 2025, Vol. 36
2025, Vol. 36扩展功能
文章信息
- 李培珍, 马玥, 李佳成, 傅琼瑶, 孙美姣
- LI Pei-zhen, MA Yue, LI Jia-cheng, FU Qiong-yao, SUN Mei-jiao
- 浙江省金华市2019-2023年发热伴血小板减少综合征流行病学特征分析
- Epidemiological characteristics of severe fever with thrombocytopenia syndrome in Jinhua, Zhejiang Province, China, 2019-2023
- 中国媒介生物学及控制杂志, 2025, 36(2): 190-194
- Chin J Vector Biol & Control, 2025, 36(2): 190-194
- 10.11853/j.issn.1003.8280.2025.02.009
-
文章历史
- 收稿日期: 2024-09-20



发热伴血小板减少综合征(severe fever with thrombocytopenia syndrome,SFTS)是一种由大别班达病毒(Dabie bandavirus,DBV)感染引起的,以发热伴血小板减少为主要临床特征的蜱媒传染病,病情严重的患者可表现为多脏器功能衰竭甚至死亡[1]。2011-2021年全国共报告SFTS病例18 902例,发病率整体呈上升趋势,病例主要集中于河南、山东、湖北、安徽、江苏、浙江和辽宁7个省份,不同省份病死率差异较大,浙江和山东省的病死率较高[2]。浙江省2011年首次发现SFTS病例,2011-2019年共报告459例确诊病例,发病率整体呈逐年上升趋势[3-5]。近年来,金华市SFTS发病率也有上升趋势,且病死率较浙江省平均水平高[2]。为了解金华市SFTS病例的流行特征,更好地对SFTS开展防控工作,本研究针对2019-2023年金华市SFTS报告病例进行流行病学特征分析。
1 材料与方法 1.1 资料从中国疾病预防控制信息系统传染病报告信息管理系统、个案调查原始记录表以及浙江省慢性病监测信息管理系统的死亡登记管理模块中收集2019-2023年金华市84例SFTS确诊病例信息,包括性别、年龄、人群分类、发病时间、就诊时间、确诊时间、地区、是否死亡等。
1.2 方法采用描述流行病学研究方法对SFTS病例进行分析。包括各年病例分布、病例人群分布、病例地区分布、发病时间分布、病死率分析等。
1.3 统计学分析采用Excel 2016软件整理数据并建立数据库,ArcGIS 10.8软件绘制SFTS病例统计地图,SPSS 27.0软件进行统计分析。年龄、时间间隔等定量资料用均数±标准差(x±s)和中位数[M(P25,P75)]描述,组间比较用独立样本t检验;发病率、病死率等定性资料用相对数描述,组间比较用χ2检验,多重比较用Bonferroni方法,P < 0.05为差异有统计学意义。
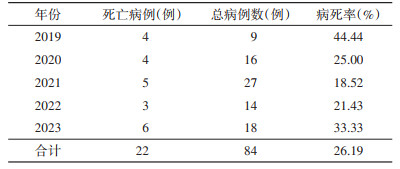
2 结果 2.1 病例概况2019-2023年金华市共报告SFTS病例84例,发病率在0.16/10万~0.38/10万,平均发病率为0.26/10万,见图 1。报告SFTS死亡病例22例,总病死率为26.19%,见表 1。

|
| 图 1 2019-2023年浙江省金华市84例发热伴血小板减少综合征发病情况 Figure 1 Annual distribution of 84 cases of severe fever with thrombocytopenia syndrome in Jinhua, Zhejiang Province, 2019-2023 |
| |
|
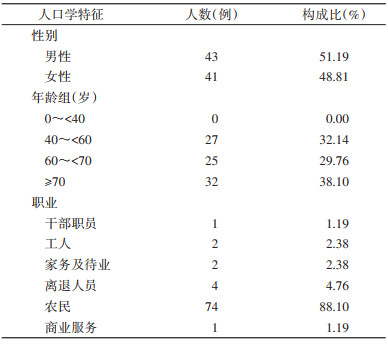
84例SFTS病例的男女性别比为1.05∶1(43∶41),男性(1.48/10万)与女性(1.51/10万)累积报告发病率差异无统计学意义(χ2=0.008,P=0.928)。报告病例以中老年为主,发病年龄最小44岁,最大90岁,平均年龄为(65.46±10.07)岁。病例人群分类以农民为主,共74例,占88.10%。见表 2。
|
2019-2023年除武义县外,全市其他8个县(市、区)均有SFTS病例报告,报告病例数居前3位的县(市、区)的依次为东阳(30例,35.71%),义乌(18例,21.43%)和兰溪市(17例,20.24%)。见图 2。

|
| 图 2 2019-2023年浙江省金华市发热伴血小板减少综合征报告病例地区分布 Figure 2 Regional distribution of reported cases of severe fever with thrombocytopenia syndrome in Jinhua, Zhejiang Province, 2019-2023 |
| |
