 2016, Vol. 43
2016, Vol. 43文章信息
- pT3N0M0期胸段食管鳞癌根治术后的预后因素
- Prognosis Factors for Patients with Stage pT3N0M0 Thoracic Esophageal Squamous Cell Carcinoma after Radical Resection
- 肿瘤防治研究, 2016, 43(6): 483-488
- Cancer Research on Prevention and Treatment, 2016, 43(6): 483-488
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2016.06.010
- 收稿日期: 2015-10-19
- 修回日期: 2016-01-22
引用本文 |

2. 050011 石家庄,河北医科大学第四医院胸外科(*:现单位:221300 邳州,邳州市人民医院放疗科)
2. Department of Thoracic Surgery, The Fourth Hospital of Hebei Medical University, Shijiazhuang 050011, China (*: Present: Department of Radiation Oncology, The People’s Hospital of Pizhou, 221300 Pizhou,China)
我国食管癌高发、且90%以上为鳞癌[1-2]。手术是食管鳞癌最重要的治疗方法之一,术后局部区域复发和(或)远处转移仍是主要失败原因;多数研究显示,Ⅲ期和N1期食管癌术后辅助治疗可能有生存获益,而N0期(尤其T2-3N0M0期)食管癌术后辅助治疗的作用争议很大[2-11]。河北医科大学第四医院胸外科食管癌手术方式以左胸入路的胸腹两野食管癌根治术为主,常规不行锁骨上淋巴结清扫,上纵隔淋巴结清扫多不充分,清扫淋巴结数偏少,术后病理分期中T3N0M0期比例较高[2, 12]; 为此,本研究拟收集术后病理分期为T3N0M0的249例胸段食管鳞癌,分析预后及影响因素,以及术后辅助治疗的价值。
1 资料与方法 1.1 临床资料收集2008年1月—2009年12月在河北医科大学第四医院胸外科行胸腹两野为主的食管癌根治术,术后病理分期为pT3N0M0(UICC,2002年)、术后生存3月以上、未行术前放化疗、随访资料完整的249例胸段食管鳞癌资料。其中男171例、女78例,中位年龄60岁(范围33~78岁);胸上、中和下段鳞癌为39、166和44例;134例有吸烟史,93例有饮酒史,56例有肿瘤家族史;食管肿瘤中位长度5 cm(范围2~12 cm);有50例术前胸部CT可见纵隔小淋巴结(短轴直径<1 cm);术中摘除淋巴结中位数9枚(范围1~27枚),术中无粘连35例、轻度粘连90例、重度粘连124例;左胸入路229例、右胸入路20例;吻合口位置:颈部25例、胸膜顶17例、弓上184例、弓下23例;术后病理中高分化鳞癌210例、低分化鳞癌39例。单纯手术者98例、术后化疗110例、术后放疗20例、术后放化疗21例。
1.2 随访采用电话随访为主,结合书信随访和病例资料查阅,随访截至2013年7月31日。
1.3 统计学方法采用SPSS13.0统计软件,计数资料采用卡方检验,单因素生存分析应用Kaplan-Meier法,组间比较采用双尾Log rank法;多因素分析采用Cox回归模型,backward LR筛选法,P<0.05为差异有统计学意义。
2 结果 2.1 总体生存率所有病例均随访满3年,71例随访满5年,中位随访期48月(5~66月);至随访期结束,249例胸段ESCC中,105例死亡,144例存活;1、2、3、5年总生存率(overall survival,OS)分别为90.0%、77.9%、68.7%和55.2%。随访期内108例复发,其中局部复发61例、远处转移24例、局部区域复发合并远处转移23例;全组1、2、3和5年无进展生存率(progression-free survival,PFS)分别为82.1%、70.8%、61.7%和53.9%。
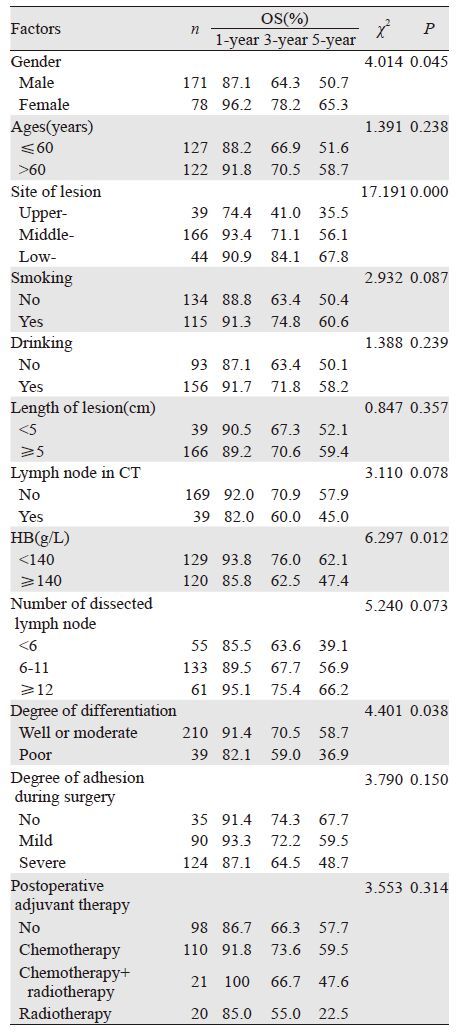
