 2016, Vol.29
2016, Vol.29



Objective This study was designed to evaluate the prevalence of thyroid nodules (TNs) and its relationship with urine iodine concentrations (UICs) after the regional rapid economic growth and lifestyle changes.
Methods A cross-sectional survey was conducted in the general population aged 15-69 years. A questionnaire regarding general and personal characteristics and relevant information was administered. Ultrasonography of the thyroid was performed,and serum triiodothyronine (T3),tetraiodothyronine (T4),serum thyroid stimulating hormone (TSH),free triiodothyronine (FT3),free tetraiodothyronine (FT4),thyroglobulin antibody (TgAb),thyroid peroxidase antibody (TPOAb),and TSH receptor antibody (TRAb) levels were measured for each individual subject.
Results The prevalence rates of TNs in the whole population,females and males were 27.76%,34.04%,and 21.60%,respectively. The prevalence of multiple nodules increased with age,whereas the prevalence peaks differed between males and females. The median UICs in the whole population and females with non-TNs were higher than those of subjects with TNs (P=0.0035, P=0.0068). The median UICs in subjects with a single TN were higher than those in subjects with multiple TNs (P=0.0164,P=0.0127). The result showed a U-shaped curve relationship between UIC and prevalence of TNs. The prevalence of TNs was the lowest when the UIC was 140-400 µg/L.
Conclusion The prevalence of TNs was nearly 30% and increased with age. The relationship between UIC and prevalence of TNs is U-shaped,with an increase in risk when the UIC was <140 µg/L and >400 µg/L. Very low or high UIC levels need attention and correction.
I ncreasing age,iodine deficiency,female sex,and a history of head and neck radiation increase the risk of hyroid nodules (TNs)[1, 2]. The prevalence of palpable TNs has been estimated to be approximately 5% in women and 1% in men living in iodine-sufficient areas of the world[3, 4]. Moreover,nodules were incidentally found with a prevalence of 19%-67%[5] on ultrasonography and 8.2%-65% based on autopsy data[6, 7].
During the past several decades,an increasing number of outpatient cases of TNs and cancer have been reported by clinicians in Shanghai,China. An increasing incidence of thyroid cancer has been reported in some European countries[8, 9],the United States[10],and some regions of China[11]. Moreover,the International Agency for Research on Cancer (IARC)[12] has reported that the incidence of thyroid cancer has increased in most other countries and areas. A pooled analysis of individual data from 12 case-control studies conducted in seven countries,which provided more precise estimates than previously available on the relationship between benign thyroid diseases and mostly well-differentiated,nonmedullary thyroid cancer,showed that benign nodules/adenomas are the strongest risk factors for thyroid cancer besides radiation in childhood[13]. The analysis revealed that women with a history of benign nodules or adenomas have an approximate 30-fold increased risk for thyroid cancer. Elevated risks are observed in men and women and in relation to both major histological thyroid cancer types. No significant heterogeneity across geographic areas or across studies has been observed. The excess risk is greatest within 2-4 years prior to thyroid cancer diagnosis; however,elevated odds ratios (ORs) also reveal a risk of 10 years or more prior to cancer[14]. To understand the current status in the region of Shanghai,epidemiological studies exploring numerous factors influencing thyroid disorders were conducted.
Rapid economic development and the consequent improvement in living conditions,nutrition,and health care have resulted in declines in deaths due to infectious diseases,which in turn led to increases in chronic diseases in China[15] with the rapid economic development and urbanization in Shanghai,which is one of the biggest and most developed cities in China and has experienced an epidemiological transition shifting from infectious to chronic diseases in a much shorter time than several other cities,people have been facing remarkable variations in pollution,nutrition,lifestyle,and stress[16, 17, 18]. The incidence rate of thyroid cancer in Shanghai increased from 1.64 per 100,000 in the 1981-1983 period to 2.96 per 100,000 in the 1999-2001 period. The incidence rate of thyroid cancer increased rapidly and reached 13.65 per 100,000 in the whole population and 20.6 per 100,000 among females in 2010. Thyroid cancer was ranked as the third most commonly diagnosed cancer in females in Shanghai in 2010[19]. The correlation between TNs and cancer remains unclear. Whether the abovementioned factors and which of these factors are involved in the increase of thyroid cancer in Shanghai population are not clear. Moreover,no study has yet surveyed the prevalence and condition of TNs in a normal population in Shanghai,which is critical for public health because of its potential risk of serious clinical outcomes.
