
Effect of intensive pelvic floor muscle training assisted by sEMG-BF on pelvic floor function in patients with post-prostatectomy incontinence
-
摘要:
目的 探讨盆底表面肌电生物反馈(sEMG-BF)辅助的强化盆底肌训练(PFMT)对前列腺癌术后尿失禁(PPI)患者盆底功能的影响。
方法 采用前瞻性自身对照设计,便利抽样纳入2022年11月至2023年4月海军军医大学第一附属医院尿失禁护理门诊收治的PPI患者,接受为期3个月、由失禁专科护士主导的sEMG-BF联合PFMT干预。于基线(T0)及干预后4周(T4)、6周(T6)、8周(T8)、10周(T10)、12周(T12),通过24 h尿垫试验漏尿量与盆底表面肌电指标评估尿控及盆底肌功能,采用广义估计方程分析时序变化。
结果 共招募PPI患者113例,脱落10例,最终纳入103例。干预后漏尿量及盆底表面肌电参数总体变化显著,快速收缩阶段最大振幅自T4起显著提升(均
P <0.001),T8增幅最大;而前、后静息阶段平均振幅直至T8才显著降低(均P <0.05)。结论 sEMG-BF辅助的强化PFMT可有效促进PPI患者早期尿控恢复与盆底肌功能重建,且术后8~12周是强化干预的关键期。
Abstract:Objective To investigate the effect of intensive pelvic floor muscle training (PFMT) assisted by surface electromyographic biofeedback (sEMG-BF) on pelvic floor function in patients with post-prostatectomy incontinence (PPI).
Methods A prospective single-group pretest-posttest design was employed. Patients with PPI were recruited via convenience sampling from Urinary Incontinence Nursing Clinic at The First Affiliated Hospital of Naval Medical University between Nov. 2022 and Apr. 2023. All participants received a 3-month intensive PFMT program assisted by sEMG-BF, delivered by specialized incontinence nurses. Urinary incontinence and pelvic floor muscle function were assessed at baseline (T0) and at weeks 4 (T4), 6 (T6), 8 (T8), 10 (T10), and 12 (T12) using the 24-h pad test leakage weight and surface electromyography parameters. Generalized estimating equations were used to analyze temporal changes across time points.
Results A total of 113 patients were recruited, with 10 patients dropping out, resulting in a final inclusion of 103 patients. Both leakage weight and surface electromyography parameters showed significant overall improvement over time. The peak amplitude during the fast contraction phase increased significantly from T4 onward (all
P < 0.001), with the greatest gain observed at T8. In contrast, mean amplitudes during the pre- and post-rest phases did not decrease significantly until T8 (bothP < 0.05).Conclusion sEMG-BF-assisted intensive PFMT can effectively promote early urinary incontinence recovery and pelvic floor muscle function rehabilitation in PPI patients, with weeks 8-12 postoperatively representing a key therapeutic window.
-