2019-2023年,除1、2和11月外,其他各月均有SFTS病例报告,发病集中于夏、秋季,主要分布在4-10月,占总报告例数的95.24%(80/84);发病高峰期为5-7月,报告病例数占总报告例数的64.29%(54/84),10月出现发病小高峰。2019年12月有1例SFTS病例报告。见图 3。

|
| 图 3 2019-2023年浙江省金华市84例发热伴血小板减少综合征病例月分布 Figure 3 Monthly distribution of 84 cases of severe fever with thrombocytopenia syndrome in Jinhua, Zhejiang Province, 2019-2023 |
| |
报告死亡病例中男性与女性均为11例,病死率分别为25.58%(11/43)和26.83%(11/41),病死率性别差异无统计学意义(χ2=0.017,P=0.897)。22例死亡病例平均年龄为(70.45±9.96)岁,62例存活病例平均年龄为(63.69±9.57)岁,死亡组平均年龄大于存活组(t=2.817,P=0.006)。
按照报告病例的年龄进行分组。其中,40~ < 60岁病例死亡4例,病死率为14.81%(4/27),60~ < 70岁病例死亡4例,病死率为16.00%(4/25),≥70岁病例死亡14例,病死率为43.75%(14/32),不同年龄组病死率差异有统计学意义(χ2=8.255,P=0.016),≥70岁病例病死率显著高于40~ < 60岁病例。排除发病日期、就诊日期和确诊日期无记录的病例,剩余80例病例中,发病至首次就诊的时间间隔最短为0 d,M(P25,P75)为2.00(1.00,4.00)d;发病至确诊的时间间隔最短为2 d,M(P25,P75)为6.50(5.00,9.00)d;首次就诊至确诊的时间间隔最短为0 d,M(P25,P75)为4.00(2.00,6.00)d。
3 讨论金华市位于金衢盆地东段,属于浙中丘陵盆地地区,地势南北高、中部低,具有山地、大小盆地以及丘陵等多种地形地貌,属中亚热带季风气候,多样的地理环境以及适合的气温气候有利于蜱的生长和蜱媒传染病的传播[6]。本研究针对2019-2023年金华市SFTS报告病例数据的分析发现,全市SFTS发病率自2019年开始逐年上升,2021年为发病高峰,这与陈秋兰等[2]对浙江省的研究结果一致,发病率的上升可能与医务人员对SFTS疾病敏感程度的提高有关。2022年开始发病率出现回落的现象,可能与近些年金华市加强对SFTS监测和积极采取干预措施有关,虽然2023年又出现增长,但增长幅度不大,这可能与新型冠状病毒感染疫情实施“乙类乙管”后,人群野外暴露(劳作)显著增加有关。SFTS男女性发病率无明显差别,病例主要为中老年农民。全市SFTS病例无明显的空间聚集性,除武义县外,各个县(市、区)均有病例报告,东阳市病例数最多。SFTS发病具有较明显的季节性,高发季节主要为春夏季,与既往研究一致[2, 7],主要与蜱虫活动和人群暴露增加有关。
2019-2023年金华市总病死率较高,以2019年最高,此后出现下降趋势,2021年病死率降至最低水平,此后又逐渐上升。男女性别病死率无明显差别。与既往研究结果一致[8-9],年龄增长会在一定程度上影响病死率的大小,年龄大的病例更容易死亡。金华市SFTS病例发病至首次就诊、发病至确诊以及首次就诊至确诊的时间间隔均较长,说明医疗机构对SFTS诊断敏感性还不够高,往往容易延误病例救治时间,进一步增加病例死亡风险,与既往研究类似[10-11]。
2019-2023年金华市SFTS发病率(26.19%)比全国重点省份发病率低,但病死率较高,远高于2011-2021年全国的5.11%,甚至高于浙江省的11.27%[2]。本研究发现,金华市SFTS病死率高的原因可能与病例的年龄多为≥60岁的老年人以及确诊时间过长有关。与浙江省其他病死率较低的地级市相比,金华市SFTS病例的平均年龄及高龄年龄组占比均高于丽水市[12],金华市确诊病例平均确诊时间长于台州市[13]。此外,金华市SFTS病死率远高于全国平均水平的原因可能是数据来源有所不同,本研究不仅从中国疾病预防控制信息系统传染病报告信息管理系统获取SFTS报告数据,且进一步追踪了所有SFTS病例出院后的后续治疗,同时通过浙江省慢性病监测信息管理系统的死亡登记管理模块将确诊后21 d内无其他原因死亡的病例修正为SFTS死亡病例,更能评估SFTS死亡风险的实际情况。金华市与同样修正死亡病例数据的大连市SFTS病死率水平相当[14],这提示对SFTS病例后续的跟踪需要引起关注。
综上所述,金华市SFTS病例主要为中老年农民,春夏季蜱活动时期发病率高,且近年有病例增多的趋势,提示应进一步加强对SFTS的重视程度。建议在流行季节前对居民开展健康教育,提高人群对SFTS的认识以及防蜱意识;加强对环境和宿主动物的管理,尽可能减少蜱在居住环境的孳生地;加强蜱的生态学密度监测以及病原学监测,及时反馈并进行风险评估。因SFTS初期症状的特异性较低,在病例高发的地区有大约8%的病例未被诊断[15],这需要医务人员和患者提高诊疗知识和防治意识,早发现、早诊断、早治疗,减少重症和死亡病例的发生。
利益冲突无