Shanghai has been following implementation of universal salt iodization to prevent iodine deficiency diseases since 1996. The median urine iodine concentration (UIC) increased from 72.3 μg/L (urban) and 52.2 μg/L (suburban) before universal salt iodization to 179.2 μg/L in 2014. Correlation between urinary iodine level and TN is an important aspect that needs to be explored.
The aims of this study were to reveal the incidence of TNs in a normal population aged from 15 to 69 years in Shanghai and to investigate the relationship between the incidence of TN and iodine nutrition status. The results obtained from this study would provide us a basis to understand the current epidemiological status of thyroid disorders,thereby advancing government policies on disease control.
Materials and Methods PopulationThe survey,which aimed to assess the prevalence of thyroid diseases in the whole population of Shanghai after the introduction of salt iodization for 13 years,was conducted from September 2009 to December 2009. A multistage,stratified random sampling scheme was used to recruit participants from the general population. Individuals aged from 15 to 69 years were randomly recruited from selected resident groups in each neighborhood or village. All residents who had been living in Shanghai for more than 12 months were initially eligible for inclusion. Subjects who could not complete the survey independently,such as those with serious mental disorders or dementia,those who were deaf or bedridden,or those who had hepatitis (infectious period),active tuberculosis,AIDS,or other infectious diseases,were excluded. The sampling method has been described in detail in our previous article[20].
MethodsA questionnaire was designed to obtain general and personal information,which included sex,age,nationality,socioeconomic status,physical activity,personal or family history of thyroid diseases (including time of diagnosis),and intake of iodine supplements. The questionnaire was administered face-to-face by trained staff in the respondents’ homes. All questionnaires were immediately checked for quality and completeness after the home interview. Ultrasonography of the thyroid was performed for the participants. Thyroid ultrasound examination was performed by specially trained technicians by using equipment model LOGIQE9 with 7.5-MHz linear transducers,GE. Subjects were examined in the supine position with the neck hyperextended. Then,5 mL of fasting venous blood sample was drawn from the subjects. Serum was centrifuged and stored at -70 °C. Thyroid TSH,FT3,FT4,TgAb,and TPOAb were measured with the chemiluminescence immunoassay method,using electrochemical luminescence (Roche E601,Germany). TRAb was measured by using a radioimmunoassay[21]. All participants provided written informed consent[20].
Diagnostic CriteriaSingle nodule was defined as a normal thyroid volume with a single nodule >3 mm in diameter,and multiple nodules were defined as a normal thyroid volume with two or more nodules >3 mm in diameter[21]. The diagnostic criteria for other thyroid diseases have been described in our previous study[18].
Statistical AnalysisSAS statistical software version 9.1.3 (SAS Institute) was used to compute the prevalence,standard error,and 95% CI estimates. To identify variables related to TNs and estimate ORs,we fitted logistic regression models separately for women and men. Risk factors found to be statistically significant (P value <0.05) in single-variable analysis,as well as basic demographic variables considered to be potential indicators such as age,income,and nationality,were included in multivariable regression modeling. To compare the estimated prevalence between the populations,we used two-sided t tests as recommended in other studies[22]. To confirm the significance testing of the difference in prevalence between time periods,χ2 analyses were performed and the corresponding P values were reported. Results were considered statistically significant if the P value was less than 0.05.
