 2021, Vol. 42
2021, Vol. 42文章信息
- 戚家豪, 魏俊妮, 张振君, 东靓, 张丽, 董丽, 毛盈颖, 雷立健, 胡晓琴, 白文启.
- Qi Jiahao, Wei Junni, Zhang Zhenjun, Dong Liang, Zhang Li, Dong Li, Mao Yingying, Lei Lijian, Hu Xiaoqin, Bai Wenqi
- 他汀类药物与结直肠癌相关性的Meta分析
- A Meta-analysis on association between statins and colorectal cancer
- 中华流行病学杂志, 2021, 42(2): 343-350
- Chinese Journal of Epidemiology, 2021, 42(2): 343-350
- http://dx.doi.org/10.3760/cma.j.cn112338-20200119-00045
-
文章历史
收稿日期: 2020-01-19




2. 山西省肿瘤医院医务科, 太原 030001;
3. 太原市中心医院消化科 030001;
4. 浙江中医药大学公共卫生学院流行病学教研室, 杭州 310053;
5. 山西省肿瘤医院结直肠肛门外科, 太原 030001
2. Division of Medical Affairs, Shanxi Cancer Hospital, Taiyuan 030001, China;
3. Department of Gastroenterology, Taiyuan Central Hospital, Taiyuan 030001, China;
4. Department of Epidemiology, School of Public Health, Zhejiang Traditional Chinese Medical University, Hangzhou 310053, China;
5. Department of Colorectal and Anal Surgery, Shanxi Cancer Hospital, Taiyuan 030001, China
结直肠癌(colorectal cancer)是消化道最常见的恶性肿瘤,也是世界上常见肿瘤之一。在全球范围内,结直肠癌的发病率和死亡率分别位居世界第三和第二位[1]。在我国,结直肠癌发病率已上升至恶性肿瘤的第三位,每年新发病例超17万,且近年发病率呈明显上升趋势,新发病例数以每年4%的速度增长[2],已经成为危害我国居民健康的重大公共卫生问题。因此,探寻有效的结直肠癌预防措施成为该领域的研究热点。除了改善饮食结构和采用先进的早期诊断技术,药物预防也被认为是预防结直肠癌的有效措施之一。
他汀类药物是世界范围内使用非常广泛的一类药物[3],目前常用于高胆固醇血症患者、动脉粥样硬化性心血管疾病患者以及血脂异常人群[4]。一项基于改善中国心血管疾病护理项目(The Improving Care for Cardiovascular Disease in China Project)的研究共纳入6 523名急性冠状动脉患者,其中91.8%的患者接受了他汀类药物的治疗[5]。多项研究结果表明,他汀类药物对心血管疾病发病率和死亡率的一级和二级预防作用是有效的[6-7]。他汀类药物具有多效性,可能对癌症发生风险有影响,并在癌症的化学预防中发挥作用[8],但关于他汀类药物与结直肠癌的关系依然没有足够的证据来证实[9]。大量流行病学研究报道了他汀类药物与结直肠癌的关系,从风险降低47%至风险增加7%,结果不相一致。因此,本研究系统地检索了国内外数据库中关于他汀类药物与结直肠癌的相关研究并进行Meta分析,以评估他汀类药物与结直肠癌发生风险的相关性,从而为结直肠癌的预防提供循证医学依据。
