 2023, Vol. 44
2023, Vol. 44文章信息
- 谢莉, 肖琳.
- Xie Li, Xiao Lin
- 呼出气一氧化碳检测在戒烟门诊中的开展情况及对患者戒烟意愿和戒烟行为的影响
- Performance of exhaled carbon monoxide measurement in smoking cessation clinics and its influence on patients' willingness and behavior for smoking cessation
- 中华流行病学杂志, 2023, 44(7): 1063-1067
- Chinese Journal of Epidemiology, 2023, 44(7): 1063-1067
- http://dx.doi.org/10.3760/cma.j.cn112338-20220930-00836
-
文章历史
收稿日期: 2022-09-30




吸烟是可预防的导致早死的主要原因[1]。有充分证据表明,吸烟能导致呼吸疾病、恶性肿瘤、心脑血管疾病和糖尿病等全身多系统疾病[2]。烟草烟雾中有7 000余种化学物质[1],如尼古丁、焦油、氰化氢、亚硝胺、一氧化碳和多环芳烃等,这些化学物质被吸入并分布到全身各个器官。其中一氧化碳在吸入呼吸道的肺泡后进入血液循环,与红细胞中的血红蛋白结合,形成碳氧血红蛋白。在身体停止吸入一氧化碳后,碳氧血红蛋白解离,一氧化碳通过肺排出。由于一氧化碳与血红蛋白的亲和力比氧气高200~240倍,暴露于一氧化碳会导致组织缺氧,使细胞受损[3]。通过特定的生化标志物,如血液中的可替宁等水平测定可用于评估吸烟状态。但血液检查为侵入性且价格较高。研究发现,测量呼出气一氧化碳水平是评估吸烟状态较为简单、有效的途径,且由于无创、价格相对较低,被全球广泛应用于评估患者吸烟状态[4-7]。
我国烟草流行形势严峻,并带来了严重的疾病负担,2018年中国成年人吸烟率为26.6%,吸烟人数达3.06亿[8]。2019年我国烟草归因死亡人数达270万[9]。由于烟草依赖是一种慢性病[10],《国际疾病分类》第十版(ICD-10)编码为F17.2,我国基本公共卫生项目(原中央补助地方项目)自2014年开始要求各省份每年选择≥3家医院提供戒烟服务。截至目前,项目已在全国支持了几百家戒烟门诊的创建;项目医院戒烟门诊需配备呼出气一氧化碳检测仪对患者开展检查,以帮助其更好地戒烟。本研究旨在探索呼出气一氧化碳检测在我国戒烟门诊中的开展情况及对患者戒烟意愿和戒烟行为的影响,为相关政策提供参考。
资料与方法1. 资料来源: 来源于基本公共卫生项目戒烟门诊数据管理平台,选取2019-2021年,257家配备呼出气一氧化碳检测仪的项目医院戒烟的患者数据。纳入标准:≥18周岁;首诊时仍处于吸烟状态的患者。
2. 研究方法:
(1) 戒烟干预流程:医生询问并记录患者信息,进行行为心理学干预,测量身高、体重、呼出气一氧化碳值后,询问患者的戒烟意愿并与患者共同约定戒烟日和下次随访时间。根据患者的意愿和尼古丁依赖程度开具戒烟药物(酒石酸伐尼克兰、盐酸安非他酮、尼古丁替代产品等),帮助患者克服戒断症状。首诊后1、3个月时开展电话随访,了解戒烟情况。
(2) 呼出气一氧化碳检测:首诊时,患者在医生的指导下用力吸气并屏气15~20 s,接着对着检测仪用力呼气,通过检测仪上的读数(定量)或显色(非定量)判断患者的吸烟状态[11]。一般认为,定量检测结果显示0~ ppm为非吸烟者,5~ ppm为偶尔吸烟者,7~ ppm为吸烟者,11~ ppm为经常吸烟者,16~25 ppm为吸烟成瘾者[12]。非定量检测结果通过显色不同,将检测对象分为轻、中、重度吸烟者。由于项目医院使用的呼出气一氧化碳检测仪既有定量也有非定量,本研究仅分为检测和未检测。
3. 指标和定义: 东部地区包括北京、上海、天津、河北、辽宁、江苏、浙江、福建、山东、广东、海南;中部地区包括山西、吉林、黑龙江、安徽、江西、河南、湖北、湖南;西部地区包括四川、重庆、贵州、云南、西藏、陕西、甘肃、青海、宁夏、新疆、广西、内蒙古。非雇佣职业包括退休、学生、无业;雇佣职业包括政府/事业单位、企业、务农、教师和医务人员。
干预时,医生同时询问并记录患者性别、年龄、职业、文化程度、每日吸烟量、吸烟年限、戒烟意愿等情况,利用尼古丁依赖检测量表衡量患者尼古丁依赖程度(0~分为尼古丁低依赖,4~分为中度依赖,≥7分为高度依赖)。