Results Summary of Samples ObtainedThe details of potential samples,the responses and samples obtained,and the number of satisfactory samples for general population,pregnant women,and lactating women are listed in Table 1.
|
|
Table 1. A Summary of the Samples Collected and Investigations Performed in the General Population and the Two Subgroups |
Assessment of the representative features of current sample. Myers’ index >60 in a sample indicates that there is a serious age preference. However,Myer’s index was only 16.92 in the whole sample in this study (male: 17.04,female: 18.76). Thus,our sample had no age preference. There were differences in age distribution when all the sampled participants were compared to the whole population,but no differences were observed when only those aged 20 years or above were compared. This may be due to oversampling for those aged 5-19 years. We used the age of the whole population in Shanghai to adjust the estimated iodine status. The male-to- female ratio was 1.07 in our sample,similar to the sex ratio in the corresponding age range of the whole population in Shanghai (χ2=1.87,P=0.1713)[20].
The study examined a representative sample of the Shanghai population. Overall,5144 participants,including 2547 females and 2597 males who underwent thyroid ultrasonography and for whom urine and blood samples were collected,were included in our study.
Prevalence of TNs in Different Genders and Age GroupsThe prevalence rates of TNs in all subjects,females,and males were 27.76%,34.04%,and 21.60% respectively. The ratio of prevalence between the genders was 3:2 (female: 34.04% vs. male: 21.60%). The prevalence increased along with increase in age. Subjects aged from 15 to 20 years had the lowest prevalence and subjects aged from 60 years had the highest prevalence (Table 2).
|
|
Table 2. The Prevalence of Thyroid Nodules in Different Populations |
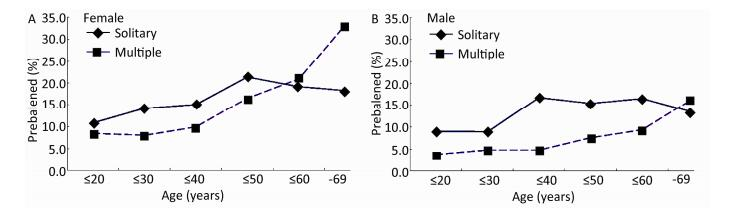
The prevalence of solitary TNs increased in women with age up to 50 years,from 10.76% to 21.36%,but decreased from 21.36% to 18.24% among those aged 51-69 years. However,the prevalence of multiple TNs was 8.50% in subjects aged below 20 years,which then slightly decreased to 8.05% in subjects aged 20-30 years. Then,the prevalence increased to 33.24% with increase in age in the group aged 60-69 years (Figure 1).

|
Download:
|
| Figure 1. The prevalence of single or multiple thyroid nodules. | |
{kind=link}
The prevalence of solitary TNs in men fluctuated with increase in age. The overall trend was that it increased to the peak of around 16.00% from 9.00% in subjects aged 30-60 years and decreased subsequently. Men younger than 30 years of age had the lowest prevalence (approximately 9.00%) and those aged 30-40 years had the highest prevalence rate (16.71%). The prevalence of multiple TNs increased along with increase in age. Subjects below 20 years of age had the lowest prevalence,and those aged from 60 years higher had the highest prevalence (Figure 1).
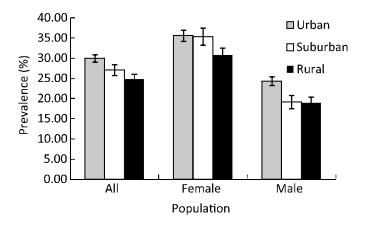
Prevalence of TNs in Urban,Suburban,and Rural AreasThe prevalence rates of TNs among subjects living in urban,suburban,and rural areas of Shanghai were 29.92%,27.03%,and 24.78%,respectively. A statistically significantly higher prevalence was found in urban subjects than in rural subjects (P<0.001).
The prevalence rates of TNs among women living in urban,suburban,and rural areas were 35.55%,35.32%,and 30.77%,respectively. A statistically significantly higher prevalence was found among urban-dwelling women (P<0.001) and suburban-dwelling women (P<0.001) than in rural-dwelling women (Figure 2).