资料与方法1. 文献检索:系统检索中国知网(CNKI)、万方数据知识服务平台(Wanfang data)、PubMed和Cochrane Library数据库中所有他汀类药物与结直肠癌研究的文献,检索时间自2000年1月至2020年1月。中文检索词:“他汀类药物”“阿托伐他汀”“辛伐他汀”“普伐他汀”“瑞舒伐他汀”“洛伐他汀”“结直肠癌”“结肠癌”“直肠癌”“结直肠肿瘤”。英文检索词为:“statins”“atorvastatin”“simvastatin”“pravastatin”“rosuvastatin”“lovastatin”“colorectal cancer”“colon cancer”“rectal cancer”“colorectal tumor”。此外,辅助采用文献追溯法,尽可能查找到相关文献。
2. 文献纳入排除标准:纳入标准:①文献内容涉及他汀类药物与结直肠癌发病风险相关性的研究;②文献研究类型为病例对照研究、队列研究或随机对照试验(randomized controlled trials,RCT)研究;③可直接或间接计算OR值或危险度比(RR)值及其95%CI。排除标准:①动物研究和细胞实验研究;②同一课题组重复文献,选取数据最新最全的一次报道;③综述类文献;④研究内容为结直肠癌预后。
3. 文献质量评价标准:病例对照研究和队列研究采用纽卡斯尔-渥太华(the Newcastle-Ottawa Scale,NOS)量表评价文章质量,NOS量表主要从3个方面进行评价:①研究人群的选择(4分);②组间的可比性(2分);③结果评价(3分)。总分共9分,0~4分为低质量研究,5~9分为高质量研究。RCT研究用Jadad评分量表进行评定,从随机化(4分)、盲法(2分)以及随访(1分)进行测评。总分7分,1~3分为低质量研究,4~7分为高质量研究。
4. 数据提取:由2名研究人员独立进行文献筛选、数据提取和质量评价工作,最终结果由2名研究人员交叉核对,意见不一致时,咨询第三方专家。提取文献数据:①文献的基本信息(包括发表刊物、第一作者、发表年份和地区);②研究类型;③纳入分析的研究对象类型、总例数、各组出现结直肠癌结局的频数;④使用他汀类药物的时间、剂量和种类;⑤研究效应指标:OR值、RR值及其95%CI。
5. 统计学分析:将纳入文献根据研究设计类型、药物服用时间和剂量、研究地区以及他汀类药物溶解性和种类进行亚组分析。合并效应值采用RR值及其95%CI表示。用I2衡量各研究间结果的异质性大小[10],当I2≤25%且P > 0.10,认为不存在异质性,选择固定效应模型进行分析;如果I2 > 25%且P < 0.10,则存在异质性,选择随机效应模型进行分析。采用敏感性分析来评价本次Meta分析结果的稳定性,逐一剔除各项研究,分析剔除前后合并效应值的差异,评价各项研究对总体研究结果的影响。采用Egger线性回归法评估发表偏倚,检验水准取双侧α=0.05。以上分析由Revman 5.0和Stata 12.1软件完成。
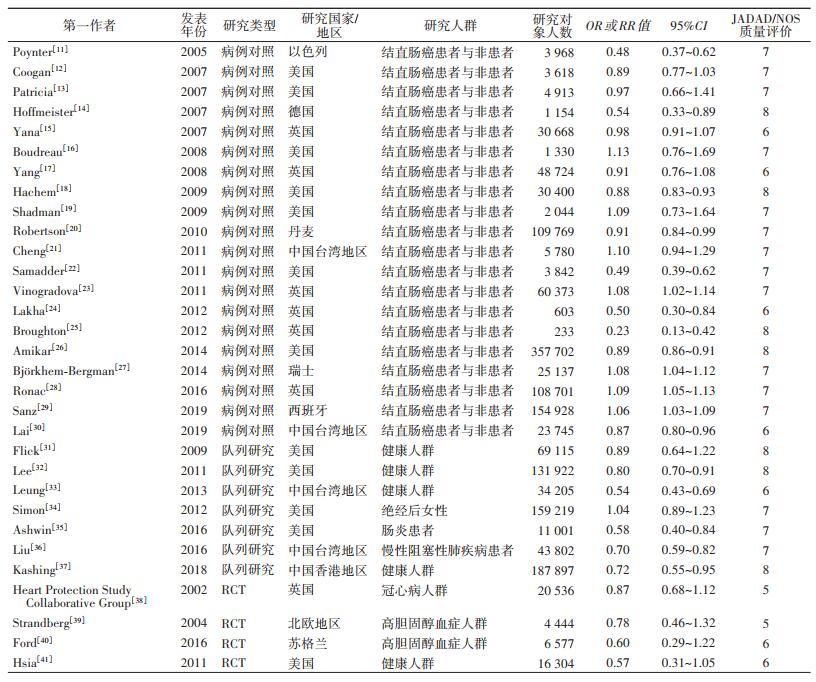
结果1. 纳入文献概况:共检索出相关文献1 424篇,经排除重复文献、与研究无关文献以及按照纳入排除标准筛除的文献,最终纳入31篇文献,其中病例对照研究20篇、队列研究7篇、RCT研究4篇(图 1)。文献涉及研究地区:美国(12篇)、英国(7篇)、德国(1篇)、西班牙(1篇)、苏格兰(1篇)、丹麦(1篇)、以色列(1篇)、瑞士(1篇)、北欧地区(1篇)、中国香港地区(1篇)、中国台湾地区(4篇)。纳入文献基本信息及质量评价见表 1。

|
| 图 1 文献检索及筛选流程 |
2. Meta分析:
(1)按研究类型分组:根据不同的研究类型分为病例对照研究、队列研究和RCT研究3组。病例对照研究和队列研究组的I2均 > 50%,故选择随机效应模型进行分析,结果显示服用他汀类药物可以降低结直肠癌发生风险(病例对照研究:RR=0.93,95%CI:0.88~0.98,P=0.005;队列研究:RR=0.75,95%CI:0.63~0.88,P < 0.001)。RCT组I2=0%,故使用固定效应模型。结果显示他汀类药物可降低结直肠癌发生风险(RR=0.79,95%CI:0.65~0.97,P=0.02)(图 2)。Egger检验结果表明各亚组存在发表偏倚可能性较低(病例对照:P=0.166;队列研究:P=0.386;RCT:P=0.758)(表 2)。

|
| 图 2 他汀类药物与结直肠癌关系的Meta分析 |

(2)按研究地区分组:将纳入研究按不同地区分为欧美和亚洲两组,结果显示,两组I2均 > 50%,故选择随机效应模型。欧美地区(RR=0.84,95%CI:0.77~0.91,P=0.001)和亚洲地区(RR=0.77,95%CI:0.62~0.92,P=0.001)的分析结果均表明他汀类药物可以降低结直肠癌发生风险。两组Egger检验的P值分别为0.421和0.227(表 2)。
(3)按服药年限分组:将报告他汀类药物服用时间的研究按照服用年限分为1、2、3和5年4个组别,分别进行Meta分析。其中服用年限 < 5年组(I2=80%,随机效应模型)的分析结果显示,他汀类药物对结直肠癌具有保护作用(RR=0.86,95%CI:0.76~0.96,P=0.001)。Egger检验的P值为0.062。其余亚组分析结果均无统计学意义(表 2)。
(4)按日均服用剂量分组:根据他汀类药物使用者每日服用药物的剂量分为低剂量组(< 34 mg)和高剂量组(≥34 mg)。两组I2均 > 50%,故选择随机效应模型进行分析,结果显示日均剂量≥34 mg对结直肠癌发生具有保护作用(RR=0.81,95%CI:0.66~0.98,P=0.001),Egger检验的P值为0.150(表 2)。
(5)按他汀类药物溶解性分组:根据他汀类药物的溶解性分为脂溶性他汀组和水溶性他汀组进行分析,结果显示脂溶性他汀可以降低结直肠癌发生风险(RR=0.86,95%CI:0.74~0.99,P=0.04),其I2=93.5%,故选择随机效应模型分析。Egger检验的P值为0.077(表 2)。
(6)按他汀类药物种类分组:根据他汀类药物的种类分为辛伐他汀、普伐他汀、阿托伐他汀、洛伐他汀和瑞舒伐他汀组进行分析。结果显示,不同种类他汀类药物都未表现出对结直肠癌明显的保护或危险作用。
3. 敏感性分析:敏感性分析结果显示,逐一排除各项研究所得结果均与原结果的RR值相近,表明本研究结果可靠、稳定(图 3)。

|
| 图 3 他汀类药物与结直肠癌关系的敏感性分析 |
4. 发表偏倚:本研究纳入文献时,严格遵循纳入排除标准。Egger检验结果未显示出偏倚的高可能性(表 2),漏斗图结果显示无明显不对称性(图 4)。

|
| 图 4 他汀类药物与结直肠癌关系的Meta分析漏斗图 |
他汀类药物所拥有的降胆固醇、调血脂以及延缓动脉粥样硬化等作用,已经在临床上广泛应用。近年来,越来越多的研究表明他汀类药物可能具有抵抗癌症的化学预防作用[42]。然而,关于他汀类药物与结直肠癌发生风险的研究结果尚存在争论,且人们对他汀类药物的安全性也存在顾虑[43]。
