 2016, Vol. 43
2016, Vol. 43文章信息
- miR-658和miR-492的差异表达与宫颈鳞状细胞癌盆腔淋巴结转移的关系
- Relationship of Expression Difference of miR-658 and miR-492 with Pelvic Lymph Node Metastasis from Squamous Carcinoma of Cervix
- 肿瘤防治研究, 2016, 43(8): 699-703
- Cancer Research on Prevention and Treatment, 2016, 43(8): 699-703
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2016.08.010
- 收稿日期: 2015-11-06
- 修回日期: 2016-03-31
引用本文 |



2. 510140 广州,广州市妇女儿童医疗中心妇科
2. Department of Gynecology, Guangzhou Women and Children’s Medical Center, Guangzhou 510140, China
宫颈癌(cervical cancer,CC)是最常见的妇科恶性肿瘤之一,全球每年大约有529 800个新诊断病例,死亡人数约为275 000例[1]。在我国,宫颈癌的发病率和死亡率呈逐年上升趋势[2],宫颈癌防治在妇幼保健和肿瘤防治工作中占有重要地位。盆腔淋巴结转移是宫颈癌最重要的预后影响因素之一,无淋巴结转移的早期宫颈癌患者术后5年生存率为75%~90%;如发生淋巴结转移,5年生存率则降至52%~62%[3-4]。淋巴结转移是一个多因素参与、多基因调控的复杂过程,各种生长因子、趋化因子、细胞周期蛋白、信号分子等形成的调节网络促进转移的发生。目前,从遗传学和表观遗传学角度着手,寻找用于肿瘤早期诊断,或者预测肿瘤转移和预后的分子标志物,以及能够作为生物治疗的靶标,已成为肿瘤防治研究的热点[5-6]。
微小RNA(microRNAs,miRNAs)是广泛存在于真核生物中的一类内源性非编码单链小RNA,由19~25个核苷酸组成,由编码或非编码基因转录而来。miRNAs的转录具有组织和时间特异性,通过与目标messenger RNA(mRNA)的碱基互补配对,进而抑制蛋白翻译和(或)降解靶mRNA,在转录后水平调控基因的表达[7]。诸多研究发现,miRNAs在正常组织和肿瘤组织中的表达水平并不相同,与多种肿瘤的发生、侵袭、转移等密切相关[8-10],但miRNAs在宫颈鳞癌盆腔淋巴结转移中扮演的角色尚不清楚。本研究以是否有盆腔淋巴结转移作为分组标准,筛选在宫颈鳞癌转移过程中表达水平有显著差异的miRNAs,为深入研究miRNAs在宫颈鳞癌转移及预后中发挥的作用提供实验依据和理论基础。
1 资料与方法 1.1 研究样本组织标本及相关临床资料由广州市妇女儿童医疗中心肿瘤妇科提供。选择2011年12月——2014年6月间由该科室收治的行宫颈癌根治性子宫全切术+盆腔淋巴结清扫术的24例宫颈鳞癌患者,平均年龄48.2岁(30~68岁)。收集癌组织样本,同时采集患者的临床资料。所有患者符合以下特征:(1)具有白带异常、阴道出血、宫颈糜烂、宫颈肥大、接触性出血等一项或几项临床症状、体征,符合相关手术指征;(2)均经两位以上有经验病理医师独立检查确诊为宫颈鳞状细胞癌;(3)术前均未接受过放疗。该研究已获得深圳市人口和计划生育科学研究所、广州市妇女儿童医疗中心伦理委员会同意,患者及家属均已知晓研究计划并签署知情同意书。24例患者术前HPV-DNA检测均为(+)。标本离体30 min内置于液氮保存。
1.2 实验分组及miRNA芯片操作根据患者术后病理检查结果,将病例分为盆腔淋巴结转移组(n=8)和未转移组(n=16)。使用AllPrep DNA/RNA/miRNAs提取试剂盒(德国Qiagen公司)提取组织总RNA后,采用美国Affymetrix公司的FlashTag Biotin HSR试剂盒对总RNA中的小分子RNA进行加尾和生物素标记,然后将样本用GeneChip Hybridization和Wash and Stain试剂盒与Affymetrix miRNA 4.0芯片进行杂交和洗染,最后将芯片置于GCS3000型芯片扫描仪(美国Affymetrix公司)扫描,具体操作步骤按照说明书进行。
1.3 实时定量RT-PCR法验证miRNA表达差异取等量材料和方法1.2中提取的每个临床组织标本总RNA,用miScriptⅡRT试剂盒(德国Qiagen公司)反转录合成cDNA,然后以cDNA为模版,用miScript SYBR® Green PCR试剂盒(德国Qiagen公司),在7500型实时荧光定量PCR仪(新加坡Applied Biosystems公司)上进行实时定量PCR检测。反应体系20 μl,反应条件:95℃ 15 min,激活DNA聚合酶;40个循环的PCR反应,包括:变性94℃ 15 s,退火55℃ 30 s,延伸70℃ 30s,U6 snRNA作为荧光定量的内参基因。实时定量RT-PCR的相对表达量采用2-ΔΔCt法计算,Ct值即实时荧光定量PCR仪监测到的循环阈值,ΔCt=(CtmiRNA-CtU6),ΔΔCt=ΔCt转移组-ΔCt未转移组,转移组相对于未转移组miRNA表达量倍数=2-ΔΔCt。
1.4 数据分析患者的临床和病理资料采用SPSS18.0软件进行卡方分析,P<0.05为差异有统计学意义;芯片数据采用Affymetrix公司配套软件进行分析:将扫描芯片获得的数据导入Expression Console软件进行芯片质量检测和归一化处理,处理后的数据按照上述实验分组导入Transcriptome Analysis Console软件对miRNAs组间表达差异进行方差分析比较,当同时满足ANOVA P-value<0.05且Fold Change(linear)<-2或>2时,认为存在差异表达。实时定量RT-PCR结果组间比较采用t检验,P<0.05认为差异有统计学意义。