|
Download:
|
| Figure 2. The prevalence of thyroid nodules in urban,suburban,and rural areas. | |
{kind=link}
As for men,24.29%,19.13%,and 18.98% of those living in urban,suburban,and rural areas,respectively,were found with TNs. Meanwhile,a statistically significantly higher prevalence was also found in urban-dwelling men than in rural-dwelling men (P<0.001) (Figure 2).
Other Thyroid Diseases in TN and Non-TN GroupsIt was observed that 84.78% of women and 86.99% of men had normal thyroid function. Hyperthyroidism,subclinical hyperthyroidism,hypothyroidism,subclinical hypothyroidism,and graves’ disease were found in both TN and non-TN groups. Subclinical hypothyroidism had the highest prevalence in both groups and both genders. No statistically significant differences in the prevalence of other thyroid diseases were observed in both groups with and without TNs (Table 3).
|
|
Table 3. Other Thyroid Diseases in Groups with and without Thyroid Nodules |
UICs with and without TNs showed a positively skewed distribution. The median UICs in the non-TN and TN groups were 143.1 µg/L and 135.4 µg/L,respectively. The median UICs in the non-TN group were higher than those in the TN group (P=0.0035). The median UICs in the non-TN group with intake of iodized salt were higher than those in the TN group (P=0.003). There was no statistically significant difference in the median UICs between the non-TN group with intake of non-iodized salt and the TN group (Table 4).
|
|
Table 4. Comparison of Urine Iodine Concentrations (UICs) between Participants with and without Thyroid Nodules |
UICs with solitary and multiple TNs showed a positively skewed distribution. The median UICs in the single and multiple TN groups were 139.8 µg/L and 130.6 µg/L,respectively. The median UICs in the single TN group were higher than those in the multiple TN group (P=0.0164). The median UICs in the single TN group with intake of iodized salt were higher than those in the multiple TN group (P=0.0174). No statistically significant difference in the median UICs was found between the single TN group with intake of non-iodized salt and the multiple TN group (Table 5).
|
|
Table 5. Risk Factors of Thyroid Nodules in Women |
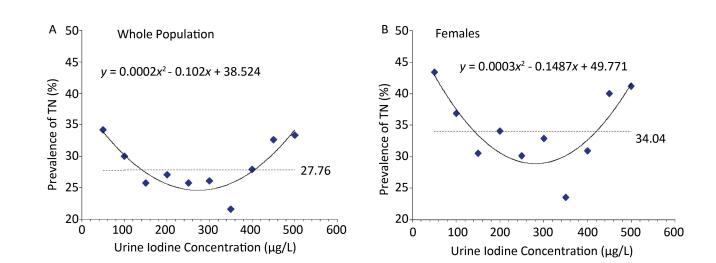
The prevalence of TNs decreased from 34.19% to 25.75% when the UIC <250 µg/L,but it slightly increased to 26.1% when the UIC increased from 250 µg/L to 300 µg/L. The prevalence of TNs increased from 21.64% to 33.33% when the UIC increased from 301 µg/L to 500 µg/L. The prevalence of TNs was lower than the average prevalence when the UIC was between 140 and 400 µg/L (Figure 3).

|
Download:
|
| Figure 3. The relationship between urine iodine and the prevalence of TN. | |
{kind=link}
UICs in females with non-TNs,single TN,and multiple TNs showed a positively skewed distribution. The median UICs in females with non-TNs were higher than those in the TN group (P=0.0068). Median UICs in the solitary TN group were higher than those in the multiple TN group (P=0.0127) (Tables 4,5). UICs in males with non-TNs,single TN,and multiple TNs also showed a positively skewed distribution. The median UICs were similar in the non-TN,single TN,and multiple TN groups (Tables 4,5).