本研究Meta分析结果显示,服用他汀类药物对结直肠癌有一定保护作用(病例对照研究:RR=0.93;队列研究:RR=0.75;RCT:RR=0.79),有学者在大肠癌细胞系和动物模型中证实了该结论[44-45],他汀类药物可通过增加细胞内氧化应激反应[46]、诱导细胞凋亡[47]和抑制肿瘤转移[48]等途径来抑制结直肠癌的发生发展。进一步按服药时间、剂量、药物种类分组进行Meta分析,结果提示,服用他汀类药物 < 5年、日均剂量≥34 mg和脂溶性他汀均可降低结直肠癌发生风险,为预防性服用他汀类药物提供了建设性意见。Ronac等[28]的研究结果提示,服用他汀类药物至少1年以上才能表现出对结直肠癌的预防作用。关于预防性服用他汀类药物的服用时间、剂量、药物种类等还需要大量RCT研究提供更为可靠的数据。
既往研究表明阿司匹林对结直肠癌有预防作用,可是其高概率引起消化道出血等不良反应的副作用限制了它的广泛使用[49]。与阿司匹林相比,他汀类药物的耐受性较好,不良事件发生率低,有研究提出,他汀类药物治疗的益处远远大于任何可能存在的风险[50],但这并不代表没有风险。然而,本研究纳入的文献中只有2篇报道了他汀类药物产生的肌无力等肌肉症状的不良反应[37-38],无法对其安全性进行评估。因此,需要更多研究关注他汀类药物的不良反应。
本研究结论与2014年Lytras等[51]的Meta分析结论一致,即他汀类药物对结直肠癌有一定预防作用。与该文相比,本研究不仅更新了文献,对纳入文献质量进行评价,更重要的是对他汀类药物服用时间、剂量和药物种类进行了分组分析,从而为预防性服用他汀类药物提供了更为详实的参考依据。本研究纳入的研究间异质性较大,考虑其主要原因是不同研究对他汀类药物的使用标准不统一,如部分文献定义为他汀类药物6个月内至少处方2次[30, 34, 52],还有部分文献定义为服用他汀类药物 > 100 d[12, 31]。其次,本研究纳入研究的人群来自多个国家,研究对象的遗传背景差异较大,而遗传易感性在结直肠癌的患病中起着重要作用[53],且有研究表明基因多态性会改变他汀类药物对结直肠癌的预防作用[54]。尽管本研究按欧美地区(RR=0.84)和亚洲地区(RR=0.77)进行分组分析,仍未很好控制异质性。再者,他汀类药物的服用有明显的社会和经济差异[52, 55],社会经济地位较高的人更可能服用他汀类药物,这也是造成异质性的潜在因素之一。本研究Egger检验和漏斗图结果显示无明显的发表偏倚,敏感性分析结果较为稳定。
本研究存在局限性。首先,各研究间样本量差异较大,虽然整体结果较为稳定,但可能会影响亚组分析结果的稳定性;其次,纳入的文献大都来自欧美地区,其他地区的文献报道较少;再者,无法对原始文献中他汀类药物的累计剂量统一标准后进行分析,不能推断服用他汀类药物的累计剂量对结直肠癌的影响;此外,本次分析纳入的研究自2000年至今,对于2000年之前的文章未纳入分析;最后,纳入文献中仅有2篇报道他汀类药物的不良反应,无法评估长期服用他汀类药物的安全性。
综上所述,本次Meta分析结果提示,服用脂溶性他汀类药物 < 5年、日均剂量≥34 mg可降低结直肠癌发生风险。然而,由于缺少高质量的RCT研究,服用他汀类药物的不良反应报道较少,有关他汀类药物服用最佳剂量和疗程、长期服用他汀类药物的不良反应等内容,还需进一步研究,以便为预防性服用他汀类药物预防结直肠癌发生提供更为可靠详实的依据。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394-424. DOI:10.3322/caac.21492 |
| [2] |
Siegel Rl, Miller KD, Jemal A. Cancer statistics 2017[J]. CA Cancer J Clin, 2017, 67(1): 7-30. DOI:10.3322/caac.21387 |
| [3] |
