 2023, Vol. 44
2023, Vol. 44文章信息
- 赖雪峰, 刘志科, 沈鹏, 孙烨祥, 陆怀初, 詹思延, 林鸿波.
- Lai Xuefeng, Liu Zhike, Shen Peng, Sun Yexiang, Lu Huaichu, Zhan Siyan, Lin Hongbo
- 宁波市鄞州区2016-2021年系统性红斑狼疮发病的流行病学研究
- Epidemiological study of incidence of systematic lupus erythematosus in Yinzhou, Ningbo, 2016-2021
- 中华流行病学杂志, 2023, 44(7): 1080-1085
- Chinese Journal of Epidemiology, 2023, 44(7): 1080-1085
- http://dx.doi.org/10.3760/cma.j.cn112338-20221225-01081
-
文章历史
收稿日期: 2022-12-25




2. 宁波市鄞州区疾病预防控制中心, 宁波 315199
2. Yinzhou District Center for Disease Control and Prevention of Ningbo, Ningbo 315199, China
系统性红斑狼疮(SLE)是一种慢性、系统性的自身免疫性疾病,临床可表现为多个系统的病变[1]。SLE的发病以女性为主,女性与男性的发病密度比在2∶1[2]~15∶1[3]之间。疾病对育龄期女性影响较大,目前已成为年轻女性的主要死因之一[4]。我国SLE流行病学研究起步较晚,主要采用传统的流行病学调查,受限于研究方法和数据资料,相关研究较少,且主要为患病率研究[5-7]。本研究基于宁波市鄞州区域健康信息平台(YRHIP)开展回顾性队列研究,描述鄞州区SLE发病的流行病学特征与趋势,为SLE的病因学和防控策略等研究提供基础数据。
对象与方法1. 数据来源:研究对象来自YRHIP,该纵向数据库整合了鄞州区电子病历、疾病监测与管理数据、死亡登记以及其他卫生保健信息[8]。自2009年起,该数据库涵盖了鄞州区居民全生命周期的健康相关活动记录。截至2017年,该平台覆盖了鄞州区98%的常住人口,包含鄞州区全部医院及其附属社区卫生服务中心的卫生保健数据,并在2020年“国家卫生信息互联互通标准化成熟度等级”测评中获得5级乙等(全国区域化卫生信息平台最高等级)[9],为开展SLE发病的流行特征研究提供了良好的数据支持。
2. 研究设计:采用回顾性队列设计,收集了YRHIP在2015年1月1日至2021年10月31日的数据,构建鄞州区常住居民动态队列。研究对象纳入标准:①2015年1月1日至2021年10月31日鄞州区常住人口;②研究期间在YRHIP中的记录 > 1年;③具有完整的个人唯一识别码和居民健康档案建档日期。
队列开始时间为2016年1月1日或建档日期加1年(二者中较晚的日期)。队列结束的时间为以下事件中最早发生的日期:①由于区划调整划出鄞州区;②死亡;③诊断为SLE;④健康档案的管理状态为“迁出”“临时”等其他情况且未发生上述事件的研究对象,在宁波市最后一次就诊的时间;⑤2021年10月31日。
本研究纳入的SLE新发病例需满足条件:①门/急诊或住院患者;②首次出现的具有符合《国际疾病分类》第十版(ICD-10)编码M32.x对应疾病名称的文本诊断,为排除现患病例的影响,本研究参考既往研究[10-12],设置1年为洗脱期,排除了在洗脱期内有SLE诊断记录的患者;③满足SLE病例识别算法的患者。
3. 资料整理:从YRHIP提取研究对象的匿名化数据,其中,从健康档案信息系统中提取研究对象的基本信息,包括隐匿化的个人唯一识别码、性别、出生日期、建档日期;从死亡登记系统中提取死亡日期和死因;从电子病历系统中提取患者在宁波市内就诊的疾病诊断、检查和处方相关信息。
采用ICD-10中编码“M32”或中文文本“狼疮”模糊匹配的方式,识别SLE疑似病例,剔除散播性粟粒性狼疮、寻常狼疮以及局限性/皮肤型红斑狼疮(ICD-10编码L93.x)。
2012年系统性红斑狼疮国际协作组(SLICC-2012)和2019年欧洲抗风湿病联盟/美国风湿病学会(EULAR/ACR-2019)分类标准已被证明具有较高的灵敏度和特异性[13],且对病例识别的一致性较好[14]。本研究以满足SLICC-2012或EULAR/ACR-2019分类标准为确认SLE病例的参考标准,以是否有免疫学指标检查、门/急诊记录(≥1次vs. ≥2次)和住院记录(0次vs. ≥1次)中目标疾病诊断频次、是否有SLE用药记录等信息构建SLE病例的识别算法,比较不同算法组合的阳性预测值和灵敏度,最终确定SLE病例的识别算法:①中文诊断名称包含“系统性红斑狼疮”或ICD-10编码M32.x对应的疾病名称,或诊断编码为M32.x;②在数据库中有至少1次住院记录和/或至少2次门/急诊记录符合上述诊断。经验证,该识别算法的阳性预测值为81.36%,在有相关免疫检查指标的疑似病例中的灵敏度为96.26%。本研究最终纳入该算法识别的SLE新发病例进行分析,以首次明确诊断SLE的时间为发病时间。