根治性前列腺切除术是治疗局限性前列腺癌的主要方式,但手术过程中盆底组织及其支配神经可能会受损,影响患者盆底功能[1]。前列腺癌术后尿失禁(post-prostatectomy incontinence,PPI)是根治性前列腺切除术患者常见的并发症,其发生率因研究人群、评估时间和评估标准的不同而有较大差异(2%~60%)[2-3]。PPI不仅限制了患者的身体活动,还对其心理健康和生活质量产生负面影响,增加了家庭护理和医疗费用负担[4]。盆底肌肉训练(pelvic floor muscle training,PFMT)通过加强盆底肌肉的收缩来提升其强度,能够增强盆底的支撑力和尿道内的压力,对治疗PPI有效[5]。但目前尚不清楚PPI患者需要多大强度的PFMT才能实现症状最大的改善且持续,以及如何帮助患者实现这一目标。盆底表面肌电生物反馈(surface electromyographic biofeedback,sEMG-BF)作为强化PFMT的一种辅助手段,通过经肛门探头采集盆底肌肉运动时肌肉细胞膜去极化产生的电信号,客观、直接地评估训练过程中肌肉群的肌电激活[6]。该技术因其无创、无痛、可视化等优点,已成为评估盆底肌功能的“金标准”,并在前列腺癌术后盆底功能障碍患者中显示出良好的应用价值[7]。一项系统综述和meta分析显示,与单纯PFMT相比,sEMG-BF辅助的PFMT显著改善了患者尿失禁症状,主要体现在患者24 h尿垫使用量减少及生活质量提升[8]。PPI主要原因是手术导致尿道括约肌张力下降,而sEMG-BF辅助的PFMT能否客观、有效地改善患者盆底肌功能尚需进一步研究。为了评估强化的PFMT对PPI患者尿失禁康复水平和盆底功能恢复的效果,海军军医大学第一附属医院开展了一项前瞻性、自身对照临床研究,现报道如下。
1 对象和方法
1.1 研究对象
采用便利抽样法,选取2022年11月至2023年4月在海军军医大学第一附属医院尿失禁护理门诊收治的PPI患者作为研究对象。纳入标准:(1)由同一术者完成前列腺癌根治术;(2)意识清楚,无沟通障碍和认知障碍;(3)术前无尿失禁,术后拔除导尿管后1 h尿垫试验漏尿量>1 g[9];(4)尿失禁护理门诊随访满3个月且临床资料完整。排除标准:(1)合并其他恶性肿瘤或严重器质性疾病;(2)无法配合完成评估及治疗;(3)合并sEMG-BF治疗禁忌证,如植入心脏起搏器、癫痫、泌尿道急性感染、金属过敏。剔除标准:(1)生存时间<3个月;(2)病情急性加重或治疗期间发生不良事件;(3)主动退出本研究。本研究获得海军军医大学第一附属医院伦理委员会审批(CHEC2020-136),并在中国临床试验中心注册(ChiC-TR2200061350),所有研究对象知情同意且自愿参与本研究。
1.2 样本量的确定
基于盆底肌电评估中快速收缩阶段的最大收缩值进行样本量计算。采用单组样本重复测量的样本量计算方法[10],设定双侧检验α为0.05,1-β为80%,测量次数为6次。预实验结果显示,快速收缩阶段最大收缩值的均数为31.96 μV,标准差为2.8 μV,同一研究对象相邻2次测量值的相关系数均为0.7。根据研究假设,预期干预后快速收缩最大值可提升20%,使用PASS 15.0软件计算得到所需样本量为64例,考虑20%的失访率,最终确定本研究所需最小样本量为80例。
1.3 干预方法
由失禁专科护士提供一对一指导与监督,利用个性化sEMG-BF技术辅助PFMT,干预周期为3个月。
1.3.1 术前指导
在手术前3 d,责任护士向患者解释PPI的风险,并强调PFMT的重要性。指导患者使用排尿中断法准确定位盆底肌,并教授PFMT快法训练。患者需要放松身体,仅收缩盆底肌,每次收缩持续4 s后放松4 s为1次动作,每组动作重复32次,每天做5组,可以在不同体位和一天中的不同时间段进行[11]。患者需要连续训练3 d,并每天记录排尿情况直至手术。
1.3.2 出院教育
在患者出院前,失禁专科护士集中授课和答疑,讲解PPI的原因、症状、导尿管的自我护理,以及饮食和运动建议[12]。
1.3.3 居家康复
在术后拔除导尿管当天,专科护士强化PFMT教育内容,在患者掌握PFMT快法训练的基础上,教会患者慢法训练,即每次收缩持续8 s后放松8 s,同样每组32次。快法和慢法可交替进行,每天共做5组[11]。同时,向患者展示如何进行24 h尿垫试验并记录结果。
1.3.4 门诊强化
从拔除导尿管到术后3个月,患者在完成居家PFMT基础上接受门诊sEMG-BF治疗。治疗包括基于Glazer方案的盆底生物反馈训练及电刺激。盆底生物反馈训练旨在评估患者主动收缩时盆底肌肉功能状态,分为前静息阶段、快速收缩阶段、紧张收缩阶段、耐力收缩阶段和后静息阶段。患者根据语音提示完成各个训练阶段的评估。电刺激训练模块协助患者进行盆底肌肉被动收缩,治疗参数根据文献报道和盆底康复专家建议设定,包括频率30~50 Hz、脉冲宽度为200~300 μs、电流波升为0~30 s,以唤醒患者的本体感觉[13-14]。治疗强度为每周3次,每次30 min。
1.3.5 个性化反馈
专科护士根据患者盆底肌肉功能及尿失禁康复效果动态调整治疗方案。对于尚未熟练掌握PFMT方法的患者,治疗方案侧重于电刺激,辅以生物反馈训练。如果患者能够主动配合PFMT,则以生物反馈训练为主。若患者的快肌纤维收缩强度不足,将加强PFMT快法训练;若慢肌纤维收缩强度不足,则加强PFMT慢法训练。此外,患者每次训练后需在微信群中进行打卡并填写训练日志,记录训练内容与进度,以确保训练的连续性和有效性。