患者完成首诊时被询问“在过去30 d,你是否吸过烟”时,若回答“每天吸”“偶尔吸”,定义为处于吸烟状态;若回答“没有吸过”,定义为患者未处于吸烟状态。患者完成首诊时被询问“准备什么时候戒烟”时,若回答“会在就诊当天戒烟”“会在7 d内开始戒烟”“会在30 d内开始戒烟”,定义为强戒烟意愿;若回答“会在6个月内开始戒烟”“会在6个月后开始戒烟”“未决定何时戒烟”,定义为弱戒烟意愿。进行首诊后1、3个月随访时,若患者自报在过去的≥7 d内未吸烟,定义为1、3个月随访时戒烟。失访患者在本研究中被视为未戒烟状态。戒烟率为戒烟人数与初始随访人数的比值。
4. 统计学分析: 采用SPSS 22.0软件分析数据,定量资料采用x±s描述,定性资料采用构成比或比例或率(%)描述,组间比较采用χ2检验。分析呼出气一氧化碳检测对患者戒烟意愿和戒烟率的影响时,采用logistic回归模型估计OR值及其95%CI。双侧检验,检验水准α=0.05。
结果1. 基本情况: 共纳入41 566名患者,其中96.6%为男性,女性仅占3.4%。患者年龄为(50.3±14.8)岁,吸烟年限为(24.4±13.6)年,每日吸烟量(18.7±11.4)支。尼古丁依赖程度低、中、高分别为14 884名(35.8%)、16 599名(39.9%)、10 083名(24.3%)。非雇佣职业28 254名(68.0%),雇佣职业13 312名(32.0%)。文化程度以中学居多,共19 256名(46.4%),其次为大专及以上(11 989名,28.8%)和小学及以下(10 321名,24.8%)。见表 1。
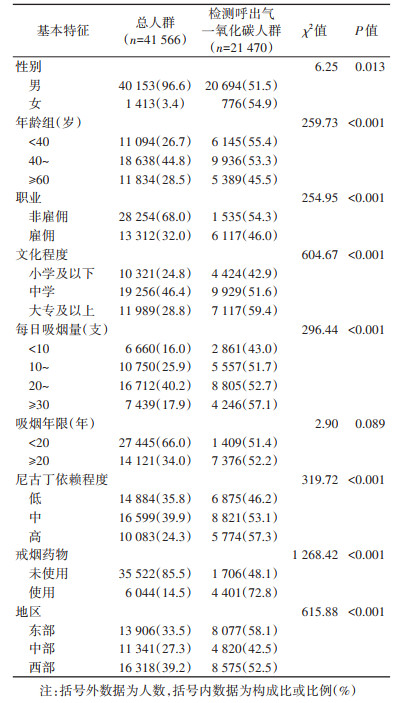
2. 呼出气一氧化碳检测情况: 首诊时仅21 470名(51.7%)患者做了检测。不同特征患者的检测情况不尽相同,女性、年龄越小、非雇佣、文化程度越高、每日吸烟量越大,尼古丁依赖程度高、使用戒烟药物及东部地区的患者检测比例更高,差异均有统计学意义(P < 0.05)。见表 1。
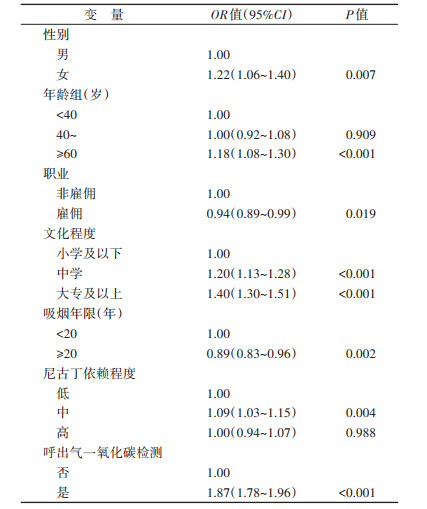
3. 呼出气一氧化碳检测与患者戒烟意愿: 完成呼出气一氧化碳检测的患者具有强戒烟意愿的比例为85.1%,高于未检测的患者(74.9%),差异有统计学意义(P < 0.001)。通过logistic回归分析控制可能影响因素(由于戒烟药物使用发生在患者首诊之后,因此在分析检测对戒烟意愿影响时未纳入该变量)后发现,检测呼出气一氧化碳的患者有强戒烟意愿的可能性是未检测患者的1.87(95%CI:1.78~1.96)倍,提示呼出气一氧化碳检测能够提高患者戒烟意愿。见表 2。
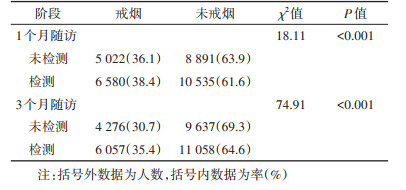
4. 呼出气一氧化碳检测与戒烟情况: 首诊后1个月项目医院对31 028名患者进行随访,其中28 851名应答并完成随访,应答率为93.0%;3个月随访22 941名患者,其中20 975名应答并完成随访,应答率为91.4%。完成随访人群与首诊人群人口学特征差异无统计学意义(P > 0.05)。首诊时检测过呼出气一氧化碳的患者1个月随访时戒烟率为38.4%,高于未检测患者(36.1%),差异有统计学意义(P < 0.001);3个月随访时戒烟率为35.4%,高于未检测患者(30.7%),差异有统计学意义(P < 0.001)。见表 3。
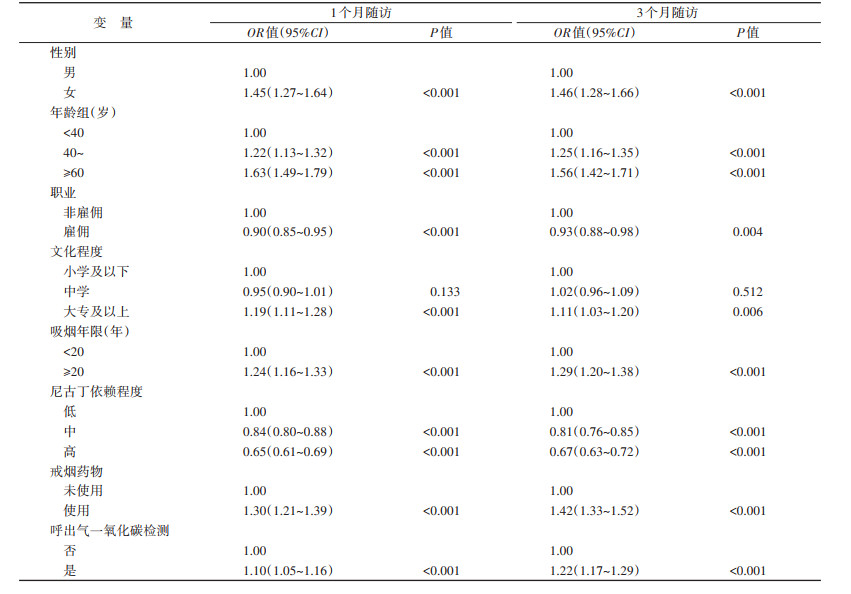
通过logistic回归分析控制可能影响因素后发现,首诊时检测呼出气一氧化碳的患者在1个月随访时戒烟的可能性是未检测患者的1.10(95%CI:1.05~1.16)倍,3个月随访时戒烟的可能性是未检测患者的1.22(95%CI:1.17~1.29)倍。提示呼出气一氧化碳检测能影响患者戒烟行为。见表 4。
既往研究充分证明了呼出气一氧化碳检测的重要性,可与唾液或尿中的可替宁检测互补,被用于临床验证吸烟者的戒烟情况[13-14]、评估患者的依从性[15-16]及戒烟和控烟项目的有效性[17]。本研究发现,检测呼出气一氧化碳的患者,愿意在30 d或更短时间内戒烟的意愿高于未检测的患者,与2019年测定骨科创伤患者呼出气一氧化碳值能提高其戒烟意愿的研究结果一致[18]。患者对呼出气一氧化碳检测仪及其读数感兴趣,并对身体一氧化碳值超标结果表示担忧,可能是更容易下决心戒烟的原因。