本研究已通过北京大学生物医学伦理委员会的审查(批准文号:IRB00001052-18013)。
4. 统计学分析:使用HiveSQL软件进行数据清洗和提取。使用Stata 15.0软件进行数据整理和统计分析。连续型变量服从正态分布者报告x±s,服从偏态分布者报告M(Q1,Q3);分类变量报告频数和百分比(%)。研究人群的发病密度以及各年份、性别和年龄组的发病密度的95%CI采用泊松分布的方法估计。双侧检验,检验水准α=0.05。
为评估结果稳健性,本研究进行了敏感性分析:将新发病例的洗脱期延长至2年,以排除潜在的现患病例。
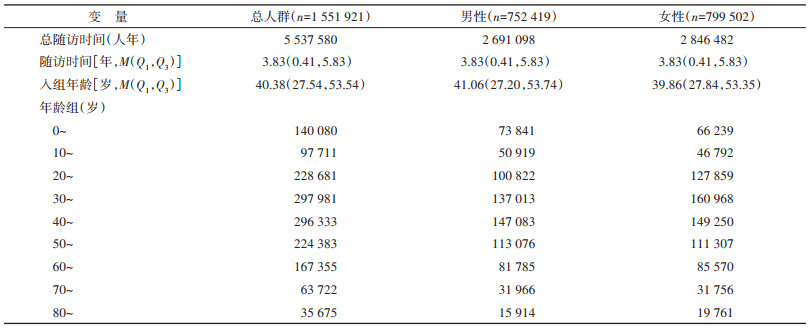
结果1. 一般人口学特征:2016-2021年符合本研究纳入标准的研究对象1 551 921人,其中女性799 502人,占51.52%。入组年龄M(Q1,Q3)为40.38(27.54,53.54)岁,总随访时间5 537 580人年,随访时间M(Q1,Q3)为3.83(0.41,5.83)年。见表 1。
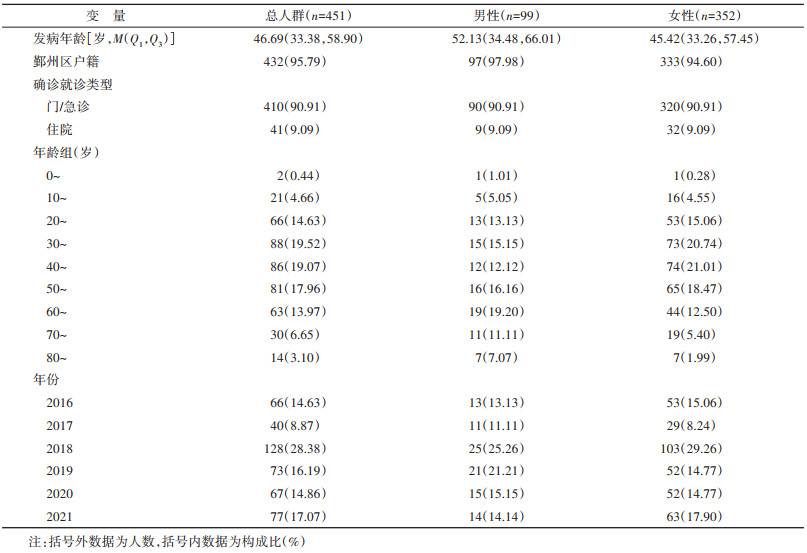
研究期间共有451例SLE新发病例,其中女性352例(78.05%)。发病年龄M(Q1,Q3)为46.69(33.38,58.90)岁,男性发病年龄为60~69岁组占比最高(19.20%),女性发病年龄为30~39岁和40~49岁组占比较高,分别为20.74%和21.01%(表 2)。
2. SLE发病密度:
(1)总研究人群发病密度及其人群分布:2016- 2021年鄞州区SLE的总发病密度为8.14/10万人年(95%CI:7.41/10万人年~8.93/10万人年)。SLE在男性的发病密度为3.68/10万人年(95%CI:2.99/10万人年~4.48/10万人年),女性发病密度为12.37/10万人年(95%CI:11.11/10万人年~13.73/10万人年),女性的发病密度是男性的3.36倍。男性的发病密度在20~29岁有个小高峰,从40岁开始随着年龄的增长不断升高。在女性中,SLE发病密度在20~29岁最高,达到16.57/10万人年(95%CI:12.41/10万人年~21.68/10万人年),随后到79岁均维持在较高水平(图 1)。

|
| 图 1 2016-2021年宁波市鄞州区系统性红斑狼疮发病密度的年龄分布 |
(2)时间分布特征:2016-2021年鄞州区SLE的发病密度在男性(P=0.848)和女性(P=1.000)中均无明显随时间变化的趋势(图 2)。

|
| 图 2 2016-2021年宁波市鄞州区系统性红斑狼疮发病密度的时间分布 |
3. 敏感性分析:将洗脱期延长至2年,同时纳入2015年之前的数据对现患病例进行排除,得到2016-2021年鄞州区SLE的发病密度为7.62/10万人年(95%CI:6.88/10万人年~8.42/10万人年),男性发病密度为3.59/10万人年(95%CI:2.88/10万人年~4.41/10万人年),女性发病密度为11.44/10万人年(95%CI:10.18/10万人年~12.81/10万人年),女性的发病密度是男性的3.19倍,与主分析结果相近。在年龄和时间分布上,男性和女性发病密度的趋势均与主分析一致。
讨论本研究基于YRHIP的纵向数据开展回顾性队列研究,描述了2016-2021年鄞州区常住居民的SLE发病密度及其人群和时间分布特征。本研究结果显示,女性SLE发病密度高于男性。男性的发病密度在青年时期出现小高峰后,从40岁开始随年龄增长而升高,而女性发病密度在20~29岁最高。近6年SLE的发病密度无随时间变化的趋势。
SLE的既往流行病学研究多基于与国家登记数据相链接的综合性卫生保健数据库开展[15],但这要求国家有较为完善的公共卫生保健系统和可靠的人口普查数据,在一些发展中国家往往难以实现。近年来,也有一些国家基于电子医疗数据库开展SLE流行病学研究,成本较低且覆盖人群范围广[16-18]。本研究基于YRHIP的纵向数据,估算2016- 2021年中国宁波市鄞州区SLE发病密度,与既往报道中国台湾地区2001-2007年的8.1/10万人年[6]、2001-2011年的8.7/10万人年[7],以及中国香港地区1999-2008年的6.7/10万人年相近[5]。与全球其他地区相比,本研究结果稍高于美洲地区(1.4/10万人年~6.3/10万人年)[19-20]、欧洲地区(1.5/10万人年~7.4/10万人年)[21-22]以及亚洲地区的一些发达国家(1.03/10万人年~2.5/10万人年)[17, 23],但与亚洲地区的其他发展中国家相近(8.6/10万人年)[24]。既往研究显示SLE的发病率在不同种族之间存在较大差异[25],但由于缺乏非洲地区SLE发病数据的报道,尚无法与该地区比较[26]。