1.4 评价指标
分别于PPI患者术后拔除导尿管当日(基线水平,T0)及干预4周(T4)、6周(T6)、8周(T8)、10周(T10)、12周(T12)时收集相关资料,评价患者3个月内的尿失禁康复水平和盆底肌肉功能。
1.4.1 尿失禁康复水平采用PPI患者24
h尿垫试验的漏尿量作为尿失禁康复水平的评价指标。尿垫试验的重复性和准确性较高,可用于量化尿失禁的严重程度并评估患者康复治疗效果[9]。
1.4.2 盆底肌肉功能
采用Glazer盆底表面肌电指标评估盆底肌肉功能,护士记录各阶段的肌电值,包括前静息阶段平均振幅、快速收缩阶段最大振幅、紧张收缩阶段平均振幅、耐力收缩阶段平均振幅和后静息阶段平均振幅,这些指标能全面反映盆底肌肉的活动能力、耐力和功能状态[15]。
1.5 质量控制方法
所有参与本研究的护士均已获得失禁专科护士认证,具备相应的专业资格,且接受了课题组的专门培训。在门诊康复治疗过程中,如果患者在预定的随访日无法到访,护士将为其重新安排一个接近的时间。所有数据的录入和分析工作由2名研究生分别执行,并进行交叉核对以确保准确性。
1.6 统计学处理
应用SPSS 27.0软件对数据进行分析。符合正态分布的计量资料以x±s描述,不符合正态分布的计量资料以M(Q1,Q3)描述。考虑到重复测量数据存在组内相关性,本研究采用广义估计方程分析24 h尿垫试验漏尿量及盆底肌电参数在6个时间点上的变化趋势。若时间主效应具有统计学意义(P<0.05),则进一步采用Wald检验对各随访时间点与基线的边际均值差异进行两两比较,并进行Bonferroni法校正。检验水准(α)为0.05。
2 结果
2.1 研究对象的基线资料
本研究共招募PPI患者113例,剔除未能坚持完成3个月训练的6例患者及门诊随访脱落的4例患者,最终纳入103例,治疗依从性为91.2%,其间无不良事件发生。患者的平均年龄为(69.68±5.92)岁,平均BMI为(25.28±2.86)kg/m2;59例(57.3%)患有高血压,32例(31.1%)有糖尿病,59例(57.3%)有吸烟史。确诊时,前列腺特异性抗原水平为9.86(7.24,16.63)ng/mL;Gleason评分“3+3”占15.5%(16例),“3+4”占37.9%(39例),“4+3”占21.4%(22例),“4+4”占15.5%(16例),“≥9”占9.7%(10例)。
2.2 不同时间点PPI患者尿失禁症状的变化
广义估计方程分析结果显示,24 h尿垫试验漏尿量在6个时间点的变化有统计学意义(P<0.001),表明PPI患者的尿失禁症状随干预时间的延长发生显著变化(表 1)。与基线(T0)相比,漏尿量在T4、T6、T8、T10、T12时间点均减少(均P<0.001),且呈持续下降趋势(表 2、图 1)。
表 1 PPI患者不同时间点24 h漏尿量及盆底表面肌电参数的广义估计方程分析结果Table 1 Generalized estimating equation analysis of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time pointsOutcome measure Wald χ2 Degree of freedom P value 24-h pad test leakage weight 736.609 5 <0.001 Mean amplitude during pre-rest phase 40.088 5 <0.001 Peak amplitude during fast contraction phase 872.151 5 <0.001 Mean amplitude during tonic contraction phase 740.741 5 <0.001 Mean amplitude during endurance contraction phase 1 034.413 5 <0.001 Mean amplitude during post-rest phase 23.488 5 <0.001 PPI: Post-prostatectomy incontinence. 表 2 PPI患者各时间点24 h漏尿量及盆底表面肌电参数的变化分析结果Table 2 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients at each time pointTime point 24-h pad test leakage weight Time point Mean amplitude during pre-rest phase b (95%CI) SE Wald P value b (95%CI) SE Wald P value T0 0 T0 0 T4 -174.272 (-208.775, -139.769) 17.604 98.002 <0.001 T4 -0.122 (-0.441, 0.197) 0.162 0.565 >0.05 T6 -270.194 (-306.168, -234.220) 18.354 216.710 <0.001 T6 -0.183 (-0.562, 