Walley T, Folino-Gallo P, Schwabe U, et al. Variations and increase in use of statins across Europe: data from administrative databases[J]. BMJ, 2004, 328(7436): 385-386. DOI:10.1136/bmj.328.7436.385 |
| [4] |
诸骏仁, 高润霖, 赵水平, 等. 中国成人血脂异常防治指南(2016年修订版)[J]. 中国循环杂志, 2016, 31(10): 937-953. Zhu JR, Gao RL, Zhao SP, et al. Guidelines for the prevention and treatment of dyslipidemia in Chinese adults (revised edition, 2016)[J]. Chin J Circulation, 2016, 31(10): 937-953. DOI:10.3969/j.issn.1000-3614.2016.10.001 |
| [5] |
Xing YY, Liu J, Hao YC, et al. Prehospital statin use and low-density lipoprotein cholesterol levels at admission in acute coronary syndrome patients with history of myocardial infarction or revascularization: findingsfrom the improving care for cardiovascular disease in China (CCC) project[J]. Am Heart J, 2019, 212: 120-128. DOI:10.1016/j.ahj.2019.02.019 |
| [6] |
Oesterle A, Laufs U, Liao JK. Pleiotropic effects of statins on the cardiovascular system[J]. Circ Res, 2017, 120(1): 229-243. DOI:10.1161/CIRCRESAHA.116.308537 |
| [7] |
Lloyd-Jones D, Morris P, Ballantyne C, et al. 2017 focused update of the 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology T ask Force on Expert Consensus Decision Pathways[J]. J Am Coll Cardiol, 2017, 70(14): 1785-1822. DOI:10.1016/j.jacc.2017.07.745 |
| [8] |
Gazzerro P, Proto MC, Gangemi G, et al. Pharmacological actions of statins: a critical appraisal in the management of cancer[J]. Pharmacol Rev, 2012, 64(1): 102-146. DOI:10.1124/pr.111.004994 |
| [9] |
Jeong GH, Lee KH, Kim JY, et al. Effect of statin on cancer incidence: an umbrella systematic review and Metaanalysis[J/OL]. J Clin Med, 2019, 8(6): 819. DOI: 10.3390/jcm8060819.