另外,本研究发现若患者在首诊时检测呼出气一氧化碳,1、3个月随访时戒烟率高于未检测的患者,类似研究在国内外尚未见报道,仅有呼出气一氧化碳值与戒烟比例的定量关系研究[19-20],但由于本研究中部分戒烟门诊只有定性检测结果,不能确定两者间的定量关系。
本研究配备检测仪的医院,仅一半左右的患者开展了检测,可能由于检测仪未进入医保目录,医院需自付检测项目费用[21],检测仪吹嘴造成的耗材支出可能影响医务人员使用积极性,因此部分医务人员只倾向于让尼古丁依赖程度高的患者检测。
鉴于呼出气一氧化碳的检测对提高戒烟意愿和戒烟行为的影响,建议戒烟门诊配备检测仪,医院对耗材给予必要支持,医务人员向患者解释检测的重要性,提高设备使用率。此外,部分国家和地区开始研发基于手机和电脑的呼出气一氧化碳检测相关应用,如日本和美国研发的移动设备交互的呼出气一氧化碳检测应用程序,使用者在家即可测量和记录呼出气一氧化碳的浓度,与戒烟治疗结合时能显著提高长期戒烟率[22-23]。为提高呼出气一氧化碳检测的可及性和对戒烟效果的长期影响,与移动设备交互的检测应用研发已成为一种趋势,我国可加大在此领域的探索。
本研究存在局限性。由于本研究对象为仅选取了在配备检测仪医院就诊的患者,探索了已开展随访患者戒烟行为和首诊呼出气一氧化碳检测的关系,外推到所有患者时可能会有一定偏差。
利益冲突 所有作者声明无利益冲突
作者贡献声明 谢莉:研究设计与实施、数据分析、论文撰写;肖琳:研究设计与实施、论文修改、研究指导
| [1] |
Drope J, Schluger N, Cahn Z, et al. The tobacco atlas[R]. Atlanta: American Cancer Society and Vital Strategies, 2018.
|
| [2] |
中华人民共和国国家卫生健康委. 中国吸烟危害健康报告2020[R]. 北京: 中华人民共和国国家卫生健康委, 2021. National Health Commission of the People's Republic of China. Report on the health hazards of smoking in China 2020[R]. Beijing: National Health Commission of the People's Republic of China, 2021. |
| [3] |
Carel RS. Health aspects of air pollution[M]//Sher E. Handbook of air pollution from internal combustion engines. Boston: Academic Press.
|
| [4] |
Yoshida N, Baba Y, Kuroda D, et al. Clinical utility of exhaled carbon monoxide in assessing preoperative smoking status and risks of postoperative morbidity after esophagectomy[J]. Dis Esophagus, 2018, 31(9): doy024. DOI:10.1093/dote/doy024 |
| [5] |
Beaupre LA, Hammal F, Stiegelmar R, et al. A community-based pharmacist-led smoking cessation program, before elective total joint replacement surgery, markedly enhances smoking cessation rates[J]. Tob Induc Dis, 2020, 18: 78. DOI:10.18332/tid/126405 |
| [6] |
Coleman T, Cooper S, Thornton JG, et al. A randomized trial of nicotine-replacement therapy patches in pregnancy[J]. N Engl J Med, 2012, 366(9): 808-818. DOI:10.1056/NEJMoa1109582 |
| [7] |