2.2 生存率预后因素单因素分析,性别、肿瘤位置、病理分化程度和术前血红蛋白水平与pT3N0M0期胸段ESCC预后生存有关(P<0.05);而年龄、吸烟史、饮酒史、家族史、肿瘤长度、术后清扫淋巴结数、术前胸部CT纵隔有无小淋巴结(直径<1cm)、术中粘连程度和术后辅助治疗与预后生存均无明显关系(P>0.05),见表 1。多因素分析,肿瘤位置、术前CT纵隔小淋巴结、术前血红蛋白水平和术中清扫淋巴结数为独立预后因素,见表 2。进一步分析,胸上段癌OS明显低于胸中段和胸下段癌(χ2=11.551,13.056; P=0.001,P=0.000),而胸中段与胸下段癌OS相似(χ2=2.696,P=0.101);另外,摘除淋巴结<6枚者OS明显低于≥12枚者(χ2=5.219,P=0.022),而<6枚与6~12枚、6~12枚与≥12枚者比较OS相似(P>0.05)。ESCC单纯手术、术后化疗、术后放疗和术后放化疗OS差异也无统计学意义(P>0.05)。术后无辅助治疗者,术前CT有纵隔小淋巴结者OS明显低于无淋巴结者(χ2=10.006,P=0.002);而术后行辅助治疗者,术前CT显示纵隔有无小淋巴结OS相似(P>0.05)。术前CT无纵隔淋巴结者,术后辅助治疗与否OS相似(P>0.05);而纵隔有小淋巴结者,术后辅助治疗能提高OS(χ2=5.036,P=0.025)。
|

|
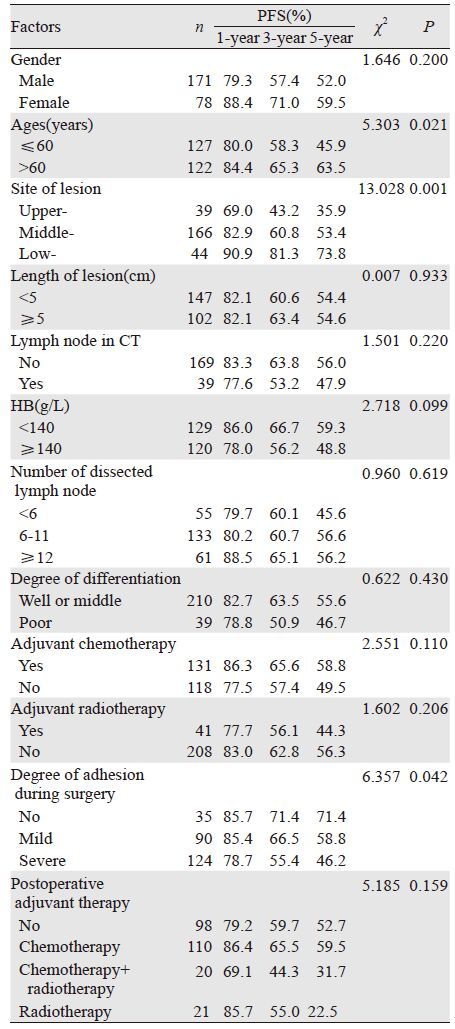
单因素分析,年龄、肿瘤位置和术中粘连程度与PFS有关(P<0.05);而性别、肿瘤长度、术前血红蛋白水平、术前CT纵隔有无小淋巴结、术中摘除淋巴结数、病理分化程度、术后辅助治疗与PFS均无明显关系(P>0.05),见表 3。多因素分析仅肿瘤位置是影响PFS的独立因素,见表 4;年龄和术中粘连程度也是影响PFS的重要因素(χ2=3.765,P=0.052)。另外,术后无辅助治疗者,术前CT提示有纵隔小淋巴结者、无进展生存率明显低于无淋巴结者(χ2=8.966,P=0.003);而术后辅助治疗者,术前CT显示纵隔有无小淋巴结、无进展生存率相似(P>0.05)。术前纵隔无淋巴结者、术后辅助治疗与否,PFS相似(P>0.05) ;而有纵隔小淋巴结者,术后辅助治疗明显增加PFS(χ2=6.933,P=0.008)。
|

|
手术是早中期食管癌最主要的治疗方法。本研究显示,249例pT3N0M0期胸段食管鳞癌(ESCC)胸腹两野根治术后1、3、5年OS为90.0%、68.7%、55.2%。本中心另一组1984—1989年资料显示,512例pT3N0M0食管癌两野术后5年OS为53.9%[2];祝淑衩等[12]报道,2002—2006年我院389例Ⅰ~Ⅱ期胸段食管癌两野为主根治术后5年生存率为44.9%;提示pT3N0M0期食管鳞癌行胸腹两野淋巴结清扫术后近20年生存率相似。Xiao等[4]报道,119例Ⅰ~Ⅱa期(Ⅰ期仅1例)食管癌术后5年生存率为52.3%;张冬坤等[13]报道,349例Ⅱa期食管癌术后5年生存率为51.0%;以上结果与本研究基本一致。但张明月等[14]报道,125例Ⅱa期食管癌术后3、5年生存率为58.5%和43.2%,OS低于本研究。
本研究中,肿瘤位置是影响pT3N0M0期胸段ESCC术后OS和PFS的独立危险因素;胸上、胸中、胸下段ESCC根治术后的5年OS分别为35.7%、56.1%和67.8%(P=0.000),胸上段预后最差、胸中段次之、胸下段癌预后最好。张合林等[2]和安丰山等[15]也报道,食管原发肿瘤位置与OS有关,与本研究结果基本一致。而Chen等[16]、祝淑衩等[12]和张冬坤等[13]报道,肿瘤位置与OS无明显关系。认为其主要原因是,我院食管癌根治术主要采用左胸入路的胸腹两野为主的淋巴结清扫,常规不行主动脉弓以上区域的淋巴结清扫术,胸上段癌手术视野限制、淋巴结清扫不够充分,而胸中下癌清扫主动脉弓以下纵隔和腹腔淋巴结引流区视野良好、淋巴结清扫更彻底。
本研究中,清扫淋巴结数目是影响pT3N0M0胸段ESCC两野根治术后OS的另一个独立因素;清扫淋巴结数越多、预后越好,清扫淋巴结数越少、预后越差。Yang等[17]报道,592例行R0切除术后N0期食管癌,摘除淋巴结<6、6~9、10~17和≥18枚者,5年生存率分别为40.8%、50.6%、55.9%和71.4%(P<0.01);Groth等[18]总结1985—2005年SEER资料,4882例食管癌术后摘除淋巴结数0、1~11、12~29和≥30枚者术后5年生存率分别为27.7%、28.5%、30.9%和47.4%(P<0.01);Greenstein等[19]报道另一组SEER资料,972例Ⅰ~Ⅱa期食管癌术中摘除淋巴结1~10、11~17和≥18枚者,术后5年肿瘤专项生存率分别为55%、66%和75%(P<0.01);解明然等[20]、陈龙奇等[21]和祝淑衩等[12]均报道,食管癌手术清扫淋巴结越多预后越好,反之预后越差;NCCN指南推荐食管癌根治术至少需要清扫15枚淋巴结,因此,食管癌手术时应该尽可能清扫更多的淋巴结。