|
| [10] |
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses[J]. BMJ, 2003, 327(7414): 557-560. DOI:10.1136/bmj.327.7414.557 |
| [11] |
Poynter JN, Gruber SB, Higgins PD, et al. Statins and the risk of colorectal cancer[J]. N Engl J Med, 2005, 352(21): 2184-2192. DOI:10.1056/NEJMoa043792 |
| [12] |
Coogan PF, Smith J, Rosenberg L. Statin use and risk of colorectal cancer[J]. J Natl Cancer Inst, 2007, 99(1): 32-40. DOI:10.1093/jnci/djk003 |
| [13] |
Patricia F, Lynn R, Brian L. Statin use and the risk of 10 cancers[J]. Epidemiology, 2007, 18(2): 213-219. DOI:10.1097/01.ede.0000254694.03027.a1 |
| [14] |
Hoffmeister M, Chang-Claude J, Brenner H. Individual and joint use of statins and low-dose aspirin and risk of colorectal cancer: a population-based case-control study[J]. Int J Cancer, 2007, 121(6): 1325-1330. DOI:10.1002/ijc.22796 |
| [15] |
Ya na, Hippisely CJ, Logan RF, et al. Risk of colorectal cancer in patients prescribed statins, nonsteroidal antiinflflammatory drugs, and cyclooxygenase-2 inhibitors: nested case-control study[J]. Gastroenterology, 2007, 133(2): 393-402. DOI:10.1053/j.gastro.2007.05.023 |
| [16] |
Boudreau DM, Koehler E, Rulyak SJ, et al. Cardiovascular medication use and risk for colorectal cancer[J]. Cancer Epidemiol Biomarkers Prev, 2008, 17(11): 3076-3080. DOI:10.1158/1055-9965 |
| [17] |
Yang YX, Hennessy S, Propert K, et al. Chronic statin therapy and the risk of colorectal cancer[J]. Pharmacoepid Drug Saf, 2008, 17(9): 869-876. DOI:10.1002/pds.1599 |
| [18] |
Hachem C, Morgan R, Johnson M, et al. Statins and the risk of colorectal carcinoma: a nested case-control study in veterans with diabetes[J]. Am J Gastroenterol, 2009, 104(5): 1241-1248. DOI:10.1038/ajg.2009.64 |
| [19] |
Shadman M, Newcomb PA, Hampton JM, et al. Nonsteroidal anti-inflammatory drugs and statins in relation to colorectal cancer risk[J]. World J Gastroenterol, 2009, 15(19): 2336-2339. DOI:10.3748/wjg.15.2336 |
| [20] |
Robertson DJ, Riis AH, Friis S, et al. Neither long-term statin use nor atherosclerotic disease is associated with risk of colorectal cancer[J]. Clin Gastroenterol Hepatol, 2010, 8(12): 1056-1061. DOI:10.1016/j.cgh.2010.08.010 |
| [21] |
Cheng MH, Chiu HF, Ho SC, et al. Statin use and the risk of colorectal cancer: a population-based case-control study[J]. World J Gastroenterol, 2011, 17(47): 5197-5202. DOI:10.3748/wjg.v17.i47.5197 |
| [22] |
Samadder J, Bhramar M, Huang SC, et al. Risk of colorectal cancer in self-reported inflammatory bowel disease and modification of risk by statin and NSAID use[J]. Cancer, 2011, 117(8): 1640-1648. DOI:10.1002/cncr.25731 |
| [23] |
Vinogradova Y, Coupland C, Hippisley-Cox J. Exposure to statins and risk of common cancers: a series of nested case-control studies[J/OL]. BMC Cancer, 2011, 11(1): 409. DOI: 10.1186/1471-2407-11-409.
|
| [24] |
Lakha F, Theodoratou E, Farrington SM, et al. Statin use and association with colorectal cancer survival and risk: case control study with prescription data linkage[J/OL]. BMC Cancer, 2012, 12(1): 487. DOI: 10.1186/1471-240712-487.
|
| [25] |
Broughton T, Sington J, Beales IL. Statin use is associated with a reduced incidence of colorectal cancer: a colonoscopy-controlled case-control study[J/OL]. BMC Gastroenterol, 2012, 12(1): 36. DOI: 10.1186/1471-230X-12-36.
|
| [26] |
Amikar Sehedev, Ya-chen T. The Role of Statins for Primary Prevention in Non-elderly Colorectal Cancer Patients[J]. Anticancer Res, 2014, 34(9): 5043-5050. DOI:10.1001/j.5043-50.2014 |
| [27] |
Björkhem-Bergman L, Backheden M, Löfdal KS. Statin treatment reduces the risk of hepatocellular carcinoma but not colon cancer-results from a nationwide case-control study in Sweden[J]. Pharmacoepid Drug Safety, 2014, 23(10): 1101-1106. DOI:10.1002/pds.3685 |
| [28] |
Ronac M, Lewis JD, Scott FI, et al.Disentangling the association between statins, cholesterol, and colorectal cancer: a nested case-control study[J/OL]. PLoS Med, 2016, 13(4): e1002007. DOI: 10.1371/journal.pmed.1002007.
