 2012, Vol. 28
2012, Vol. 28

2. 青岛大学医学院公共卫生学系
人口老龄化是21世纪全球人口发展面临的共同问题,随着年龄增长,老年人躯体功能[1, 2, 3]、认知功能[4]呈下降趋势,抑郁症状[5]逐渐加剧,严重影响其晚年生活质量,给老年人及其家庭和社会带来沉重的疾病负担和经济负担。因此,探索人类老化规律,对延长其预期寿命及提高其生活质量有着重要意义。为了解山东省青岛市老年人老化表型分布特征,分析年龄对老化表型的影响,探讨除年龄以外,影响老化的潜在机制,为提高其生活质量提供科学依据,于2009年8月-2010年11月对青岛市2006名中老年人老化表型进行现况研究。现将结果报告如下。
1 对象与方法 1.1 对象根据地理位置、经济状况等因素,在青岛市四方区、黄岛区、胶南市、即墨市分别分层随机抽取10、12、19和25个社区(或村),再按身份证号对50~74岁常住居民(在当地居住时间≥5年)进行随机抽样,共抽取2476人。排除患有严重疾病、意识不清不能正常交流者,有严重肢体残疾、不能配合者和本人不愿参加、未签署知情同意书者。
1.2 方法采取问卷调查、体能测试和体格检查相结合的调查方法。由调查员采用自制调查问卷对调查对象进行面访式调查。问卷内容包括年龄、性别、基本信息、健康自评(self-rated health,SRH)、认知功能和抑郁症状等。健康自评结果由非常差到非常好分别赋值1~5分,分数越高表示自评健康状况越好。认知功能部分、抑郁症状部分的量表及赋值参照文献[6, 7]。由社区医生在现场对调查对象进行体能测试和体格检查,项目包括握力、5次起坐时间(time to complete sit-to-stand test,STS-5)、第1s肺通气量(forced expiratory volume in 1 second,FEV1)、最大肺通气量(force vital capacity,FVC)、近视力、牙齿脱落数、平均听阈等老化表型的数量性状特征。其具体的测量仪器、测量方法及赋值均参照文献[6, 7]。
1.3 统计分析应用Epi Data 3.0软件建立数据库,应用SPSS 18.0软件对这10个表型进行正态分布描述,再根据变量分布类型,采用x ± s或M(P25、P75)来描述数据的集中趋势和离散趋势;应用Amos 7.0软件,采用极大似然法构建结构方程模型,用绝对拟合指数和相对拟合指数评价模型,进行模型修正,检验水准α=0.05。
2 结果 2.1 一般情况发放问卷2476份,回收2006份,问卷回收率为81.02%,其中有效问卷2006份,问卷有效率为100%。其中男性844人,女性1162人,男女性别比1:1.377,年龄为50~74岁,平均年龄为(60.5±7.1)岁,其中男性平均年龄为(61.2±7.3)岁,女性平均年龄为(60.0±6.8)岁。
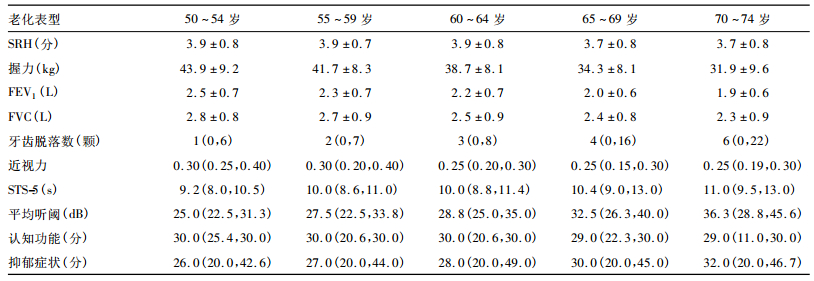
2.2 老化表型的统计描述(表 1、2)| 表 1 不同年龄组男性老化表型的集中趋势和离散趋势 |
| 表 2 不同年龄组女性老化表型的集中趋势和离散趋势 |
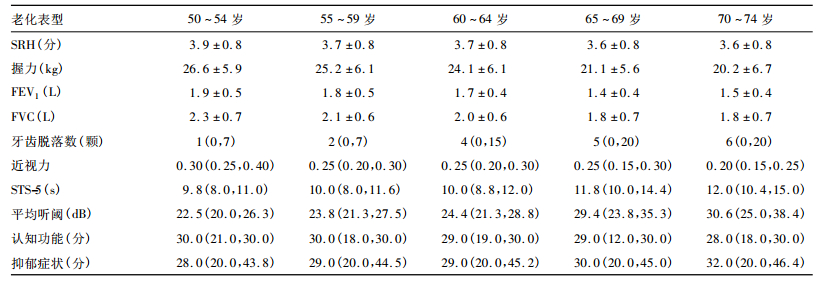
对10个老化表型做频数分布图,发现SRH、握力、FEV1、FVC呈近似正态分布,用x ± s来描述;STS-5、近视力、平均听阈、牙齿脱落数、认知功能、抑郁症状呈偏态分布,用M(P25、P75)来描述。SRH、握力、FEV1、FVC分别为(3.8±0.8)分、(30.4±10.7)kg、(1.9±0.6)L、(2.3±0.8)L;STS-5、近视力、牙齿脱落数、平均听阈、认知功能、抑郁症状的M(P25、P75)分别为10.0(8.7,12.0)s、0.25(0.20,0.30)、3(1,5)颗、26.3(22.5,32.5)dB、30(27,30)分、29(23,34)分。随着年龄增大,男性和女性的SRH、握力、FEV1、FVC、近视力、认知功能平均水平均下降,离散度均变大;STS-5、牙齿脱落数、平均听阈、抑郁症状平均水平均上升,离散度均变大。在同一年龄组,男性SRH、握力、STS-5、肺功能、认知功能、抑郁症状均优于女性,女性听力状况优于男性,而男性与女性的近视力和牙齿脱落数无明显差异。
2.3 结构方程模型(图 1) | 注: 各通径上数值为变量间的路径系数。 图 1 老年人老化表型结构方程模型图 |