0.195) 0.193 0.900 >0.05 T8 -340.340 (-378.359, -302.321) 19.398 307.839 <0.001 T8 -0.357 (-0.671, -0.043) 0.160 4.962 <0.05 T10 -400.340 (-439.411, -361.269) 19.935 403.311 <0.001 T10 -0.499 (-0.829, -0.169) 0.168 8.782 <0.05 T12 -454.903 (-494.614, -415.192) 20.261 504.085 <0.001 T12 -0.510 (-0.841, -0.180) 0.169 9.151 <0.05 Intercept 473.786 (433.858, 513.715) 20.372 540.865 <0.001 Intercept 2.479 (2.147, 2.810) 0.169 214.482 <0.001 Time point Peak amplitude during fast contraction phase Time point Mean amplitude during tonic contraction phase b (95%CI) SE Wald P value b (95%CI) SE Wald P value T0 0 T0 0 T4 4.874 (3.284, 6.463) 0.811 36.113 <0.001 T4 2.441 (1.223, 3.659) 0.621 15.424 <0.001 T6 4.714 (3.290, 6.139) 0.727 42.060 <0.001 T6 6.659 (5.297, 8.020) 0.695 91.855 <0.001 T8 13.392 (11.833, 14.950) 0.795 283.645 <0.001 T8 5.859 (4.529, 7.190) 0.679 74.491 <0.001 T10 18.377 (16.739, 20.016) 0.836 483.297 <0.001 T10 10.691 (9.479, 11.902) 0.618 299.059 <0.001 T12 22.707 (21.180, 24.233) 0.779 850.040 <0.001 T12 14.387 (13.186, 15.588) 0.613 551.253 <0.001 Intercept 15.562 (14.450, 16.674) 0.567 752.437 <0.001 Intercept 13.661 (12.540, 14.782) 0.572 570.131 <0.001 Time point Mean amplitude during endurance contraction phase Time point Mean amplitude during post-rest phase b (95%CI) SE Wald P value b (95%CI) SE Wald P value T0 0 T0 0 T4 3.642 (2.608, 4.677) 0.528 47.621 <0.001 T4 0.155 (-0.373, 0.682) 0.269 0.330 >0.05 T6 7.791 (6.649, 8.934) 0.583 178.617 <0.001 T6 -0.353 (-0.759, 0.054) 0.207 2.889 >0.05 T8 12.407 (11.149, 13.664) 0.642 374.085 <0.001 T8 -0.464 (-0.884, -0.043) 0.215 4.665 <0.05 T10 15.410 (14.288, 16.532) 0.573 724.279 <0.001 T10 -0.545 (-0.975, -0.115) 0.220 6.170 <0.05 T12 17.557 (16.427, 18.686) 0.576 928.863 <0.001 T12 -0.562 (-1.016, -0.108) 0.232 5.895 <0.05 Intercept 11.366 (10.503, 12.229) 0.440 666.383 <0.001 Intercept 2.737 (2.312, 3.162) 0.217 159.473 <0.001 PPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively; b: Regression coefficient; 95%CI: 95% confidence interval; SE: Standard error. 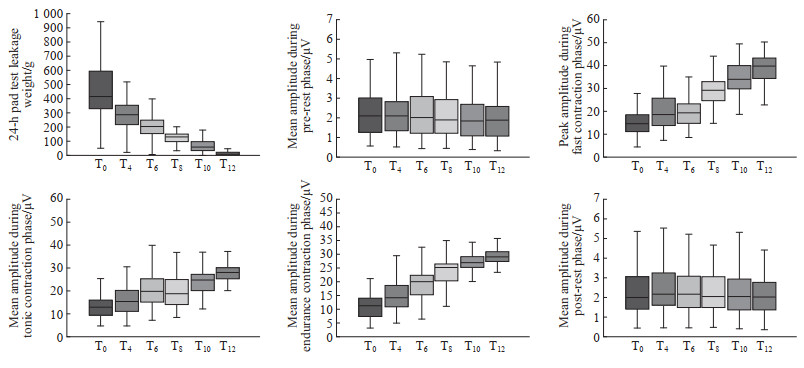 图 1 PPI患者24 h漏尿量及盆底表面肌电参数在不同时间点的变化趋势Fig. 1 Temporal trends of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time pointsPPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively.