志谢 感谢金华市各县(市、区)疾控同仁对病例流调的支持利益冲突 无
| [1] |
迪丽胡玛尔·扎衣尔, 张斌, 朱彬, 等. 发热伴血小板减少综合征发病机制及诊疗研究进展[J]. 中国病毒病杂志, 2024, 14(2): 189-195. Dilihumaer ZYE, Zhang B, Zhu B, et al. Research progress of pathogenesis, diagnosis and treatment of severe fever with thrombocytopenia syndrome[J]. Chin J Viral Dis, 2024, 14(2): 189-195. DOI:10.16505/j.2095-0136.2024.2013 |
| [2] |
陈秋兰, 朱曼桐, 陈宁, 等. 2011-2021年全国发热伴血小板减少综合征流行特征分析[J]. 中华流行病学杂志, 2022, 43(6): 852-859. Chen QL, Zhu MT, Chen N, et al. Epidemiological characteristics of severe fever with thrombocytopenia syndrome in China, 2011-2021[J]. Chin J Epidemiol, 2022, 43(6): 852-859. DOI:10.3760/cma.j.cn112338-20220325-00228 |
| [3] |
Sun JM, Chai CL, Lv HK, et al. Epidemiological characteristics of severe fever with thrombocytopenia syndrome in Zhejiang Province, China[J]. Int J Infect Dis, 2014, 25: 180-185. DOI:10.1016/j.ijid.2014.02.022 |
| [4] |
吴昊澄, 徐校平, 吴晨, 等. 浙江省2011-2015年发热伴血小板减少综合征发病空间预测[J]. 中华流行病学杂志, 2016, 37(11): 1485-1490. Wu HC, Xu XP, Wu C, et al. Spatial analysis and prediction of severe fever with thrombocytopenia syndrome in Zhejiang Province, 2011-2015[J]. Chin J Epidemiol, 2016, 37(11): 1485-1490. DOI:10.3760/cma.j.issn.0254-6450.2016.11.011 |
| [5] |
施旭光, 孙继民, 刘营, 等. 2015-2019年浙江省发热伴血小板减少综合征流行特征分析[J]. 疾病监测, 2021, 36(5): 431-435. Shi XG, Sun JM, Liu Y, et al. Epidemiological characteristics of fever with thrombocytopenia syndrome in Zhejiang, 2015-2019[J]. Dis Surveill, 2021, 36(5): 431-435. DOI:10.3784/jbjc.202101070014 |
| [6] |
朱波, 郎少伟, 边勇, 等. 我国新发蜱媒传染病流行风险及应对措施[J]. 中国国境卫生检疫杂志, 2024, 47(4): 431-435. Zhu B, Lang SW, Bian Y, et al. Epidemic risk and response measures of novel tick-borne infectious diseases in China[J]. Chin J Front Health Quar, 2024, 47(4): 431-435. DOI:10.16408/j.1004-9770.2024.04.023 |
| [7] |
张乾通, 孙继民, 凌锋, 等. 浙江省2021年发热伴血小板减少综合征报告病例及蜱媒监测结果分析[J]. 中国媒介生物学及控制杂志, 2022, 33(4): 485-488. Zhang QT, Sun JM, Ling F, et al. Analysis of reported cases of fever with thrombocytopenia syndrome and tick vectors surveillance results in Zhejiang Province of China in 2021[J]. Chin J Vector Biol Control, 2022, 33(4): 485-488. DOI:10.11853/j.issn.1003.8280.2022.04.008 |
| [8] |