Relationship between UICs and Prevalence of TN in Different GendersThe prevalence of TNs in females decreased from 43.41% to 30.54% when the UIC was <150 µg/L,while it increased from 23.53% to 41.18% when the UIC increased from 301 µg/L to 500 µg/L. The prevalence of TNs was lower than the average prevalence when the UIC was between 140 and 410 µg/L (Figure 3).
No statistically significant difference in the UIC and prevalence of TNs was found in males.
Comparison of UICs in Urban,Suburban,and Rural AreasThere was no statistically significant difference observed in this study as the median UIC levels were 132.47 μg/L,146.71 μg/L,and 145.41 μg/L among the urban,suburban,and rural subjects,respectively. The corresponding levels in urban,suburban,and rural females were 137.59 μg/L,151.13 μg/L,and 149.33 μg/L,while those in urban,suburban,and rural males were 127.34 μg/L,139.40 μg/L,and 140.90 μg/L,respectively.
DiscussionBased on the data collected from a large sample size survey in Shanghai,we evaluated the epidemiological status of TNs in the whole population,women,and men and its relationship with UICs. To our knowledge,this is an advanced report on the prevalence and predictors of TNs under the dramatic dietary and socioeconomic changes in the present decades in China.
Overall,27.76%,34.04%,and 21.60% population,women,and men,respectively. Several previous studies have reported that the prevalence of TNs ranged from 19.0% to 34.7% diagnosed by high-resolution ultrasound (HRUS)[23, 24, 25]. The prevalence of thyroid nodularity in Shanghai residents was consistent with the range reported by other studies. One study conducted in north China by Dr. Teng reported that the prevalence rates of TNs were 17.0%,17.1%,and 17.4% in places with mildly deficient,more than adequate,and excessive iodine intake during 1999-2004[26]. The different criteria used for the definition of nodularity,iodine fortification,the nationalities,and age might account for this discrepancy[27, 28]. TNs were defined as >3 mm in our study and >5 mm in the study conducted by Dr. Teng[24]. Age of the study population,from 15 to 69 years,was similar in both studies; however,the sample size of our study was smaller than that of Teng’s study,and the living environment,lifestyle,and rhythm of the subjects were also very different in these two studies. These factors perhaps have led to the different prevalence rates of TNs. The prevalence of TNs was also influenced by iodine intake. A Danish investigation observing a large population before and after iodine fortification reported that even small changes in iodine intake significantly influence TN incidence[29]. There is a similarity in Shanghai as the mandatory iodine supplementation has been in place for 13 years. However,the mandatory iodine supplementation implemented in the counties in Teng’s study was only less than 6 years. This might also contribute to the discrepancy of the prevalence in these two studies.
An increase in the prevalence of TNs with increase in age has been consistently observed,at least up to the age of 69 years,in some other studies[30, 31, 32, 33]. Our study included enough observations to allow stratification and showed that the prevalence of multiple nodules increased with age,a similar trend found in previous studies[34, 35]. In our study,the prevalence of solitary nodules reached the peak among women in their forties and men in their thirties and then declining thereafter,whereas previous studies showed a relatively constant prevalence of solitary nodules in different age groups[32, 33].
In this study,both gender groups showed a higher prevalence of TNs in the urban area than in the rural area. To our knowledge,these findings have not yet been reported so far by other studies. The differences in the prevalence of TNs between urban and rural areas might be accounted for by the differences in the dietary structure,environment pollution,socioeconomic status,and stress. Several studies have reported that thyroid disorders are associated with environmental factors,socioeconomic indicators,and psychiatric factors[36, 37, 38]. These factors might partially contribute to the discrepancy in the prevalence of TNs between urban and rural areas.
The prevalence of other thyroid disorders in participants with or without TNs was similar in both women and men,which could indicate that thyroid dysfunction might be independent of TNs.
