord, 2008, 6(4): 299-304. DOI:10.1089/met.2008.0034 |
| [5] |
Barzegar N, Tohidi M, Hasheminia M, et al. The impact of triglyceride-glucose index on incident cardiovascular events during 16 years of follow-up: Tehran Lipid and Glucose Study[J]. Cardiovasc Diabetol, 2020, 19(1): 155. DOI:10.1186/s12933-020-01121-5 |
| [6] |
Li HB, Zuo YT, Qian F, et al. Triglyceride-glucose index variability and incident cardiovascular disease: a prospective cohort study[J]. Cardiovasc Diabetol, 2022, 21(1): 105. DOI:10.1186/s12933-022-01541-5 |
| [7] |
Sánchez-Íñigo L, Navarro-González D, Fernández-Montero A, et al. The TyG index may predict the development of cardiovascular events[J]. Eur J Clin Invest, 2016, 46(2): 189-197. DOI:10.1111/eci.12583 |
| [8] |
Hu HF, Han Y, Cao CC, et al. The triglyceride glucose-body mass index: a non-invasive index that identifies non-alcoholic fatty liver disease in the general Japanese population[J]. J Transl Med, 2022, 20(1): 398. DOI:10.1186/s12967-022-03611-4 |
| [9] |
Xuan WT, Liu DX, Zhong JN, et al. Impacts of triglyceride glucose-waist to height ratio on diabetes incidence: a secondary analysis of a population-based longitudinal data[J]. Front Endocrinol, 2022, 13: 949831. DOI:10.3389/fendo.2022.949831 |
| [10] |
Reaven GM. Insulin resistance: the link between obesity and cardiovascular disease[J]. Med Clin North Am, 2011, 95(5): 875-892. DOI:10.1016/j.mcna.2011.06.002 |
| [11] |
Li SS, Guo BX, Chen HN, et al. The role of the triglyceride (triacylglycerol) glucose index in the development of cardiovascular events: a retrospective cohort analysis[J]. Sci Rep, 2019, 9(1): 7320. DOI:10.1038/s41598-019-43776-5 |
| [12] |
Guo YB, Yang J, Ma RL, et al. Metabolic dysfunction- associated fatty liver disease is associated with the risk of incident cardiovascular disease: a prospective cohort study in Xinjiang[J]. Nutrients, 2022, 14(12): 2361. DOI:10.3390/nu14122361 |
| [13] |
Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American heart association[J]. Circulation, 2022, 145(8): e153-639. DOI:10.1161/cir.0000000000001052 |
| [14] |
中国高血压防治指南修订委员会, 高血压联盟(中国, 中华医学会心血管病学分会中国医师协会高血压专业委员会, 等. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志, 2019, 24(1): 24-56. DOI:10.3969/j.issn.1007-5410.2019.01.002 Writing Group of Chinese Guidelines for the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology, et al. 2018 Chinese guidelines for the management of hypertension[J]. Chin J Cardiovasc Med, 2019, 24(1): 24-56. DOI:10.3969/j.issn.1007-5410.2019.01.002 |
| [15] |
Centers for Disease Control and Prevention (CDC). Cigarette smoking among adults-United States, 1992, and changes in the definition of current cigarette smoking[J]. MMWR Morb Mortal Wkly Rep, 1994, 43(19): 342-346. |
| [16] |
Sun K, Ren M, Liu D, et al. Alcohol consumption and risk of metabolic syndrome: a meta-analysis of prospective studies[J]. Clin Nutr, 2014, 33(4): 596-602. DOI:10.1016/j.clnu.2013.10.003 |
| [17] |
陈春明, 孔灵芝. 中国成人超重和肥胖症预防控制指南[M]. 北京: 人民卫生出版社, 2006. Chen CM, Kong LZ. Guideline for prevention and control of overweight and obesity in Chinese adults[M]. Beijing: People's Medical Publishing House, 2006. |
| [18] |
中华人民共和国国家卫生健康委员会. 健康中国行动(2019-2030年) [EB/OL]. (2019-07-15) [2023-04-06]. http://www.nhc.gov.cn/guihuaxxs/s3585u/201907/e9275fb95d5b4295be8308415d4cd1b.shtml.