Dong Y, Lin SH, Jiang L, et al. Clinical characteristics and risk factors of 267 patients having severe fever with thrombocytopenia syndrome-new epidemiological characteristics of fever with thrombocytopenia syndrome: Epidemiological characteristics of SFTS[J]. Medicine (Baltimore), 2022, 101(50): e31947. DOI:10.1097/MD.0000000000031947 |
| [9] |
Wang WJ, Zhang AP, Wu QL, et al. Epidemiological and clinical characteristics of severe fever with thrombocytopenia syndrome in southern Anhui Province, China, 2011-2020[J]. Jpn J Infect Dis, 2022, 75(2): 133-139. DOI:10.7883/yoken.JJID.2021.391 |
| [10] |
Sun JM, Gong ZY, Ling F, et al. Factors associated with severe fever with thrombocytopenia syndrome infection and fatal outcome[J]. Sci Rep, 2016, 6: 33175. DOI:10.1038/srep33175 |
| [11] |
Kim J, Hong HJ, Hwang JH, et al. Risk factors associated with death due to severe fever with thrombocytopenia syndrome in hospitalized Korean patients (2018-2022)[J]. Osong Public Health Res Perspect, 2023, 14(3): 151-163. DOI:10.24171/j.phrp.2023.0048 |
| [12] |
陈君丽, 李婷婷, 吴金香. 丽水地区发热伴血小板减少综合征临床特征分析[J]. 中国地方病防治杂志, 2023, 38(4): 338-339. Chen JL, Li TT, Wu JX. Analysis of clinical characteristics of fever with thrombocytopenia syndrome in Lishui[J]. Chin J Ctrl Endem Dis, 2023, 38(4): 338-339. |
| [13] |
李江麟, 胡雅飞, 翁坚, 等. 台州市发热伴血小板减少综合征流行特征分析[J]. 预防医学, 2019, 31(12): 1267-1268, 1272. Li JL, Hu YF, Weng J, et al. Epidemiological characteristics of severe fever with thrombocytopenia syndrome in Taizhou[J]. Prev Med, 2019, 31(12): 1267-1268, 1272. DOI:10.19485/j.cnki.issn2096-5087.2019.12.019 |
| [14] |
齐上, 庞为, 邢俊, 等. 2011-2023年大连市发热伴血小板减少综合征流行病学特征及空间分析[J]. 中国公共卫生, 2024, 40(9): 1052-1058. Qi S, Pang W, Xing J, et al. Epidemiological characteristics and spatial aggregation of severe fever with thrombocytopenia syndrome(SFTS) in Dalian City from 2011 to 2023[J]. Chin J Public Health, 2024, 40(9): 1052-1058. DOI:10.11847/zgggws1142880 |
| [15] |
Du YH, Cheng NN, Li Y, et al. Seroprevalance of antibodies specific for Severe fever with thrombocytopenia syndrome virus and the discovery of asymptomatic infections in Henan Province, China[J]. PLoS Negl Trop Dis, 2019, 13(11): e0007242. DOI:10.1371/journal.pntd.0007242 |