Based on the data analysis on the relationship between UICs and thyroid disorders,our study showed that the median UICs were the highest in the non-TN group and the lowest in the multiple TN group in all populations and females who had non-TNs,single TN,and multiple TNs. Iodine deficiency results in insufficient thyroid hormone synthesis,and because iodine is an essential element for the synthesis of thyroid hormones,the TSH increases due to the feedback regulation of the hypothalamus-pituitary-thyroid axis,leading to lower thyroxine (T4) levels. This leads to compensatory hyperplasia and hypertrophy in the thyroid follicular cells. These follicular cells easily form solitary or multiple nodules after certain period of time. In this study,the median UICs in the TN group were lower than those in the non-TN group in the whole population and females. Further study and investigations are needed to clarify whether the occurrence and development of TNs lead to decrease in urinary iodine level or the lower urinary iodine level initiates the formation of TNs. Females were more sensitive to levels of hormones and the changes of high and low iodine intake. They are more likely to suffer from TNs than men. The results from this study comply with the results reported by other authors[39, 40, 41, 42, 43].
Excessive iodine supplementation or iodine deficiency will cause thyroid disorders. In our study,the relationship of UIC with the prevalence of TNs showed a ‘U’-shaped curve in all subjects and females. The prevalence of TNs decreased with the increase in UIC,when the UIC was <140 µg/L. The prevalence of TNs increased with the increase in UIC,when the UIC was >400 µg/L in all subjects and >410 µg/L in females. The lowest prevalence of TNs was observed when the UIC level was between 140 and 400 µg/L. Laurberg et al. reported that the relationship between iodine intake level of a population and the occurrence of thyroid diseases is U-shaped,with an increase in risk from both low and high iodine intakes. The U-shaped bottom end is the most suitable for human existence[44]. This was also similar with the conclusion in our report.Iodine status is the mostimmediate measure of whether the thyroid gland has adequate iodineto function normally and protect the individual from the manifestationsof iodine deficiency or excess. The median urinary iodine concentration reflectsthe population status and is the indicator most commonly assessed[45]. The exact mechanism leading to thyroid diseases has not been clarified. This needs more studies to precisely define the limits of excessive iodine intake.
The strength of our study is that we conducted a systematic survey in a representative population in Shanghai to reveal the prevalence of TNs and the risk factors after several decades of iodization and rapid economic development with the accompanying dietary and lifestyle changes.
A limitation of our study is that some potential predictors,such as occupation,iodine intake,and body mass index,were not collected for analysis. The malignancy of TNs was not evaluated in our study,due to which we could not assess some of the cancer risk factors. Moreover,clinicians should carefully interpret these results when applying them in clinical practice,because of the unique nationality,geography,and time variations compared with other studies.
In conclusion,TNs are common clinical problems. The relationship between the urinary iodine level of a population and the occurrence of TNs is U-shaped,with an increase in risk from both low and high urinary iodine levels. Higher income and urban area might be potential predictors of TNs. Results of this prospective study clearly confirmed the incidence of TNs with different urinary iodine levels. The urinary iodine level of residents maintained in a safe range of 140-400 µg/L is the most suitable level to prevent the occurrence of TNs and avoid the side effects of iodine excess. Optimization of population iodine level is an important component of preventive health care to reduce the prevalence of thyroid disorders that could be implemented through government policies.