食管癌术后辅助治疗是否能提高生存率,仍有争议,尤其是食管癌术后Ⅱ期者。前瞻性研究中仅Xiao等[4]报道,术后辅助放疗仅能提高Ⅲ期食管癌的OS;多项回顾性研究显示[5-8, 16, 22],术后放疗可以提高Ⅲ期和淋巴结阳性食管癌者OS,但不能提高Ⅱ期和淋巴结阴性者OS。食管癌术后辅助化疗的作用也有争议;黄伟钊等[9]Meta分析显示,食管癌术后化疗能提高OS;而张杰等[10]另一项Meta分析显示,术后化疗仅能提高Ⅳa期食管癌OS。本研究中,pT3N0M0其胸段ESCC两野根治术后,无论放疗、化疗或放化疗均不能提高OS和PFS,与上述文献报道结果基本一致。本研究中胸段ESCC根治术后近半数出现局部复发或(和)远处转移,且局部区域复发更多、远处转移相对少见;与文献报道结果基本一致[23-27];食管鳞癌术后局部区域复发者中上纵隔和锁骨上区的淋巴结复发最常见[24-27];本研究中50例术前胸部CT提示纵隔有小淋巴结,主要在上纵隔;术前CT有纵隔小淋巴结者生存率明显低于无淋巴结者,是独立预后因素;术前CT有纵隔小淋巴结者、术后给予辅助治疗能明显改善OS和PFS,而纵隔无小淋巴结者、术后辅助治疗无生存获益。因此一方面食管癌手术时尽可能彻底清扫上纵隔淋巴结,若清扫不充分、术前CT提示纵隔有小淋巴结(<1 cm),可能需要术后辅助治疗。
本研究中,术前血红蛋白水平也是影响OS的独立危险因素,血红蛋白(hemoglobin,HB)水平<140 g/L者,OS明显高于HB≥140 g/L者。Zhang等[28]报道,食管鳞癌治疗前HB≥120(女110)g/L和<120(女110)g/L者,同期放化疗后3、5年OS分别为44.1%、23.7%和18.5%、5.6%(P=0.003),是独立预后因素;Hamai等[29]报道,食管癌新辅助放化疗前HB值越高,术后病理缓解率越高。Rades等[30]报道,食管癌放疗前HB≤120、121~140和≥141 g/L者,2年OS分别为9%、35%、12%(P=0.001);治疗前HB水平是影响OS的独立因素,疗前HB121~140 g/L者预后最好;Valencia等[31]也得出相似结果;与本研究结果基本一致。考虑疗前HB121~140 g/L者,肿瘤氧合水平最佳;HB过高则可能由于血流减慢、肿瘤氧合反而变差;HB过低可能由于携氧不足,肿瘤氧合差[30]。
总之,pT3N0M0期胸段食管鳞癌左胸入路的胸腹两野术后疗效较理想,原发肿瘤部位影响OS和PFS,胸上段癌预后最差、胸中段次之、胸下段癌预后最差;淋巴结清扫数目和术前血红蛋白水平也影响OS;术后近半数病例出现病情进展,但术后辅助治疗的价值仍有待证实。
| [1] | Liu W, Hao XS, Jin Y, et al. Analysis of Clinicopathologic Features of Esophageal Cancer Patients after Surgery-a Report of 4,329 Cases[J]. Zhongguo Zhong Liu Lin Chuang, 2008, 35 (5) : 242–4. [刘巍, 郝郗山, 晋颖, 等. 4329例手术后食管癌临床病理资料分析[J]. 中国肿瘤临床,2008, 35 (5) : 242–4. ] |
| [2] | Zhang HL, Liu RL, Shi YT, et al. Analysis of the survival in patients after surgical resection of thoracic esophageal cancer[J]. Zhonghua Zhong Liu Za Zhi, 2009, 31 (7) : 541–5. [张合林, 刘瑞林, 石彦涛, 等. 胸段食管癌切除术患者的预后分析[J]. 中华肿瘤杂志,2009, 31 (7) : 541–5. ] |
| [3] | Malthaner RA, Wong RK, Rumble RB, et al. Neoadjuvant or adjuvant therapy for resectable esophageal cancer: a systematic review and meta analysis[J]. BMC Med, 2004, 2 : 35. |
| [4] | Xiao ZF, Yang ZY, Liang J, et al. Value of radiotherapy after radical surgery for esophageal carcinoma: a report of 495 patients[J]. Ann Thorac Surg, 2003, 75 (2) : 331–6. |
| [5] | Schreiber D, Rineer J, Vongtama D, et al. Impact of postoperative radiation after esophagectomy for esophageal cancer[J]. J Thorac Oncol, 2010, 5 (2) : 244–50. |
| [6] | Shridhar R, Weber J, Hoffe SE, et al. Adjuvant radiation therapy and lymphadenectomy in esophageal cancer: a SEER database analysis[J]. J Gastrointest Surg, 2013, 17 (8) : 1339–45. |