模型的绝对拟合指数χ2=381.395,P<0.001,RMSEA=0.07,NFI=0.902,CFI=0.909,TLI=0.829,模型拟合较为理想。年龄对10个老化表型的影响均有统计学意义(P<0.001);随着居民年龄增大,其SRH、握力、FEV1、FVC、近视力、认知功能均呈下降趋势,STS-5、牙齿脱落数、平均听阈、抑郁症状均呈上升趋势(∣β∣=0.005~0.516,P<0.001)。潜在共因子路径系数的P值表明,有1个独立于年龄外的潜在共因子影响了除平均听阈(P=0.161)以外的其他9个表型(∣β∣=0.012~5.513,P<0.05),其使SRH、握力、FEV1、FVC、近视力水平、认知功能均提高,使STS-5、牙齿脱落数和抑郁症状均减少,该潜在共因子是一个老化的保护因素。
3 讨论健康自评是评价老年人主观健康的重要指标,也是独立的死亡预测指标,随着年龄增大,老年人的健康自评得分趋于下降[8, 9, 10],与本研究结果一致。握力是评估上肢力量的主要指标之一,也是能够确切预测多种关键结局的重要指标,肌肉力量随着年龄增大会逐渐减弱[11],与本研究结果一致。STS-5是对下肢肌肉力量、踝关节、髋关节、膝关节伸强度以及身体平衡、姿势保持能力的综合考评[12, 13]。本研究结果表明,随着年龄增大,居民的STS-5延长,提示其躯体综合能力随着年龄增大而衰退,与另一类似的中国老年人群(65~80岁)研究结果一致[13]。本研究结果还表明,老年人的FEV1、FVC和听力水平均随着年龄增大而下降,而各频率听阈上升;随年龄增大,老年人近视力呈下降趋势,提示其晶状体弹性改变带来的视力变化在中年期就已经凸显;老年人的认知功能随着年龄增大而下降,与国内其他研究一致[14]。年龄与老年抑郁症之间的关系一直存有争议,尽管本研究和其他一些研究发现随年龄增大,抑郁症患病率和发病率均增加[15],但有研究发现这种趋势无统计学意义[16, 17],还有研究发现在调整了其他变量之后,年龄的影响无统计学意义[18, 19]。
| [1] | Frederiksen H,Hjelmborg J,Mortensen J,et al.Age trajectories of grip strength:cross-sectional and longitudinal data among 8 342 Danes aged 46 to 102[J].Ann Epidemiol.2006,16:554-562. |
| [2] | Ummuhan BA,Ugur C,Nesrin Y,et al.Balance performance,aging and falling:a comparative study based on a Turkish sample[J].Arch Gerontol Geriatr,2008,46:283-292. |
| [3] | Rode A,Shephard RJ.The ageing of lung function:cross-sectional and longitudinal studies of an Inuit community[J].Eur Respir J, 1994,7:1653-1659. |
| [4] | Salthouse TA.When does age-related cognitive decline begin?[J].Neurobiol Aging,2009,30:507-514. |
| [5] | McCallum J.Measurement properties of the center for epidemiological studies depression scale:an Australian community study of aged persons[J].Gerontologist,1995,50:S182-189. |
| [6] | Wu Y,Pang Z,Zhang D,et al.A cross-sectional analysis of age and sex patterns in grip strength,tooth loss,near vision and hearing levels in Chinese aged 50-74 years[J].Arch Gerontol Geriatr, 2012,54:e213-220. |
| [7] | Wu Y,Zhang D,Pang Z,et al.Gender-specific patterns in age-related decline in general health among Danish and Chinese:a cross-national comparative study[J].Geriatr Gerontol Int,2012, 12(3):431-439. |