| 1. | Gharib H. Changing concepts in the diagnosis and management of thyroid nodules. Endocrinol Metab Clin North Am,1997; 26,777-800. |
| 2. | Rojeski MT,Gharib H. Nodular thyroid disease: evaluation and management. N Engl J Med,1985; 313,428-36. |
| 3. | Tunbridge WMG,Evered DC,Hall R,et al. The spectrum of thyroid disease in a community: The Whickham Survey. Clin Endocrinol (Oxf),1977; 7,481-93. |
| 4. | Vander JB,Gaston EA,Dawber TR. The significance of nontoxic thyroid nodules. Ann Intern Med,1968; 69,537-40. |
| 5. | Bruneton JN,Balu-Maestro C,Marcy PY,et al. Very high frequency (13 MHz) ultrasonographic examination of the normal neck: detection of normal lymph nodes and thyroid nodules. J Ultrasound Med,1994; 13,87-90. |
| 6. | Hull OH. Critical analysis of two hundred twenty-one thyroid glands: study of thyroid glands obtained at necropsy in Colorado. AMA Arch Pathol,1955; 59,291-311. |
| 7. | Mortensen JD,Woolner LB,Bennett WA. Gross and microscopic findings in clinically normal thyroid glands. J Clin Endocrinol Metab,1955; 15,1270-80. |
| 8. | Colonna M,Grosclaude P,Remontet L,et al. Incidence of thyroid cancer in adults recorded by French cancer registries (1978-1997). Eur J Cancer,2002; 38,1762-8. |
| 9. | Montanaro F,Pury P,Bordoni A,et al. Unexpected additional increase in the incidence of thyroid cancer among a recent birth cohort in Switzerland. Eur J Cancer Prev,2006; 15,178-86. |
| 10. | Davies L,Welch HG. Increasing incidence of thyroid cancer in the United States,1973-2002. JAMA,2006; 295,2164-7. |
| 11. | Qian B,He M,Dong S,et al. Incidence and mortality of thyroid cancers in Tianjin from 1981 to 2001. Chin J Endocrinol Metab,2005; 21,432-4. |
| 12. | Torre LA,Bray F,Siegel RL,et al. Global cancer statistics,2012. CA Cancer J Clin,2015; 65,87-105 |
| 13. | Franceschi S,Preston-Martin S,Dal Maso L,et al. A pooled analysis of case-control studies of thyroid cancer.IV Benign thyroid diseases. Cancer Causes Control,1999; 10,583-95. |
| 14. | Preston-Martin S,Franceschi S,et al. Thyroid cancer pooled analysis from 14 case-control studies: what have we learned? Cancer Causes Control,2003; 14,787-9. |
| 15. | He J,Gu D,Wu X,et al. Major causes of death among men and women in China. N Engl J Med,2005; 353,1124-34 |
| 16. | Su C,Wang H,Zhang J,et al. Intergenerational differences on the nutritional status and lifestyle of Chinese residents. Wei Sheng Yan Jiu,2012; 41,357-62. (In Chinese) |
| 17. | Gong P,Liang S,Carlton EJ,et al. Urbanisation and health in China. Lancet,2012; 379,843-52. |
| 18. | Yang GH,Kong LZ,Zhao WH,et al. Emergence of chronic non-communicable diseases in China. Lancet,2008; 372,1697-705. |
| 19. | Shanghai Municipal Center for Disease Control and Prevention. Shanghai Cancer Report. Shanghai Municipal Center for Disease Control and Prevention,Shanghai,China. 2011. |
| 20. | Zou S,Wu F,Guo C,et al. Iodine Nutrition and the Prevalence of Thyroid Disease after Salt Iodization: A Cross-Sectional Survey in Shanghai,a Coastal Area in China. PLoS One,2012; 7,e40718. |
| 21. | Li QS. Ultrasound of Superficial Organs (Series of Ultrasound Physician Training). Beijing: People's Military Medical Press,2009; 61-77. |
| 22. | National Health and Nutrition Examination Survey.Hypothesis testing. http://www.cdc.gov/nchs/tutorials/nhanes/NHANES-Analyses/HypothesisTesting/hypothesis_testing_intro.htm.[2012-09-08] |
| 23. | Woestyn J,Afschrift M,Schelstraete K,et al. Demonstration of nodules in the normal thyroid by echography. Br J Radiol,1985; 58,1179-82. |