| [7] | Zhu WG, Tao GZ, Li T, et al. Effects of postoperative 3-dimensional conformal radiotherapy on lymph node positive patients after radical resection of esophageal carcinoma[J]. Zhonghua Fang She Yi Xue Yu Fang Hu Za Zhi, 2011, 31 (5) : 571–4. [朱卫国, 陶光州, 李涛, 等. 淋巴结阳性的食管癌患者术后预防性放射治疗的回顾性研究[J]. 中华放射医学与防护杂志,2011, 31 (5) : 571–4. ] |
| [8] | Liu X, Zhang WC, Yu SF, et al. Patterns of failure after radical surgery among patients vdth stage T2-3 N0 M0 esophageal squamous cell carcinoma-potential value of postoperative radiotherapy[J]. Zhonghua Fang She Zhong Liu Xue Za Zhi, 2015, 24 (1) : 19–24. [刘晓, 章文成, 于舒飞, 等. T2-3 N0 M0期食管癌凡术后失败模式分析术后放疗潜在价值与意义[J]. 中华放射肿瘤学杂志,2015, 24 (1) : 19–24. ] |
| [9] | Huang WZ, Fu JH, Hu Y, et al. Meta-analysis of Postoperative Adjuvant Chemotherapy for Localized Esophageal Carcinoma[J]. Ai Zheng, 2006, 25 (10) : 1303–6. [黄伟钊, 傅剑华, 胡祎, 等. 食管癌术后辅助化疗价值的Meta分析[J]. 癌症,2006, 25 (10) : 1303–6. ] |
| [10] | Zhang J, Chen HQ, Zhang YW, et al. Adjuvant chemotherapy in esophageal cancer: a meta-analysis and experience from Cancer Hospital, Fudan University[J]. Zhongguo Ai Zheng Za Zhi, 2008, 18 (4) : 276–81. [张杰, 陈海泉, 张亚伟, 等. 食管癌术后辅助化疗的荟萃分析和来自复旦大学附属肿瘤医院的配对研究[J]. 中国癌症杂志,2008, 18 (4) : 276–81. ] |
| [11] | Lv X, Huang J. Current status of postoperative adjuvant therapy in esophageal squamous cell carcinoma[J]. Ai Zheng Jin Zhan, 2013, 11 (4) : 314–8. [吕潇, 黄镜. 食管鳞癌术后辅助治疗现状[J]. 癌症进展,2013, 11 (4) : 314–8. ] |
| [12] | Zhu SC, Song CL, Shen WB, et al. Prognostic analysis of clinicopathological factors in patients after radical resection of esophageal carcinoma[J]. Zhonghua Zhong Liu Za Zhi, 2012, 34 (4) : 281–6. [祝淑钗, 宋长亮, 沈文斌, 等. 食管癌根治性切除术后患者预后的影响因素分析[J]. 中华肿瘤杂志,2012, 34 (4) : 281–6. ] |
| [13] | Zhang DK, Su XD, Lin P, et al. Survival Analysis of Patients with Stage Ⅱ Squamous Cell Carcinoma of the Thoracic Esophagus after esophagectomy[J]. Ai Zheng, 2008, 27 (2) : 113–8. [张冬坤, 苏晓东, 林鹏, 等. 467例Ⅱ期胸段食管鳞癌切除术后患者的生存分析[J]. 癌症,2008, 27 (2) : 113–8. ] |