|
| [29] |
Sanz G, Elisabet G, AnaGarcía R, et al. Statin use and the risk of colorectal cancer in a population-based electronic health records study[J/OL]. Scientific Reports, 2019, 9(1): 13560. DOI: 10.1038/s41598-019-49877-5.
|
| [30] |
Lai SW, Kuo Yh, Fang CW, et al. Statins therapy and colorectal cancer risk[J]. Nutr Metab Cardiovasc Dis, 2019, 29(12): 1429-1430. DOI:10.1016/j.numecd.2019.09.011 |
| [31] |
Flick ED, Habel LA, Chan KA, et al. Statin use and risk of colorectal cancer in a cohort of middle-aged men in the US: a prospective cohort study[J]. Drugs, 2009, 69(11): 1445-1457. DOI:10.2165/00003495-200969110-00004 |
| [32] |
Lee JE, Baba Y, Ng K, et al. Statin use and colorectal cancer risk according to molecular subtypes in two large prospective cohort studies[J]. Cancer Prev Res, 2011, 4(11): 1808-1815. DOI:10.1158/1940-6207.CAPR-11-0113 |
| [33] |
Leung HW, Chan AL, Lo D, et al. Common cancer risk and statins: a population-based cohort study in a Chinese population[J]. Expert Opin Drug Saf, 2013, 12(1): 19-27. DOI:10.1517/14740338.2013.744392 |
| [34] |
Simon MS, Rosenberg CA, Rodabough RJ, et al. Prospective analysis of association between use of statins or other lipid-lowering agents and colorectal cancer risk[J]. Ann Epidemiol, 2012, 22(1): 17-27. DOI:10.1016/j.annepidem.2011.10.006 |
| [35] |
Ashwin N, Ananthakrishnan, Andrew C, et al. Statin use is Associated With Reduced Risk of Colorectal Cancer in Patients with Inflammatory Bowel Diseases[J]. Clin Gastroenterol Hepatol, 2016, 14(7): 973-979. DOI:10.1016/j.cgh.2016.02.017 |
| [36] |
Liu JC, Hao WR, Hu YP, et al. Statins dose-dependently exert a significant chemopreventive effect on colon cancer in patients with chronic obstructive pulmonary disease: a population-based cohort study[J]. Oncotarget, 2016, 7(40): 65270-65283. DOI:10.18632/oncotarget.11263 |
| [37] |
Kashing C, Chen L, Chan EW, et al. Statins reduce the progression of non-advanced adenomas to colorectal cancer: a postcolonoscopy study in 187897 patients[J]. Gut gutjnl, 2018, 68(11): 1979-1985. DOI:10.1136/gutjnl2018-317714 |
| [38] |
Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20536 high-risk individuals: a randomised placebo-controlled trial[J]. Lancet, 2002, 360(9326): 7-22. DOI:10.1016/S0140-6736(02)09327-3 |
| [39] |
Strandberg TE, Pyörälä K, Cook TJ, et al. Mortality and incidence of cancer during 10-year follow-up of the Scandinavian Simvastatin Survival Study (4S)[J]. Lancet, 2004, 364(9436): 771-777. DOI:10.1016/S0140-6736(04)16936-5 |
| [40] |
Ford I, Murray H, Packard CJ, et al. Long-Term Safety and Efficacy of Low-Density Lipoprotein Cholesterol with Statin Therapy: 20-Year Follow-Up of West of Scotland Prevention Study[J]. Circulation, 2016, 133(11): 1073-1080. DOI:10.1161/CIRCULATIONAHA.115.019014 |
| [41] |
Hsia J, MacFadyen JG, Monyak J, et al. Cardiovascular event reduction and adverse events among subjects attaining low-density lipoprotein cholesterol < 50 mg/dl with rosuvastatin[J]. J Am Coll Cardiol, 2011, 57(16): 1666-1675. DOI:10.1016/j.jacc.2010.09.082 |