图 1 PPI患者24 h漏尿量及盆底表面肌电参数在不同时间点的变化趋势Fig. 1 Temporal trends of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time pointsPPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively.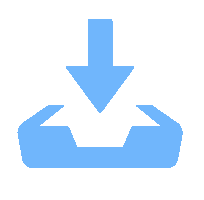 下载:
全尺寸图片
下载:
全尺寸图片
2.3 不同时间点PPI患者盆底表面肌电图参数的变化
不同时间点各阶段盆底表面肌电参数的变化显示盆底肌功能呈总体改善趋势(表 2,图 1),各指标两两比较的结果见图 2。
 图 2 PPI患者各时间点24 h漏尿量及盆底表面肌电参数两两比较的显著性热图Fig. 2 Heatmap of statistical significance for pairwise comparisons of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time pointsA: 24-h pad test leakage weight; B: Mean amplitude during pre-rest phase; C: Peak amplitude during fast contraction phase; D: Mean amplitude during tonic contraction phase; E: Mean amplitude during endurance contraction phase; F: Mean amplitude during post-rest phase. PPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively.下载:
全尺寸图片
图 2 PPI患者各时间点24 h漏尿量及盆底表面肌电参数两两比较的显著性热图Fig. 2 Heatmap of statistical significance for pairwise comparisons of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time pointsA: 24-h pad test leakage weight; B: Mean amplitude during pre-rest phase; C: Peak amplitude during fast contraction phase; D: Mean amplitude during tonic contraction phase; E: Mean amplitude during endurance contraction phase; F: Mean amplitude during post-rest phase. PPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively.下载:
全尺寸图片
2.3.1 前静息阶段肌电平均振幅的变化
T4和T6时间点的前静息阶段平均振幅与基线相比差异无统计学意义(均P>0.05),自T8时间点起降低。见表 2、图 1。
2.3.2 快速收缩阶段肌电最大振幅的变化
T4、T6、T8、T10、T12时间点的快速收缩阶段最大振幅均较基线升高(均P<0.001),呈持续增高趋势。见表 2、图 1。
2.3.3 紧张收缩阶段肌电平均振幅的变化
T4、T6、T8、T10、T12时间点的紧张收缩阶段平均振幅均高于基线(均P<0.001),呈上升趋势。见表 2、图 1。
2.3.4 耐力收缩阶段肌电平均振幅的变化
T4、T6、T8、T10、T12时间点的耐力收缩阶段平均振幅均高于基线(均P<0.001),呈持续增高趋势。见表 2、图 1。
2.3.5 后静息阶段肌电平均振幅的变化
T4和T6时间点的后静息阶段平均振幅与基线相比差异无统计学意义(均P>0.05),T8、T10、T12时间点降低(均P<0.05)。见表 2、图 1。
3 讨论
3.1 sEMG-BF辅助训练对术后尿控恢复及盆底肌功能的双重促进作用
PFMT的有效性取决于患者锻炼的频率、持续时间和依从性,并且护士在患者康复训练中起着重要作用[16]。本研究结果显示,患者基线盆底肌力处于较低水平,经失禁专科护士主导的强化干预后,不仅24 h尿垫试验漏尿量从基线至T12时间点持续减少(均P<0.001),快速收缩、紧张收缩及耐力收缩阶段肌电参数亦有所提升(均P<0.001)。分析其强化效应的原因包括:(1)治疗师利用生物反馈技术从锻炼技巧、力量和时间方面指导患者精确地进行肌肉收缩,并提供全程的教育和激励;(2)基于Glazer盆底表面肌电的动态评估数据,专科护士及时调整训练强度,制定个体化训练方案;(3)生物反馈方式符合健康行为改变理论,通过增强患者与治疗师的有效互动,提升了患者的自我效能感[17]。值得注意的是,漏尿量在T4(干预4周)即出现显著下降,提示该方案具有早期康复优势。本研究结果与韩国学者Oh等[18]的随机对照研究结果一致,其干预组采用便携式生物反馈装置,术后1个月尿控功能显著优于传统口头指导组。因此,盆底肌电生物反馈技术通过提升训练精准性与可及性,能有效加速早期康复进程。未来临床实践可探索以院内专科护士为主导、联合院外便携设备延续的尿控康复管理模式,既保障训练质量,又提高了患者参与便利性。
3.2 盆底肌功能恢复时序及盆底肌电参数的临床解读
本研究结果显示,前、后静息阶段平均振幅在干预8周前(T4、T6)与基线相比差异无统计学意义(均P>0.05),T8~T12显著降低;而快速收缩阶段最大振幅在T4即显著提升,且T8增幅最为明显,表明盆底肌主动收缩功能的恢复早于肌张力调节功能,且术后8~12周是盆底功能恢复的关键期。既往研究表明,生物反馈、电刺激及PFMT联合疗法在前列腺癌根治术后3个月内尿控功能改善显著,但对远期(≥6个月)尿控能力的影响较小[18-19]。本研究的干预周期为3个月,其间患者漏尿量持续下降且盆底表面肌电参数显著改善,证实了强化干预的有效性,然而关于远期治疗效果的评估仍需进一步研究。本研究发现,尽管患者盆底肌电收缩参数持续提升,但在12周时仍未达到设备参考值(快速收缩阶段最大振幅45~75 µV、紧张收缩阶段平均振幅35~45 µV)。分析原因,现行肌电评估参考标准基于Glazer协议[20],其参考人群为欧美小样本数据,难以直接适用于中国前列腺癌术后患者。因此,在临床实践中应关注患者个体基线提升幅度,构建针对男性群体的多维肌电图数据库,以得出适用中国人群的Glazer参数参考范围。