Slaich B, Claire R, Emery J, et al. Comparison of saliva cotinine and exhaled carbon monoxide concentrations when smoking and after being offered dual nicotine replacement therapy in pregnancy[J]. Addiction, 2022, 117(3): 751-759. DOI:10.1111/add.15671 |
| [8] |
李新华. 2018中国成人烟草调查报告[M]. 北京: 人民卫生出版社, 2020. Li XH. 2018 China adult tobacco survey report[M]. Beijing: People's Medical Publishing House, 2020. |
| [9] |
GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1223-1249. DOI:10.1016/S0140-6736(20)30752-2 |
| [10] |
中华人民共和国国家卫生和计划生育委员会. 中国临床戒烟指南: 2015年版[M]. 北京: 人民卫生出版社, 2015. National Health and Family Planning Commission of the People's Republic of China. Chinese clinical guidelines for smoking cessation 2015[M]. Beijing: People's Medical Publishing House, 2015. |
| [11] |
Raiff BR, Faix C, Turturici M, et al. Breath carbon monoxide output is affected by speed of emptying the lungs: implications for laboratory and smoking cessation research[J]. Nicotine Tob Res, 2010, 12(8): 834-838. DOI:10.1093/ntr/ntq090 |
| [12] |
Al-Sheyab N, Kheirallah KA, Mangnall LJT, et al. Agreement between exhaled breath carbon monoxide threshold levels and self-reported cigarette smoking in a sample of male adolescents in Jordan[J]. Int J Environ Res Public Health, 2015, 12(1): 841-854. DOI:10.3390/ijerph120100841 |
| [13] |
Kim SS, Kim S, Gona PN, et al. Determining optimal cutoffs for exhaled carbon monoxide and salivary cotinine to identify smokers among Korean Americans in a smoking cessation clinical trial[J]. J Smok Cessat, 2021, 2021, 6678237. DOI:10.1155/2021/6678237 |
| [14] |
Secker-walker RH, Vacek PM, Flynn BS, et al. Exhaled carbon monoxide and urinary cotinine as measures of smoking in pregnancy[J]. Addict Behav, 1997, 22(5): 671-684. DOI:10.1016/S0306-4603(97)00013-0 |
| [15] |
Shi Y, Ehlers S, Hinds R, et al. Monitoring of exhaled carbon monoxide to promote preoperative smoking abstinence[J]. Health Psychol, 2013, 32(6): 714-717. DOI:10.1037/a0029504 |