| [42] |
Zaleska M, Mozenska O, Bil J. Statins use and cancer: an update[J]. Future Oncol, 2018, 14(15): 1497-1509. DOI:10.2217/fon-2017-0543 |
| [43] |
Weverling-Rijnsburger AW, Blauw GJ, Lagaay AM, et al. Total cholesterol and risk of mortality in the oldest old[J]. Lancet, 1997, 350(9085): 1119-1123. DOI:10.1016/S01406736(97)04430-9 |
| [44] |
Notarnicola M, Messa C, Pricci M, et al. Up-regulation of 3-hydroxy-3-methylglutaryl coenzyme A reductase activity in left-sided human colon cancer[J]. Anticancer Res, 2004, 24(6): 3837-3838. DOI:10.1001/j.3837-38.2004 |
| [45] |
Narisawa T, Morotomi M, Fukaura Y, et al. Chemoprevention by pravastatin, a 3-hydroxy-3methylglutarylcoenzyme A reductase inhibitor, of N-methyl-N-nitrosourea-induced colon carcinogenesis in F344 rats[J]. Jpn J Cancer Res, 1996, 87(8): 798-804. DOI:10.1111/j.1349-7006.1996.tb02103.x |
| [46] |
Lim T, Lee I, Kim J, et al. Synergistic effect of simvastatin plus radiation in gastric cancer and colorectal cancer: Implications of BIRC5 and connective tissue growth factor[J]. Int J Radiat Oncol Biol Phys, 2015, 93(2): 316-325. DOI:10.1016/j.ijrobp.2015.05.023 |
| [47] |
Ishikawa S, Hayashi H, Kinoshita K, et al. Statins inhibit tumor progression via an enhancer of zeste homolog 2-mediated epigenetic alteration in colorectal cancer[J]. Int J cancer, 2014, 135(11): 2528-2536. DOI:10.1002/ijc.28672 |
| [48] |
Qi XF, Kin DH, Yoon YS, et al. Involvement of oxidative stress in simvastatin induced apoptosis of murine CT26 colon carcinoma cells[J]. Toxicol Lett, 2010, 199(3): 277-287. DOI:10.1016/j.toxlet.2010.09.010 |
| [49] |
Rutledge B, Desai P, Liu S, et al. The association between statins and colorectal cancer stage in the women's health initiative[J]. Mol Clin Oncol, 2019, 11(3): 252-258. DOI:10.392/moc.2019.1895 |
| [50] |
Adhyaru BB, Jacobson TA. Safety and efficacy of statin therapy[J]. Nat Rev Cardiol, 2018, 15(12): 757-769. DOI:10.1038/s41569-018-0098-5 |
| [51] |
Lytras T, Nikolopoulous G, Bonovas S. Statins and the risk of colorectal cancer: an updated systematic review and meta-analysis of 40 studies[J]. World J Gastroenterol, 2014, 20(7): 1858-1870. DOI:10.3748/wjg.v20.i7.1858 |
| [52] |
Thomsen RW, Johnsen SP, Olesen AV, et al. Socioeconomic gradient in use of statins among Danish patients: Population-based crosssectional study[J]. Br J Clin Pharmacol, 2005, 60(5): 534-542. DOI:10.1111/j.1365-2125.2005.02494.x |
| [53] |
Markowitz SD, Bertagnolli MM. Molecular origins of cancer: molecular basis of colorectal cancer[J]. N Engl J Med, 2009, 361(25): 2449-2460. DOI:10.1056/NEJMra0804588 |
| [54] |
Lipkin SM, Chao EC, Moreno V, et al. Genetic variation in 3-hydroxy-3-methylglutaryl CoA reductase modifies the chemopreventive activity of statins for colorectal cancer[J]. Cancer Prev Res (Phila), 2010, 3(5): 597-603. DOI:10.1158/1940-6207.CAPR-10-0007 |
| [55] |
Bonovas S, Sitaras NM. Statins and cancer risk: a confounded association[J]. Gastroenterology, 2009, 137(2): 740-746. DOI:10.1053/j.gastro.2009.02.088 |