| [8] | Burstrom B,Fredlund P.Self rated health:Is it as good a predictor of subsequent mortality among adults in lower as well as in higher social classes?[J].J Epidemiol Community Health,2001,55: 836-840. |
| [9] | Murata C,Kondo T,Tamakoshi K,et al.Determinants of self-rated health:Could health status explain the association between self-rated health and mortality?[J].Arch Gerontol Geriatr,2006,43: 369-380. |
| [10] | DeSalvo KB,Nicle B,Kristi R,et al.Mortality prediction with a single general self-rated health question.A meta-analysis[J].J Gen Intern Med,2006,21:267-275. |
| [11] | Taekema DG,Gussekloo J,Maier AB,et al.Handgrip strength as a predictor of functional,psychological and social health.A prospective population-based study among the oldest old[J].Age Ageing, 2010,39:331-337. |
| [12] | Takai Y,Ohta M,Akagi R,et al.Sit-to-stand test to evaluate knee extensor muscle size and strength in the elderly:a novel approach[J].J physiol Anthropol,2009,28:123-128. |
| [13] | Liang MT,Cameron Chumlea WM.Balance and strength of elder Chinese men and women[J].J Nutr Health Aging,1998,2: 21-27. |
| [14] | 杨敬源,黄文湧,杨星,等.贵阳市城区老年人认知功能障碍及影响因素分析[J].中国公共卫生,2008,24(10):1167-1168. |
| [15] | 高至旭,盛尤荣,严和竣,等.上海地区老年抑郁症的流行病学调查[J].中国神经精神疾病杂志,1992,18(2):278-280. |
| [16] | Gureje O,Afolabi E.Epidemiology of major depressive disorder in elderly Nigerians in the Ibadan study of ageing:a communitybased survey[J].Lancet,2007,370:957-964. |
| [17] | 李淑然,陈昌惠,张维熙,等.北京市城市社区老年期痴呆和老年抑郁症患病率调查[J].中国心理卫生杂志,1999,13(2): 266-268. |
| [18] | Steffens DC,Skoog I,Norton MC,et al.Prevalence of depression and its treatment in an elderly population:The Cache County Study[J].Arch Gen Psychiatry,2000,57:601-607. |
| [19] | Chong MY,Chen CC,Tsang HY,et al.Community study of depression in old age in Taiwan.Prevalence,life events and socio-demographic correlateds[J].Br J Psychiatry,2001,178:29-35. |