| [16] |
Goettel M, Niessner R, Mueller D, et al. Metabolomic fingerprinting in various body fluids of a diet-controlled clinical smoking cessation study using a validated GC-TOF-MS metabolomics platform[J]. J Proteome Res, 2017, 16(10): 3491-3503. DOI:10.1021/acs.jproteome.7b00128 |
| [17] |
Nikkholgh A, Soleimani M, Torkaman-Boutorabi A, et al. Evaluation of smoking status: comparison of self-reports with exhaled carbon monoxide analysis in university students in the Islamic Republic of Iran[J]. East Mediterr Health J, 2021, 27(4): 321-326. DOI:10.26719/emhj.20.121 |
| [18] |
Matuszewski PE, Comadoll SM, Costales T, et al. Novel application of exhaled carbon monoxide monitors: smoking cessation in orthopaedic trauma patients[J]. J Orthop Trauma, 2019, 33(11): e433-438. DOI:10.1097/BOT.0000000000001558 |
| [19] |
Hashimoto R, Tomioka H, Wada T, et al. Outcomes and predictive factors for successful smoking cessation therapy in COPD patients with nicotine dependence[J]. Respir Investig, 2020, 58(5): 387-394. DOI:10.1016/j.resinv.2020.03.007 |
| [20] |
Jiménez-Ruiz CA, Lledó JFP, Guerrero AC, et al. Searching for phenotypes in smoking cessation treatment[J]. Int J Clin Pract, 2014, 68(12): 1530-1539. DOI:10.1111/ijcp.12490 |
| [21] |
国家医疗保障局. 国家医疗保障局关于«基本医疗保险医用耗材支付管理暂行办法(征求意见稿)»[EB/OL]. (2021-11-19)[2022-09-19]. http://www.nhsa.gov.cn/art/2021/11/19/art_113_7352.html.
|
| [22] |
Masaki K, Tateno H, Nomura A, et al. A randomized controlled trial of a smoking cessation smartphone application with a carbon monoxide checker[J]. npj Digit Med, 2020, 3: 35. DOI:10.1038/s41746-020-0243-5 |
| [23] |
Krishnan N, Elf JL, Chon S, et al. COach2Quit: a pilot randomized controlled trial of a personal carbon monoxide monitor for smoking cessation[J]. Nicotine Tob Res, 2019, 21(11): 1573-1577. DOI:10.1093/ntr/nty182 |