在人群分布上,根据既往文献,不同国家和地区报告SLE在女性与男性的发病密度比在2∶1~15∶1之间[27],欧洲地区的研究结果接近6∶1[16, 18, 28-29],美洲地区报告的比值在3.4∶1~10.0∶1之间[30-32],而本研究女性与男性的发病密度比为3.36∶1,低于大多数国家的研究,也明显低于中国香港地区的9.8∶1[5]和中国台湾地区的7∶1[6-7],提示不同国家和地区,乃至同一国家的不同地区之间SLE发病密度的性别比存在较大差异。此外,与既往研究一致,本研究中大部分年龄组均表现出女性高发的特点,且男女性的发病差异在中年组表现最为显著[27],这一特征也与SLE在不同性别人群中的年龄分布差异相关。在男性中,SLE的发病密度在青年时期出现小高峰后便随年龄的增加而升高,而女性在青年时期达到高峰,随后维持在较高水平,与既往多项研究的描述基本一致[6, 27-28, 33]。
在时间趋势上,根据既往文献,不同国家和地区的发病率随时间变化的趋势存在差异。欧洲地区的一些国家如丹麦[28]和英国[34]报道的发病密度从20世纪80年代开始到21世纪初无明显的时间变化趋势或有随时间下降的趋势[27],而希腊西北部的发病密度则稍有上升,但升高趋势并不显著[35]。美国多项研究显示20世纪60-90年代SLE的发病密度也较为稳定[32]。而中国台湾地区2003-2011年的数据则显示SLE发病密度有随时间升高的趋势[7]。在本研究中,近6年SLE的发病密度在总人群、男性、女性中均无明显的时间变化趋势,大体上较稳定。需要注意的是,SLE新发病例的诊断与当地综合医院对该病诊疗水平、风湿免疫科的调整和发展有关,而患者的发病也受到环境因素如紫外线强度的影响[36],这些因素均可能造成观察期内某一年度病例数的增加。而由于SLE发病水平较低,病例数量的少量增加就有可能引起发病密度的明显升高。
本研究基于YRHIP这一高覆盖面、高质量的纵向数据库开展,通过数据库之间的连接可以较为准确地识别新发患者并对患者进行随访,相比于传统的流行病学调查方法,具有成本低、效率高、精准度好的优势;本研究对病例进行了数据库内验证,在一定程度上减小了错分偏倚;此外,本研究延长洗脱期至2年进行敏感性分析,结果较为稳健,表明1年的洗脱期可较为准确地识别SLE新发患者。
本研究存在局限性。①由于满足参考标准的病例仅限于做了相关免疫指标检查的患者,极小一部分患者由于资料不完整,使用算法进行识别仍可能存在错分偏倚;②本研究基于电子病历系统识别病例,无法解决未就诊者的发病或患病情况,但SLE是一种以复发-缓解为特征的慢性病,在长期随访过程中极大部分患者会出现轻至重度的疾病状态[36],表现出明显的临床症状,患者会为缓解症状就医,从而被诊出并录入数据库;③SLE的发病受环境、种族等因素影响,而本研究人群仅为鄞州区常住居民,将结果外推至全国或国外其他地区的人群时可能代表性不足。
综上所述,2016-2021年鄞州区SLE的发病密度大体上较为稳定。尽管SLE相对罕见,其发病密度在女性中较高,且对老年人以及育龄期女性影响较大,卫生部门和医疗机构应对其预防、诊断和控制予以重视。目前我国SLE相关流行病学数据仍较为匮乏,有必要开展更大规模、更长随访时间以及更具人群代表性的流行病学研究,为SLE的防治提供可靠数据参考。
利益冲突 所有作者声明无利益冲突
作者贡献声明 赖雪峰:数据整理、统计学分析、论文撰写;刘志科:数据整理、论文修改;沈鹏、孙烨祥、陆怀初:数据整理、论文修改、研究指导;詹思延、林鸿波:论文修改、经费支持、研究指导
| [1] |
Lisnevskaia L, Murphy G, Isenberg D. Systemic lupus erythematosus[J]. Lancet, 2014, 384(9957): 1878-1888. DOI:10.1016/S0140-6736(14)60128-8 |
| [2] |
Michet Jr CJ, McKenna CH, Elveback LR, et al. Epidemiology of systemic lupus erythematosus and other connective tissue diseases in Rochester, Minnesota, 1950 through 1979[J]. Mayo Clin Proc, 1985, 60(2): 105-113. DOI:10.1016/S0025-6196(12)60294-8 |
| [3] |
Vincent FB, Bourke P, Morand EF, et al. Focus on systemic lupus erythematosus in indigenous Australians: towards a better understanding of autoimmune diseases[J]. Intern Med J, 2013, 43(3): 227-234. DOI:10.1111/imj.12039 |
| [4] |
Borchers AT, Keen CL, Shoenfeld Y, et al. Surviving the butterfly and the wolf: mortality trends in systemic lupus erythematosus[J]. Autoimmun Rev, 2004, 3(6): 423-453. DOI:10.1016/j.autrev.2004.04.002 |
| [5] |
Mok CC. Epidemiology and survival of systemic lupus erythematosus in Hong Kong Chinese[J]. Lupus, 2011, 20(7): 767-771. DOI:10.1177/0961203310388447 |