| 24. | Brander A,Viikinkoski P,Nickels J,et al. Thyroid gland: US screening in a random adult population. Radiology,1991; 181,683-7. |
| 25. | Bruneton JN,Balu-Maestro C,Marcy PY,et al. Very high frequency (13 MHz) ultrasonographic examination of the normal neck: detection of normal lymph nodes and thyroid nodules. J Ultrasound Med,1994; 13,87-90. |
| 26. | Teng W,ShanZ,TengX,et al.Effect of iodine intakeon thyroid diseases in China. N Engl J Med,2006; 354,2783-93. |
| 27. | Popoveniuc G,Jonklaas J. Thyroid nodules. Med Clin N Am,2012; 96,329-49. |
| 28. | Dean DS,Gharib H. 2008 Epidemiology of thyroid nodules. Best Pract Res Clin Endocrinol Metab,2012; 22,901-11. |
| 29. | Laurberg P,Jφrgensen T,Perrild H,et al. The Danish investigation on iodine intake and thyroid disease,DanThyr: status and perspectives. Eur J Endocrinol,2006; 155,219-28. |
| 30. | Ezzat S,Sarti DA,Cain DR,et al. Thyroid incidentalomas: prevalence by palpation and ultrasonography. Arch Intern Med,1994; 154,1838-40. |
| 31. | Aghini-Lombardi F,Antonangeli L,Martino E,et al. The spectrum of thyroid disorders in an iodine-deficient community: The Pescopagano survey. J Clin Endocrinol Metab,1999; 84,561-6. |
| 32. | Hampel R,Kulberg T,Klein K,et al. Strumapravalenz in Deutschland grosser als bisher angenommen. Med Klin,1995; 90,324-9. |
| 33. | Barrère X,Valeix P,Preziosi P,et al. Determinants of thyroid volume in healthy French adults participating in the SU.VI.MAX cohort.ClinEndocrinol (Oxf),2000; 52,273-8. |
| 34. | Knudsen N,Bulow I,Jorgensen T,et al. Goitre prevalence and thyroid abnormalities at ultrasonography. A comparative epidemiological study in two regions with slightly different iodine status.ClinEndocrinol (Oxf),2000; 53,479-85. |
| 35. | Knudsen N,Perrild H,Christiansen E,et al. Thyroid structure and size and two-year follow-up of solitary cold thyroid nodules in an unselected population with borderline iodine deficiency. Eur J Endocrinol,2000; 142,224-30. |
| 36. | Duntas LH. Environmental factors and thyroid autoimmunity. Ann Endocrinol (Paris),2011; 72,108-13. |
| 37. | Sprague BL,Warren Andersen S,Trentham-Dietz A. Thyroid cancer incidence and socioeconomic indicators of health care access. Cancer Causes Control,2008; 19,585-93. |
| 38. | Mizokami T,Wu Li A,El-Kaissi S,et al. Stress and Thyroid Autoimmunity. Thyroid,2004; 14,1047-55. |
| 39. | FENG Shang-yong,LIU Chao,LIU Xiao-yun,et al. An epidemiologic study of thyroid nofules among community population in Gaochun and Chuzhou of Jiangsu. Acta Universitatis Medicinalis Nanjing (Natural Science),2007; 26,717-20. |
| 40. | LI Shou-un,CAO Yun-sheng,SUN Song,et al. Analysis of the Prevalence of Thyroid Nodules and Its Risk Factors among Population. Zhejiang Preventive Medicine,2012; 24,4-5. (In Chinese) |
| 41. | Nix P,Nicolaides A,Coatesworth AP. Thyoid cancer review:presentation and investigation of thyoid cancer. Int J Clin Pract,2005; 59,1459-63. |
| 42. | Azizi G,Malchoff CD. Autoimmune thyroid disease: a risk factor for thyroid cancer. Endocr Pract,2011; 17,201-9. |
| 43. | Qian Biyun,Chen Kexin,He min,et al. The Survey on Thyroid Carcinoma Incidence in Urban District of Tianjin. Chinese Journal of Clinical Oncology,2005; 32,218-21. (In Chinese) |
| 44. | Laurberg P,Bülow Pedersen I,Knudsen N,et al. Environmental iodine intake affects the type of nonmalignant thyroid disease. Thyroid,2002; 11,457-69. |
| 45. | World Health Organization. Assessment of iodine deficiency disorders and monitoring theirelimination: a guide for programme managers. - 3rd ed:47. |