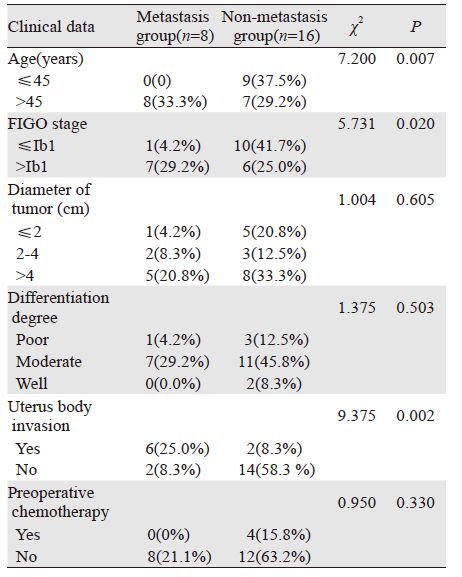
2 结果 2.1 患者临床和病理资料分析在24例宫颈鳞癌样本中,盆腔淋巴结转移组8例,未转移组16例,两组在年龄(P=0.007)、FIGO分期(P=0.020)以及侵及宫体(P=0.002)方面差异有统计学意义,而在分化程度、肿瘤最大直径、术前化疗等方面差异无统计学意义,见表 1。
|
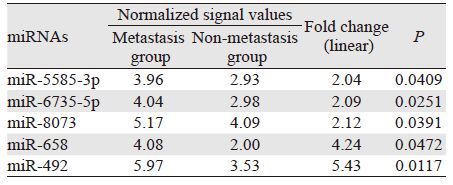
盆腔淋巴结转移组相对于未转移组,有5个miRNAs存在差异表达且全部表现为上调,分别为miR-5585-3p、miR-6735-5p、miR-8073、miR-658和miR-492,具体结果和信号表达热图分别见表 2和图 1。
|

|
| 1: the samples of non-metastasis group (n=16), 2: the samples of metastasis group (n=8); the green color indicated a decreased fold change and the red indicated an increased fold change 图 1 表达有差异的5个miRNAs的miRNA芯片热图 Figure 1 Hot-pot map of five differentially-expressed miRNAs detected by microarrays |
在存在差异表达的5个miRNAs中,miR-658和miR-492表达上调的倍数较大,分别为4.24和5.43,方差分析的P值分别为0.0472和0.0117,提示这两个miRNAs可能与宫颈癌转移密切相关,具体结果见表 2和图 2。

|
| 图 2 芯片检测到的miR-492和miR-658表达水平散点图 Figure 2 Scatter diagram of miR-492 and miR-658 expression levels detected by microarrays |
根据芯片筛查的结果,选择表达量变化最显著的两种miRNA:miR-492和miR-658,利用实时定量RT-PCR检测它们在两组宫颈癌标本中的表达差异。结果显示:这两种miRNA在淋巴结转移组中的表达量较未转移组均有显著增加,与芯片结果一致,见图 3。

|
| 图 3 miR-492和miR-658在淋巴结转移组和未转移组中表达差异的实时定量RT-PCR检测结果 Figure 3 Relative expression of miR-492 and miR-658 in metastasis group vs. non-metastasis group detected by real-time quantification PCR |
众所周知,转移是恶性肿瘤的重要生物学特征,也是导致患者死亡的主要原因之一。在癌症的发生和转移过程中,除了编码基因的突变或表达异常导致的正常细胞增殖、分化和凋亡等生理功能改变之外,还可观察到非编码转录本如miRNAs的表达异常,该异常表达最终表现为促癌还是抑癌作用,取决于其发生调控紊乱的靶点是促癌还是抑癌基因[11-13]。Calin等发现,超过50%的miRNAs编码序列定位在与癌症相关的基因组区域或脆性位点[14]。肿瘤转移涉及多种黏附分子、蛋白水解酶的作用,整个过程受到细胞调节因子、信号转导因子等调控,而这些因子大部分在癌组织中的表达是受到miRNAs调控的。到目前为止,有近70个miRNAs被认为与宫颈癌的发生密切相关,如miR-15a、miR-21、miR-34a、miR-145、miR-218、miR-375和miR-497等[7, 15-16];而宫颈癌转移相关miRNAs的研究报道并不多见。
本研究发现,宫颈鳞癌盆腔淋巴结转移组相对于未转移组,有5个miRNAs存在显著差异表达,且全部表现为上调,其中以miRNA-658和miRNA-492上调的倍数较大。经文献检索发现,miRNA-492由角蛋白19(Keratin 19)基因转录本剪切而来,在转移性肝母细胞瘤、直肠癌、胰腺癌组织中均发现表达上调,与这些肿瘤的发生和转移有关[17-19]。但是miRNA-492在不同组织来源的肿瘤中的致癌机制可能不同,例如Jiang等[20]发现miRNA-492在部分肝癌组织中高表达,且出现这种高表达的患者生存时间较表达水平无明显升高的患者短,进而在体外实验发现miRNA-492通过抑制抑癌基因PTEN来实现致癌作用;而Shen等[21]研究发现在乳腺癌细胞中miRNA-492通过抑制SOX7基因促进癌细胞增殖。关于miRNA-658的文献报道较少,Cummins等[22]在结肠癌细胞系中首次发现miRNA-658,并且将其编码序列定位在22号染色体;Guo等[23]证实miRNA-658在胃癌组织中表达上调。本研究观察到这两种miRNA在宫颈鳞癌盆腔淋巴结转移患者中表达上调,与上述文献报道一致。由此可以证明,miRNA-658和miRNA-492的表达上调与宫颈鳞癌向盆腔淋巴结转移有一定的相关性,但是其在淋巴结转移过程中的具体作用机制,比如其调控了哪些肿瘤转移相关基因、对下游哪些信号通路产生了影响、以及最终导致哪些蛋白因子功能的抑制或者激活等,还有待于进一步的深入研究;这两种miRNA的表达水平与患者术后生存状况的统计学关系,也待随访到一定时间后进行比较分析,今后的研究工作将随着术后随访时间的延长和样本数量的增加,得到更详细的结果。