| [6] |
Chiu YM, Lai CH. Nationwide population-based epidemiologic study of systemic lupus erythematosus in Taiwan[J]. Lupus, 2010, 19(10): 1250-1255. DOI:10.1177/0961203310373780 |
| [7] |
Leong PY, Huang JY, Chiou JY, et al. The prevalence and incidence of systemic lupus erythematosus in Taiwan: a nationwide population-based study[J]. Sci Rep, 2021, 11(1): 5631. DOI:10.1038/s41598-021-84957-5 |
| [8] |
Lin HB, Tang X, Shen P, et al. Using big data to improve cardiovascular care and outcomes in China: a protocol for the Chinese Electronic health Records Research in Yinzhou (CHERRY) study[J]. BMJ Open, 2018, 8(2): e019698. DOI:10.1136/bmjopen-2017-019698 |
| [9] |
Liu GX, Liu ZK, Zhao HY, et al. The effectiveness of influenza vaccine among elderly Chinese: a regression discontinuity design based on Yinzhou regional health information platform[J]. Hum Vaccin Immunother, 2022, 18(6): 2115751. DOI:10.1080/21645515.2022.2115751 |
| [10] |
Kan H, Nagar S, Patel J, et al. Longitudinal treatment patterns and associated outcomes in patients with newly diagnosed systemic lupus erythematosus[J]. Clin Ther, 2016, 38(3): 610-624. DOI:10.1016/j.clinthera.2016.01.016 |
| [11] |
Hanly JG, Sayani A, Doucette S, et al. Treatment pathways in an inception lupus cohort over the first three years[J]. Lupus, 2017, 26(2): 119-124. DOI:10.1177/0961203316655213 |
| [12] |
Langham J, Barut V, Samnaliev M, et al. Disease severity, flares and treatment patterns in adults with systemic lupus erythematosus in the UK: a real-world observational retrospective cohort analysis[J]. Rheumatol Adv Pract, 2021, 5(3): rkab061. DOI:10.1093/rap/rkab061 |
| [13] |
Chung YK, Ho LY, Lee C, et al. Validation of the 2019 EULAR/ACR classification criteria for systemic lupus erythematosus in ANA-positive Chinese patients[J]. Ther Adv Musculoskelet Dis, 2022, 14: 1759720x221100300. DOI:10.1177/1759720X221100300 |
| [14] |
Smith EMD, Rasul S, Ciurtin C, et al. Limited sensitivity and specificity of the ACR/EULAR-2019 classification criteria for SLE in JSLE?—observations from the UK JSLE Cohort Study[J]. Rheumatology, 2021, 60(11): 5271-5281. DOI:10.1093/rheumatology/keab210 |
| [15] |