| [14] | Zhang MY, Wang Z, Liu XY, et al. The local control of radiotherappy following Ivor-Lewis esophagectomy in the patients with stage ⅡA middli-third thoracic esophageal cancer[J]. Zhonghua Wai Ke Za Zhi, 2008, 46 (14) : 1048–50. [张明月, 王洲, 刘相燕, 等. Ivor-Lewis手术辅助放疗对ⅡA期中段食管癌局部控制的临床研究[J]. 中华外科杂志,2008, 46 (14) : 1048–50. ] |
| [15] | An FS, Huang JQ, Chen SH. AnaIysis of lymph node metastases of 217 cases of thoracic esophageaI carcinoma and its impact on prognosis[J]. Ai Zheng, 2003, 22 (9) : 974–7. [安丰山, 黄金球, 陈少湖. 217例胸段食管癌淋巴结转移及其对预后影响的分析[J]. 癌症,2003, 22 (9) : 974–7. ] |
| [16] | Chen J, Zhu J, Pan J, et al. Postoperative radiotherapy improved survival of poor prognostic squamous cell carcinoma esophagus[J]. Ann Thorac Surg, 2010, 90 (2) : 435–42. |
| [17] | Yang HX, Xu Y, Fu JH, et al. An evaluation of the number of lymph nodes examined and survival for node-negative esophageal carcinoma:data from China[J]. Ann Surg Oncol, 2010, 17 (7) : 1901–11. |
| [18] | Groth SS, Virnig BA, Whitson BA, et al. Determination of the minimum number of lymph nodes to examine to maximize survival in patients with esophageal carcinoma: data from the Surveillance Epidemiology and End Results database[J]. J Thorac Cardiovasc Surg, 2010, 139 (3) : 612–20. |
| [19] | Greenstein AJ, Litle VR, Swanson SJ, et al. Effect of the number of lymph nodes sampled on postoperative survival of lymph nodenegative esophageal cancer[J]. Cancer, 2008, 112 (6) : 1239–46. |
| [20] | Xie MR, Mei XY, Li T, et al. The prognostic value of the number of negative lymph nodes in esophageal carcinoma without lymphatic metastasis after esophagectomy[J]. Zhonghua Xiong Xin Xue Guan Wai Ke Za Zhi, 2014, 30 (4) : 221–4. [解明然, 梅新宇, 李田, 等. 阴性淋巴结数目对无淋巴结转移食管鳞癌患者预后的影响[J]. 中华胸心血管外科杂志,2014, 30 (4) : 221–4. ] |
| [21] | Chen LQ, Hu CY, Zhang HL, et al. Influence of removed lymph nodes on the TNM stage and survival in advanced esophageal carcinoma[J]. Zhonghua Zhong Liu Za Zhi, 2007, 29 (8) : 604–8. [陈龙奇, 胡春燕, 张合林, 等. 淋巴结清扫数目对进展期食管癌 TNM分期和预后的影响[J]. 中华肿瘤杂志,2007, 29 (8) : 604–8. ] |
| [22] | Xu Y, Liu J, Du X, et al. Prognostic impact of postoperative radiation in patients undergoing radical esophagectomy for pathologic lymph node positive esophageal cancer[J]. Radiat Oncol, 2013, 8 : 116. |