| [1] | Jemal A, Bray F, Center MM, et al. Global cancer statistics[J]. CA Cancer J Clin, 2011, 61 (2) : 69–90. DOI:10.3322/caac.v61:2 |
| [2] | Hu SY, Zheng RS, Zhao FH, et al. Trend analysis of cervical cancer incidence and mortality rates in chinese women during 1989-2008[J]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao, 2014, 36 (2) : 119–25. [ 胡尚英, 郑荣寿, 赵方辉, 等. 1989至2008年中国女性子宫颈癌发病和死亡趋势分析[J]. 中国医学科学院学报, 2014, 36 (2) : 119–25. ] |
| [3] | Alvarez RD, Soong SJ, Kinney WK, et al. Identification of prognostic factors and risk groups in patients found to have nodal metastasis at the time of radical hysterectomy for early-stage squamous carcinoma of the cervix[J]. Gynecol Oncol, 1989, 35 (2) : 130–5. DOI:10.1016/0090-8258(89)90029-2 |
| [4] | Liu MT, Hsu JL, Liu WS, et al. Prognostic factors affecting the outcome of early cervical cancer treated with radical hysterectomy and post-operative adjuvant therapy[J]. Eur J Cancer Care(Engl), 2008, 17 (2) : 174–81. DOI:10.1111/ecc.2008.17.issue-2 |
| [5] | Dietrich D, Krispin M, Dietrich J, et al. CDO1 promoter methylation is a biomarker for outcome prediction of anthracycline treated, estrogen receptor-positive, lymph node-positive breast cancer patients[J]. BMC Cancer, 2010, 10 : 247. DOI:10.1186/1471-2407-10-247 |
| [6] | Salhia B, Kiefer J, Ross JT, et al. Integrated genomic and epigenomic analysis of breast cancer brain metastasis[J]. PLoS One, 2014, 9 (1) : e85448. DOI:10.1371/journal.pone.0085448 |
| [7] | Granados López AJ, López JA. Multistep model of cervical cancer: participation of miRNAs and coding genes[J]. Int J Mol Sci, 2014, 15 (9) : 15700–33. DOI:10.3390/ijms150915700 |
| [8] | Zhang BG, Li JF, Yu BQ, et al. microRNA-21 promotes tumor proliferation and invasion in gastric cancer by targeting PTEN[J]. Oncol Rep, 2012, 27 (4) : 1019–26. |
| [9] | Lin CW, Chang YL, Chang YC, et al. MicroRNA-135b promotes lung cancer metastasis by regulating multiple targets in the Hippo pathway and LZTS1[J]. Nat Commun, 2013, 4 : 1877. DOI:10.1038/ncomms2876 |
| [10] | Zhao Y, Deng C, Wang J, et al. Let-7 family miRNAs regulate estrogen receptor alpha signaling in estrogen receptor positive breast cancer[J]. Breast Cancer Res Treat, 2011, 127 (1) : 69–80. DOI:10.1007/s10549-010-0972-2 |
| [11] | Garzon R, Calin GA, Croce CM. MicroRNAs in cancer[J]. Annu Rev Med, 2009, 60 : 167–79. DOI:10.1146/annurev.med.59.053006.104707 |