Rees F, Doherty M, Grainge MJ, et al. The worldwide incidence and prevalence of systemic lupus erythematosus: a systematic review of epidemiological studies[J]. Rheumatology (Oxford), 2017, 56(11): 1945-1961. DOI:10.1093/rheumatology/kex260 |
| [16] |
Arnaud L, Fagot JP, Mathian A, et al. Prevalence and incidence of systemic lupus erythematosus in France: a 2010 nation-wide population-based study[J]. Autoimmun Rev, 2014, 13(11): 1082-1089. DOI:10.1016/j.autrev.2014.08.034 |
| [17] |
Naleway AL, Davis ME, Greenlee RT, et al. Epidemiology of systemic lupus erythematosus in rural Wisconsin[J]. Lupus, 2005, 14(10): 862-866. DOI:10.1191/0961203305lu2182xx |
| [18] |
Fatoye F, Gebrye T, Svenson LW. Real-world incidence and prevalence of systemic lupus erythematosus in Alberta, Canada[J]. Rheumatol Int, 2018, 38(9): 1721-1726. DOI:10.1007/s00296-018-4091-4 |
| [19] |
Li S, Gong T, Peng Y, et al. Prevalence and incidence of systemic lupus erythematosus and associated outcomes in the 2009-2016 US Medicare population[J]. Lupus, 2020, 29(1): 15-26. DOI:10.1177/0961203319888691 |
| [20] |
Gonzalez Lucero L, Barbaglia AL, Bellomio VI, et al. Prevalence and incidence of systemic lupus erythematosus in Tucumán, Argentina[J]. Lupus, 2020, 29(13): 1815-1820. DOI:10.1177/0961203320957719 |
| [21] |
Magro R, Borg AA. Characterisation of patients with systemic lupus erythematosus in Malta: a population based cohort cross-sectional study[J]. Biomed Res Int, 2018, 2018, 2385386. DOI:10.1155/2018/2385386 |
| [22] |
Gergianaki I, Fanouriakis A, Repa A, et al. Epidemiology and burden of systemic lupus erythematosus in a Southern European population: data from the community-based lupus registry of Crete, Greece[J]. Ann Rheum Dis, 2017, 76(12): 1992-2000. DOI:10.1136/annrheumdis-2017-211206 |
| [23] |
Kameda S. Epidemiologic study of systemic lupus erythematosus in Fukuoka population[J]. Fukuoka Igaku Zasshi, 1988, 79(8): 571-578. |
| [24] |
Al Dhanhani AM, Agarwal M, Othman YS, et al. Incidence and prevalence of systemic lupus erythematosus among the native Arab population in UAE[J]. Lupus, 2017, 26(6): 664-669. DOI:10.1177/0961203316678677 |
| [25] |