综上所述,盆底sEMG-BF辅助强化PFMT可显著改善前列腺癌术后患者的尿控症状并提升盆底肌功能,且术后8~12周为关键恢复期。本研究证实3个月专科护士主导的sEMG-BF联合PFMT干预具有良好的短期疗效,但远期效果仍需进一步研究。未来应结合远程技术优化院外延续管理,并建立适用于中国男性患者的表面肌电评估标准。
-
图 1 PPI患者24 h漏尿量及盆底表面肌电参数在不同时间点的变化趋势
Fig. 1 Temporal trends of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time points
PPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively.
下载:
全尺寸图片
图 2 PPI患者各时间点24 h漏尿量及盆底表面肌电参数两两比较的显著性热图
Fig. 2 Heatmap of statistical significance for pairwise comparisons of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time points
A: 24-h pad test leakage weight; B: Mean amplitude during pre-rest phase; C: Peak amplitude during fast contraction phase; D: Mean amplitude during tonic contraction phase; E: Mean amplitude during endurance contraction phase; F: Mean amplitude during post-rest phase. PPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively.
下载:
全尺寸图片
表 1 PPI患者不同时间点24 h漏尿量及盆底表面肌电参数的广义估计方程分析结果
Table 1 Generalized estimating equation analysis of 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients across time points
Outcome measure Wald χ2 Degree of freedom P value 24-h pad test leakage weight 736.609 5 <0.001 Mean amplitude during pre-rest phase 40.088 5 <0.001 Peak amplitude during fast contraction phase 872.151 5 <0.001 Mean amplitude during tonic contraction phase 740.741 5 <0.001 Mean amplitude during endurance contraction phase 1 034.413 5 <0.001 Mean amplitude during post-rest phase 23.488 5 <0.001 PPI: Post-prostatectomy incontinence. 表 2 PPI患者各时间点24 h漏尿量及盆底表面肌电参数的变化分析结果
Table 2 24-h pad test leakage weight and pelvic floor surface electromyography parameters in PPI patients at each time point
Time point 24-h pad test leakage weight Time point Mean amplitude during pre-rest phase b (95%CI) SE Wald P value b (95%CI) SE Wald P value T0 0 T0 0 T4 -174.272 (-208.775, -139.769) 17.604 98.002 <0.001 T4 -0.122 (-0.441, 0.197) 0.162 0.565 >0.05 T6 -270.194 (-306.168, -234.220) 18.354 216.710 <0.001 T6 -0.183 (-0.562, 0.195) 0.193 0.900 >0.05 T8 -340.340 (-378.359, -302.321) 19.398 307.839 <0.001 T8 -0.357 (-0.671, -0.043) 0.160 4.962 <0.05 T10 -400.340 (-439.411, -361.269) 19.935 403.311 <0.001 T10 -0.499 (-0.829, -0.169) 0.168 8.782 <0.05 T12 -454.903 (-494.614, -415.192) 20.261 504.085 <0.001 T12 -0.510 (-0.841, -0.180) 0.169 9.151 <0.05 Intercept 473.786 (433.858, 513.715) 20.372 540.865 <0.001 Intercept 2.479 (2.147, 2.810) 0.169 214.482 <0.001 Time point Peak amplitude during fast contraction phase Time point Mean amplitude during tonic contraction phase b (95%CI) SE Wald P value b (95%CI) SE Wald P value T0 0 T0 0 T4 4.874 (3.284, 6.463) 0.811 36.113 <0.001 T4 2.441 (1.223, 3.659) 0.621 15.424 <0.001 T6 4.714 (3.290, 6.139) 0.727 42.060 <0.001 T6 6.659 (5.297, 8.020) 0.695 91.855 <0.001 T8 13.392 (11.833, 14.950) 0.795 283.645 <0.001 T8 5.859 (4.529, 7.190) 0.679 74.491 <0.001 T10 18.377 (16.739, 20.016) 0.836 483.297 <0.001 T10 10.691 (9.479, 11.902) 0.618 299.059 <0.001 T12 22.707 (21.180, 24.233) 0.779 850.040 <0.001 T12 14.387 (13.186, 15.588) 0.613 551.253 <0.001 Intercept 15.562 (14.450, 16.674) 0.567 752.437 <0.001 Intercept 13.661 (12.540, 14.782) 0.572 570.131 <0.001 Time point Mean amplitude during endurance contraction phase Time point Mean amplitude during post-rest phase b (95%CI) SE Wald P value b (95%CI) SE Wald P value T0 0 T0 0 T4 3.642 (2.608, 4.677) 0.528 47.621 <0.001 T4 0.155 (-0.373, 0.682) 0.269 0.330 >0.05 T6 7.791 (6.649, 8.934) 0.583 178.617 <0.001 T6 -0.353 (-0.759, 0.054) 0.207 2.889 >0.05 T8 12.407 (11.149, 13.664) 0.642 374.085 <0.001 T8 -0.464 (-0.884, -0.043) 0.215 4.665 <0.05 T10 15.410 (14.288, 16.532) 0.573 724.279 <0.001 T10 -0.545 (-0.975, -0.115) 0.220 6.170 <0.05 T12 17.557 (16.427, 18.686) 0.576 928.863 <0.001 T12 -0.562 (-1.016, -0.108) 0.232 5.895 <0.05 Intercept 11.366 (10.503, 12.229) 0.440 666.383 <0.001 Intercept 2.737 (2.312, 3.162) 0.217 159.473 <0.001 PPI: Post-prostatectomy incontinence; T0: Day of catheter removal; T4, T6, T8, T10, T12: 4, 6, 8, 10, and 12 weeks post-intervention, respectively; b: Regression coefficient; 95%CI: 95% confidence interval; SE: Standard error. -
[1] NAKAMURA M, YAMADA Y, SATO Y, et al. Preservation of pelvic floor muscles contributes to early continence recovery after robot-assisted radical prostatectomy[J]. PLoS One, 2022, 17(10): e0275792. DOI: 10.1371/journal.pone.0275792. [2] MILSOM I, ALTMAN D, LAPITAN M C, et al. Epidemiology of urinary (UI) and faecal (FI) incontinence and pelvic organ prolapse (POP) [J]. Ics, 2009: 35-112. [3] AL HUSSEIN AL AWAMLH B, WALLIS C J D, PENSON D F, et al. Functional outcomes after localized prostate cancer treatment[J]. JAMA, 2024, 331(4): 302-317. DOI: 10.1001/jama.2023.26491. [4] 孙懿松, 许方蕾. 前列腺术后尿失禁病人的生活质量调查[J]. 护理研究, 2017, 31(14): 1748-1750. DOI: 10.3969/i.issn.1009-6493.2017.14.023. [5] GACCI M, SAKALIS V I, KARAVITAKIS M, et al. European association of urology guidelines on male urinary incontinence[J]. Eur Urol, 2022, 82(4): 387-398. DOI: 10.1016/j.eururo.2022.05.012. [6] HAGEN S, ELDERS A, STRATTON S, et al. Effectiveness of pelvic floor muscle training with and without electromyographic biofeedback for urinary incontinence in women: multicentre randomised controlled trial[J]. BMJ, 2020, 371: m3719. DOI: 10.1136/bmj.m3719. [7] 陈娟, 任远, 朱兰. 改良牛津肌力分级和盆底表面肌电评估女性压力性尿失禁患者盆底肌功能的相关性[J]. 