| [12] | Albulescu R, Neagu M, Albulescu L, et al. Tissular and soluble miRNAs for diagnostic and therapy improvement in digestive tract cancers[J]. Expert Rev Mol Diagn, 2011, 11 (1) : 101–20. DOI:10.1586/erm.10.106 |
| [13] | Roa W, Brunet B, Guo L, et al. Identification of a new microRNA expression profile as a potential cancer screening tool[J]. Clin Invest Med, 2010, 33 (2) : E124. |
| [14] | Calin GA, Liu CG, Sevignani C, et al. MicroRNA profiling reveals distinct signatures in B cell chronic lymphocytic leukemias[J]. Proc Natl Acad Sci U S A, 2004, 101 (32) : 11755–60. DOI:10.1073/pnas.0404432101 |
| [15] | Yao T, Lin Z. MiR-21 is involved in cervical squamous cell tumorigenesis and regulates CCL20[J]. Biochim Biophys Acta, 2012, 1822 (2) : 248–60. DOI:10.1016/j.bbadis.2011.09.018 |
| [16] | Zeng KK, Mo XL, Liu F, et al. Differential expression of microRNAs in cervical cancer and cervical precancerous lesions[J]. Zhong Liu Fang Zhi Yan Jiu, 2014, 41 (7) : 789–93. [ 曾康康, 莫祥兰, 刘斐, 等. 宫颈癌及癌前病变组织中microRNAs的差异表达[J]. 肿瘤防治研究, 2014, 41 (7) : 789–93. ] |
| [17] | von Frowein J, Pagel P, Kappler R, et al. MicroRNA-492 is processed from the keratin 19 gene and up-regulated in metastatic hepatoblastoma[J]. Hepatology, 2011, 53 (3) : 833–42. DOI:10.1002/hep.24125 |
| [18] | Gaedcke J, Grade M, Camps J, et al. The rectal cancer microRNAome-microRNA expression in rectal cancer and matched normal mucosa[J]. Clin Cancer Res, 2012, 18 (18) : 4919–30. DOI:10.1158/1078-0432.CCR-12-0016 |
| [19] | Schultz NA, Werner J, Willenbrock H, et al. MicroRNA expression profiles associated with pancreatic adenocarcinoma and ampullary adenocarcinoma[J]. Mod Pathol, 2012, 25 (12) : 1609–22. DOI:10.1038/modpathol.2012.122 |
| [20] | Jiang J, Zhang Y, Yu C, et al. MicroRNA-492 expression promotes the progression of hepatic cancer by targeting PTEN[J]. Cancer Cell Int, 2014, 14 (1) : 95. DOI:10.1186/s12935-014-0095-7 |
| [21] | Shen F, Cai WS, Feng Z, et al. MiR-492 contributes to cell proliferation and cell cycle of human breast cancer cells by suppressing SOX7 expression[J]. Tumour Biol, 2015, 36 (3) : 1913–21. DOI:10.1007/s13277-014-2794-z |
| [22] | Cummins JM, He Y, Leary RJ, et al. The colorectal microRNA-ome[J]. Proc Natl Acad Sci U S A, 2006, 103 (10) : 3687–92. DOI:10.1073/pnas.0511155103 |
| [23] | Guo J, Miao Y, Xiao B, et al. Differential expression of microRNA species in human gastric cancer versus non-tumorous tissues[J]. J Gastroenterol Hepatol, 2009, 24 (4) : 652–7. DOI:10.1111/jgh.2009.24.issue-4 |