|
| [19] |
D'Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study[J]. Circulation, 2008, 117(6): 743-753. DOI:10.1161/circulationaha.107.699579 |
| [20] |
Imai K, Keele L, Tingley D. A general approach to causal mediation analysis[J]. Psychol Methods, 2010, 15(4): 309-334. DOI:10.1037/a0020761 |
| [21] |
Lopez-Jaramillo P, Gomez-Arbelaez D, Martinez-Bello D, et al. Association of the triglyceride glucose index as a measure of insulin resistance with mortality and cardiovascular disease in populations from five continents (PURE study): a prospective cohort study[J]. Lancet Healthy Longev, 2023, 4(1): e23-33. DOI:10.1016/s2666-7568(22)00247-1 |
| [22] |
Han C, Liu FC, Yang XL, et al. Ideal cardiovascular health and incidence of atherosclerotic cardiovascular disease among Chinese adults: the China-PAR project[J]. Sci China Life Sci, 2018, 61(5): 504-514. DOI:10.1007/s11427-018-9281-6 |
| [23] |
马一涵, 李兴雨, 韩旭, 等. 动脉硬化与原发性高血压对心脑血管疾病发病的影响及联合作用: 基于8年的随访研究[J]. 中国全科医学, 2021, 24(23): 2907-2913. DOI:10.12114/j.issn.1007-9572.2021.01.204 Ma YH, Li XY, Han X, et al. The influence and combined effect of arteriosclerosis and essential hypertension on the pathogenesis of cardiovascular and cerebrovascular diseases: a 8-year follow-up study[J]. Chin General Pract, 2021, 24(23): 2907-2913. DOI:10.12114/j.issn.1007-9572.2021.01.204 |
| [24] |
Che BZ, Zhong CK, Zhang RJ, et al. Triglyceride-glucose index and triglyceride to high-density lipoprotein cholesterol ratio as potential cardiovascular disease risk factors: an analysis of UK biobank data[J]. Cardiovasc Diabetol, 2023, 22(1): 34. DOI:10.1186/s12933-023-01762-2 |
| [25] |
张彤, 田雪, 左颖婷, 等. 无传统危险因素人群中TyG指数与心脑血管疾病的关系[J]. 上海交通大学学报: 医学版, 2022, 42(3): 267-274. DOI:10.3969/j.issn.1674-8115.2022.03.002 Zhang T, Tian X, Zuo YT, et al. Association of triglyceride-glucose index with cardiovascular disease in people without traditional risk factors[J]. J Shanghai Jiaotong Univ: Med Sci, 2022, 42(3): 267-274. DOI:10.3969/j.issn.1674-8115.2022.03.002 |
| [26] |
Wang AX, Tian X, Zuo YT, et al. Change in triglyceride-glucose index predicts the risk of cardiovascular disease in the general population: a prospective cohort study[J]. Cardiovasc Diabetol, 2021, 20(1): 113. DOI:10.1186/s12933-021-01305-7 |
| [27] |
Barber TM, Kyrou I, Randeva HS, et al. Mechanisms of insulin resistance at the crossroad of obesity with associated metabolic abnormalities and cognitive dysfunction[J]. Int J Mol Sci, 2021, 22(2): 546. DOI:10.3390/ijms22020546 |
| [28] |
Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update[J]. Physiol Rev, 2013, 93(1): 359-404. DOI:10.1152/physrev.00033.2011 |
| [29] |
Kahn B B, Flier J S. Obesity and insulin resistance[J]. J Clin Invest, 2000, 106(4): 473-481. DOI:10.1172/jci10842 |
| [30] |
郑聪毅, 王增武, 陈祚, 等. 新疆、西藏地区居民肥胖类型与10年冠心病发病风险关系的研究[J]. 中华流行病学杂志, 2017, 38(6): 721-726. DOI:10.3760/cma.j.issn.0254-6450.2017.06.006 Zheng CY, Wang ZW, Chen Z, et al. Association between the types of obesity and the 10-year-coronary heart disease risk, in Tibet Autonomous Region and Xinjiang Uygur Autonomous Region[J]. Chin J Epidemiol, 2017, 38(6): 721-726. DOI:10.3760/cma.j.issn.0254-6450.2017.06.006 |
| [31] |
中国营养学会肥胖防控分会, 中国营养学会临床营养分会, 中华预防医学会行为健康分会, 等. 中国居民肥胖防治专家共识[J]. 中华流行病学杂志, 2022, 43(5): 609-626. DOI:10.3760/cma.j.cn112338-20220402-00253 Chinese Nutrition Society Obesity Prevention and Control Section, Chinese Nutrition Society Clinical Nutrition Section, Chinese Preventive Medicine Association Behavioral Health Section, et al. Expert consensus on obesity prevention and treatment in China[J]. Chin J Epidemiol, 2022, 43(5): 609-626. DOI:10.3760/cma.j.cn112338-20220402-00253 |