| [23] | Su XD, Zhang DK, Zhang X, et al. Prognostic factors in patients with recurrence after complete resection of esophageal squamous cell carcinoma[J]. J Thorac Dis, 2014, 6 (7) : 949–57. |
| [24] | Liu Q, Cai XW, Wu B, et al. Patterns of failure after radical surgery among patients with thoracic esophageal squamous cell carcinoma: implications for the clinical target volume design of postoperative radiotherapy[J]. PLoS One, 2014, 9 (5) : e97225. |
| [25] | Guo XF, Mao T, Gu ZT, et al. Clinical study on postoperativ e recurrence in patients with pN0 esophageal squamous cell carcinoma[J]. J Cardiothorac Surg, 2014, 9 : 150. |
| [26] | Mariette C, Balon JM, Piessen G, et al. Pattern of recurrence following complete resection of esophageal carcinoma and factors predictive of recurrent disease[J]. Cancer, 2003, 97 (7) : 1616–23. |
| [27] | Liu J, Lv CX, Wang JM, et al. Pattern of relapse in left thoracotomy surgical treated patients with thoracic esophageal cancer and their value in target region delineation in postoperative radiotherapy[J]. Zhonghua Fang She Zhong Liu Za Zhi, 2013, 22 (2) : 111–4. [刘俊, 吕长兴, 王家明, 等. 104例胸段食管癌左胸路径术后局部复发规律及放疗靶区范围探讨[J]. 中华放射肿瘤杂志,2013, 22 (2) : 111–4. ] |
| [28] | Zhang HQ, Wang RB, Yan HJ, et al. Prognostic significance of CYFRA21-1, CEA and hemoglobin in patients with esophageal squamous cancer undergoing concurrent chemoradiotherapy[J]. Asian Pac J Cancer Prev, 2012, 13 (1) : 199–203. |
| [29] | Hamai Y, Hihara J, Taomoto J, et al. Hemoglobin level influences tumor response and survival after neoadjuvant chemoradiotherapy foresophageal squamous cell carcinoma[J]. World J Surg, 2014, 38 (8) : 2046–51. |
| [30] | Rades D, Schild SE, Bahrehmand R, et al. Prognostic factors in the nonsurgical treatment of esophageal carcinoma with radiotherapy or radiochemotherapy: the importance of pretreatment hemoglobin levels[J]. Cancer, 2005, 103 (8) : 1740–6. |
| [31] | Valencia Julve J, Alonso Ordu?a V, Escó Barón R, et al. Influence of hemoglobin levels on survival after radical treatment of esophageal carcinoma with radiotherapy[J]. Clin Transl Oncol, 2006, 8 (1) : 22–30. |