中华医学杂志, 2020, 100(37): 2908-2912. DOI: 10.3760/cma.j.cn112137-20200301-00525. [8] BAUMANN F T, REIMER N, GOCKELN T, et al. Supervised pelvic floor muscle exercise is more effective than unsupervised pelvic floor muscle exercise at improving urinary incontinence in prostate cancer patients following radical prostatectomy-a systematic review and meta-analysis[J]. Disabil Rehabil, 2022, 44(19): 5374-5385. DOI: 10.1080/09638288.2021.1937717. [9] 中华医学会泌尿外科学分会尿控学组. 男性压力性尿失禁诊断与治疗中国专家共识[J]. 中华泌尿外科杂志, 2022, 43(9): 641-645. DOI: 10.3760/cma.j.cn112330-20220727-00436 [10] 常靖, 常亮. 单因素重复测量设计样本含量的估算及不同计算方法之间的比较[J]. 数理医药学杂志, 2012, 25(5): 505-508. DOI: 10.3969/j.issn.1004-4337.2012.05.001. [11] 许嘉维, 谢双怡, 曹洁, 等. 前列腺癌根治术后尿失禁患者康复管理APP内容框架的构建[J]. 中华现代护理杂志, 2022, 28(6): 776-781. DOI: 10.3760/cma.j.cn115682-20210521-02219. [12] 顾婕, 马倩云, 高旭, 等. 前列腺癌术后尿失禁患者康复护理方案的构建及应用[J]. 中华护理杂志, 2023, 58(9): 1029-1036. DOI: 10.3761/j.issn.0254-1769.2023.09.001. [13] 温颖能, 卢秋莲, 王艳. Glazer盆底表面肌电评估产后盆底肌功能康复应用效果[J]. 中国计划生育学杂志, 2023, 31(5): 1105-1109. DOI: 10.3969/j.issn.1004-8189.2023.05.021. [14] PANÉ-ALEMANY R, RAMÍREZ-GARCÍA I, KAUFFMANN S, et al. Efficacy of transcutaneous perineal electrostimulation versus intracavitary anal electrostimulation in the treatment of urinary incontinence after a radical prostatectomy: randomized controlled trial[J]. Neurourol Urodyn, 2021, 40(7): 1761-1769. DOI: 10.1002/nau.24740. [15] OLEKSY Ł, WOJCIECHOWSKA M, MIKA A, et al. Normative values for Glazer protocol in the evaluation of pelvic floor muscle bioelectrical activity[J]. Medicine (Baltimore), 2020, 99(5): e19060. DOI: 10.1097/MD.0000000000019060. [16] DUMOULIN C, HAY-SMITH J, FRAWLEY H, et al. 2014 consensus statement on improving pelvic floor muscle training adherence: International Continence Society 2011 State-of-the-Science Seminar[J]. Neurourol Urodyn, 2015, 34(7): 600-605. DOI: 10.1002/nau.22796. [17] ZHANG Z, ZHOU X, YANG Z, et al. The clinical symptoms and psychological status of biofeedback electrical stimulation combined with pelvic floor muscle training during the treatment of mild stress urinary incontinence after holmium laser enucleation of the prostate[J]. Urol Int, 2025, 109(1): 34-44. DOI: 10.1159/000539813. [18] OH J J, KIM J K, LEE H, et al. Effect of personalized extracorporeal biofeedback device for pelvic floor muscle training on urinary incontinence after robot-assisted radical prostatectomy: a randomized controlled trial[J]. Neurourol Urodyn, 2020, 39(2): 674-681. DOI: 10.1002/nau.24247. [19] 高成菲, 顾婕, 马倩云, 等. 盆底肌训练联合电生物反馈在前列腺癌根治术后尿失禁患者中的应用研究[J]. 中华护理杂志, 2025, 60(2): 199-206. DOI: 10.3761/j.issn.0254-1769.2025.04.005. [20] GLAZER H I, JANTOS M, HARTMANN E H, et al. Electromyographic comparisons of the pelvic floor in women with dysesthetic vulvodynia and asymptomatic women[J]. J Reprod Med, 1998, 43(11): 959-962.