Izmirly PM, Wan I, Sahl S, et al. The incidence and prevalence of systemic lupus erythematosus in New York County (Manhattan), New York: the Manhattan lupus surveillance program[J]. Arthritis Rheumatol, 2017, 69(10): 2006-2017. DOI:10.1002/art.40192 |
| [26] |
Barber MRW, Drenkard C, Falasinnu T, et al. Global epidemiology of systemic lupus erythematosus[J]. Nat Rev Rheumatol, 2021, 17(9): 515-532. DOI:10.1038/s41584-021-00668-1 |
| [27] |
Rees F, Doherty M, Grainge M, et al. The incidence and prevalence of systemic lupus erythematosus in the UK, 1999-2012[J]. Ann Rheum Dis, 2016, 75(1): 136-141. DOI:10.1136/annrheumdis-2014-206334 |
| [28] |
Hermansen ML, Lindhardsen J, Torp-Pedersen C, et al. Incidence of systemic lupus erythematosus and lupus nephritis in Denmark: a nationwide cohort study[J]. J Rheumatol, 2016, 43(7): 1335-1339. DOI:10.3899/jrheum.151221 |
| [29] |
Ruiz-Irastorza G, Khamashta MA, Castellino G, et al. Systemic lupus erythematosus[J]. Lancet, 2001, 357(9261): 1027-1032. DOI:10.1016/S0140-6736(00)04239-2 |
| [30] |
Pons-Estel GJ, Alarcón GS, Scofield L, et al. Understanding the epidemiology and progression of systemic lupus erythematosus[J]. Semin Arthritis Rheum, 2010, 39(4): 257-268. DOI:10.1016/j.semarthrit.2008.10.007 |
| [31] |
Vilar MJ, Sato EI. Estimating the incidence of systemic lupus erythematosus in a tropical region (Natal, Brazil)[J]. Lupus, 2002, 11(8): 528-532. DOI:10.1191/0961203302lu244xx |
| [32] |
Scolnik M, Marin J, Valeiras SM, et al. Incidence and prevalence of lupus in Buenos Aires, Argentina: a 11-year health management organisation-based study[J]. Lupus Sci Med, 2014, 1(1): e000021. DOI:10.1136/lupus-2014-000021 |
| [33] |
Naleway AL, Davis ME, Greenlee RT, et al. Epidemiology of systemic lupus erythematosus in rural Wisconsin[J]. Lupus, 2005, 14(10): 862-866. DOI:10.1191/0961203305lu2182xx |
| [34] |
Somers EC, Thomas SL, Smeeth L, et al. Incidence of systemic lupus erythematosus in the United Kingdom, 1990-1999[J]. Arthritis Rheum, 2007, 57(4): 612-618. DOI:10.1002/art.22683 |
| [35] |
Alamanos Y, Voulgari PV, Siozos C, et al. Epidemiology of systemic lupus erythematosus in northwest Greece 1982-2001[J]. J Rheumatol, 2003, 30(4): 731-735. |
| [36] |
Tsokos GC. Systemic lupus erythematosus[J]. N Engl J Med, 2011, 365(22): 2110-2121. DOI:10.1056/NEJMra1100359 |