 2009, Vol. 25
2009, Vol. 25

2. 辽宁省疾病预防控制中心
近年来,随着气象和死亡资料的健全,日气象资料与日死亡关系的研究日益受到广泛关注,但多集中于极温对健康影响的研究〔1-4〕。半参数一般递加模型(semi-parametric generalized additive model,GAM)的引入,为研究日均气温与日死亡率间的关联提供了良好的途径〔3, 4〕。目前,我国日平均气温与日呼吸系统疾病死亡关系的研究报道较少。辽宁省沈阳市四季分明,气温变化范围为50 ℃左右,非常适合分析日平均气温与死亡率的关系。本研究利用沈阳市1992~2000年3 288 d的气象和死亡资料,分析日平均气温对呼吸系统疾病死亡的短期影响。现报告如下。
1 对象与方法 1.1 对象死亡数据来自辽宁省疾病预防控制中心死因统计资料。死亡原因采用第9版国际疾病标准分类编码(ICD-9)进行分类,呼吸系统疾病死亡编码为460.0-519.9,慢性阻塞性肺疾患(COPD)为490.0-496.9,肺炎为480.0-486.9,呼吸系统其他疾病为510.0-519.9。日气象数据来自沈阳市气象台的每日监测数据,主要包括气温、水汽压、风速和湿度等指标。
1.2 方法采用半参数一般递加模型(Generalized Additive Models,GAM)〔5〕,调整季节、工作日、时间趋势、气压和空气湿度等因素,运用一般化互校验方法(Generalized cross-validation,GCV)选择平滑函数的自由度,分析呼吸系统疾病与日均呼吸系统死亡率间关联〔4〕。
1.3 统计分析采用SAS 8.02软件进行统计分析。
2 结果 2.1 基本情况沈阳市1992~2000年日均气温8.7 ℃,日均最低为-21.2 ℃,最高为29.9 ℃,9年间呼吸系统疾病共死亡24 302人,其中COPD 18 767人,占77.2%;肺炎2 031人,占8.4%;呼吸系统其他疾病3 214人,占13.2%。呼吸系统疾病日均死亡7.4人,最低为0人/d,最高为39人/d; ≥65岁年龄组明显高于 < 65岁年龄组,COPD日均死亡5.7人,肺炎日均死亡0.6人。
2.2 日死亡率调整值与日均气温关系(图 1)

|
图 1 日均呼吸系统疾病死亡率调整值与日均气温关系 |
日均呼吸系统疾病死亡率与日平均气温间呈反“J”型关系,日均死亡率在22.3 ℃最低(最适温度),在最适温度两侧的最低和最高气温时分别达到峰值。低温对死亡的影响更显著,最高气温时的日均死亡率相当于日均气温10 ℃时的死亡率,死亡率随气温降低明显升高。≥65岁年龄组的日均死亡率明显高于 < 65岁年龄组,死亡率随气温变化的改变量(斜率)也高于 < 65岁年龄组。COPD死亡率随气温的降低呈单调递增趋势; 肺炎和呼吸系统其他疾病死亡率的最适温度分别为18.5和19.5 ℃,高温区间死亡率上升曲线的斜率明显高于低温区间曲线的斜率。
2.3 超过或低于最适气温1 ℃时日均呼吸系统死亡率改变情况(表 1)| 表 1 日平均气温与呼吸系统疾病死亡的单因素回归分析 |
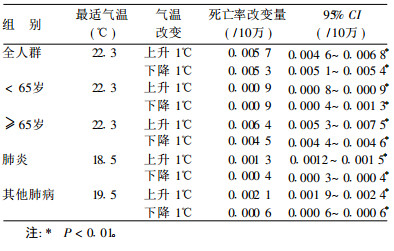
最适温度两侧每升降1 ℃,日呼吸系统死亡率增幅接近,≥65岁年龄组死亡率增幅分别为 < 65岁年龄组的7.1倍和5.0倍; COPD日均死亡率随气温增加单调递减,气温每上升1 ℃,死亡率下降0.000 3/10万; 肺炎和其他肺病的最适温度分别为18.5和19.5 ℃,最适温度以上每升高1 ℃的死亡率增幅分别为最适温度以下每降低1 ℃死亡率增幅的3.3倍和3.5倍。
3 讨论沈阳市呼吸系统疾病日均死亡率在22.3 ℃时最低,与日平均气温呈反“J”型关系。不但表明极端气温对呼吸系统疾病日均死亡率的影响, 也表明非极温状态下的气温变化也可能造成人群死亡率的增加,与国内外研究结果〔3, 4, 6〕相近。低温对呼吸道疾病死亡的总体影响大于高温。但肺炎对高温区的气温变化更敏感,与有关研究结果一致〔7, 8〕。COPD死亡率随气温的降低呈单调递增趋势,显示低温对COPD死亡的影响,可能与冷空气刺激体表,引起副交感神经反应,从而导致支气管收缩,加重通气障碍有关〔9〕。≥65岁年龄组老年人的日均死亡率随气温变化的改变幅度明显高于 < 65岁年龄组,显示出老年呼吸系统疾病患者对气温升降变化的高度敏感性,与其他研究结果一致〔7, 8〕。本研究日均气温变化导致呼吸系统疾病死亡率改变水平高于国外相似研究〔10〕,可能与沈阳市一年内日均气温变化范围大于国外同类研究有关。
| [1] | 刘学恩, 李群娜, 赵宗群. 气温及冷空气对武汉市心脑血管疾病死亡率的影响[J]. 中国公共卫生, 2002, 18(8) : 948–950. |
| [2] | 程锦泉, 刘建平, 张仁利. 深圳市脑卒中发病与气温关系[J]. 中国公共卫生, 2007, 23(8) : 970–971. |
| [3] | Therese FM, Gary AN, Jane QK, et al. Associations between air pollution and mortality in Phoenix, 1995-1997[J]. Environ Health Perspect, 2000, 108 : 347–53. DOI:10.1289/ehp.00108347 |
| [4] | 于连政, 井立斌, 冯毅平, 等. 沈阳市1992-2000年间日平均气温与居民循环系统疾病日均死亡率的关系[J]. 中国慢性病预防与控制, 2008, 16(3) : 221–224. |
| [5] | Hastie TJ, Tibshirani RJ. Generalized additive models[M].London: Chapman and Hall, 1990. |
| [6] | Frank CC, Karlyn SH, Jonathan M, et al. Temperature and mortality in 11 cities of the Eastern United States[J]. American Journal of Epidemiology, 2002, 155(1) : 80–87. DOI:10.1093/aje/155.1.80 |
| [7] | Keatinge WR, Donaldson GC, Cordioli E, et al. Heat related mortality in warm and cold regions of Europe: observational study[J]. BMJ, 2000, 321 : 670–673. DOI:10.1136/bmj.321.7262.670 |
| [8] | Koskela HO, Koskela AK, Tukiainen HO. Bronchoconstriction due to cold weather in COPD:The roles of direct airway effects and cutaneous reflex mechanisms[J]. Chest, 1996, 110(3) : 632–636. DOI:10.1378/chest.110.3.632 |
| [9] | Michelozzi P, de Donato F, Bisanti L, et al. The impact of the summer 2003 heat waves on mortality in four Italian cities[J]. Euro Surveill, 2005, 10(7) : 161–165. |
| [10] | Patrick GG, Douglas WD, Luke C. Cause-specific mortality and the extended effects of particulate pollution and temperature exposure[J]. Environ Health Perspect, 2004, 112 : 179–185. |