 2016, Vol.29
2016, Vol.29



Objective This study aimed to investigate the epidemiology of diabetes in adults from Shanghai,aged 35 and older,in 2013.
Methods We estimated the diabetes prevalence in a representative sample of 18,736 adults who were selected through a multistage stratified cluster sampling process. A standard questionnaire containing questions about demographic characteristics and lifestyle factors was distributed. After an overnight fast of at least 10 hours,a venous blood sample was collected from each participant. For each patient without a history of diabetes,another blood sample was drawn 120 min after an oral glucose tolerance test to identify undiagnosed diabetes and prediabetic condition.
Results Among Shanghai residents aged 35 and above,the overall weighted prevalence of diabetes was 17.6% [95% confidence interval (CI): 16.4%-18.8%]. The prevalences were 19.3% in men and 15.8% in women as well as 19.1%,15.4%,and 16.1% in urban,suburban,and rural residents,respectively. In addition,the weighted prevalence of prediabetes was 16.5% (95% CI: 15.3%-17.8%),with the prevalences of 16.5% in men,16.6% in women,15.2% in urban residents,18.0% in suburban residents,and 18.5% in rural residents. Among all patients with diabetes,68.1% (95% CI: 64.3%-71.6%) were aware of their status,63.5% (95% CI: 60.0%-66.9%) received diabetes treatment,but only 35.1% (95% CI: 32.4%-37.8%) had adequate glycemic control.
Conclusion In Shanghai,diabetes and prediabetes are highly prevalent. However,1/3rd of diabetes cases are undiagnosed,and the rate of glycemic control is low.
D iabetes prevalence has increased significantly in recent decades and is now reaching epidemic proportions worldwide. More and more people live with this condition. The most recent estimates from the International Diabetes Federation (IDF) indicated that 8.8% of adults,or 415 million people,had diabetes,and 75% of people with diabetes live in low- and middle-income countries. In addition,318 million adults have impaired glucose tolerance,which puts them at high risk of diabetes later in life[1]. Yet,with 193 million of cases,or nearly half (46.5%),of all diabetes cases currently undiagnosed,a large number of people with diabetes were progressing towards complications while unaware of the problem[1]. Inadequately managed diabetes increases the risk of disabilities,life-threatening complications from microvascular disease (affecting the kidneys,eyes,and limbs),and macrovascular disease (involving the coronary vascular,cerebrovascular,and peripheral vascular systems),which are the leading causes of death among people with diabetes. As a result,diabetes creates a huge economic burden for individuals and families,health care systems,and countries. Medicalexpenditures for people with diabetes have been reported to be 2- to 4-times higher than those for non-diabetics[2-3]. Diabetes was estimated to cause5.0million deaths and cost 673billion U.S. dollars in health spending (12% of the total spent worldwide) in 2015[1].
Several surveys have indicated that the prevalence of diabetes in the Chinese population has increased dramatically from 1.0% in 1980 to 11.6% in 2010,although sampling methods,screening procedures,and diagnostic criteria were different[4-8]. As a modern city in China,Shanghai has had a higher prevalence of diabetes over the past few decades with great change in lifestyle and environment for inhabitants[9, 10, 11]. However,information on control of diabetes in a large populationis scarce. Our study aimed to investigate epidemiological characteristics of diabetes,including the current prevalence and related risk factors,as well as to assess awareness and level of glycemic control of diabetics in Shanghai among adults aged 35 or older,in 2013.
METHODS Study ParticipantsThe data were sourced from the 2013 Shanghai Noncommunicable and Chronic Disease (NCD) Surveillance Program,which was conducted among permanent residents aged 15 and older over a period of at least 6 months. Representative samples were selected through a multistage stratified cluster sampling process. In the first stage,all 299 townships were divided into 3 types,according to the proportion of registered non-agricultural residents and rural-to-urban agricultural residents. In total,60 urban townships,30 suburban townships,and 30 rural townships were randomly sampled. In the second stage,4 residential areas or villages were then sampled from each selected township by probability proportion to size (PPS). In the final stage,2 residential groups (at least 50 families) were sampled from each village by a simple random sampling method,and a family member aged 15 and above from each family was selected using the KISH grid method. A total of 25,657 people were selected to participate in the survey. We estimated epidemiology of diabetes in 18,736 people aged 35 and older. The study protocol was approved by the ethical review committee of Shanghai Municipal Center forDisease Control and Prevention (SCDC). Written informed consent was obtained from all respondents.
Data CollectionA standard questionnaire administered by trained staff contained questions about demographic characteristics,medical history,and lifestyle risk factors. Body weight and height were measured while the subject was barefoot and in light clothing. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Waist circumference (WC) was measured with the participants standing,midway between the lower edge of the costal arch and the upper edge of the iliac crest. Overweight was defined as a BMI between 24.0 kg/m2 and 28.0 kg/m2,and obesity was defined as a BMI of 28.0 kg/m2 or more[12]. Central obesity was defined as a WC of 90 cm or more in men and 80 cm or more in women[13]. Blood pressure was measured 3 times consecutively,with a 1 min interval between measurements with the participant in a seated position after 5 min of rest by using an automated device HEM-7071,OMRON Healthcare (China) Co.,Ltd.
After an overnight fast of at least 10 h,a venous blood sample was collected from each participant. For each subject without a history of diabetes,a blood sample was drawn 120 min after an oral glucose tolerance test using a standard 75 g glucose solution. Plasma glucose level was measured using the glucose oxidase-peroxidase method.
To ensure overall quality,a quality control network composed of SCDC,the district CDC,and community health service centers was set up. The roles of all participants and associated responsibility were determined. A quality control system was developed and executed. All investigators and research staff underwent a training session on the use of standardized protocols and instruments for data collection. Only certified staff members were allowed to collect data. All study laboratories successfully completed a standardization and certification program. The laboratory equipment was calibrated,and blinded duplicate samples were used. All data were entered twice in a database and then compared and corrected for errors.
DefinitionsAccording to the World Health Organization diagnostic criteria[14],diabetes wasdefined as (1) self-reported diabetes,(2) fasting plasma glucose (FPG) level of 126 mg/dL (7.0 mmol/L) or higher,or (3)2 h plasma glucose level (2hPG) of 200 mg/dL (11.1 mmol/L) or higher. Impaired fasting glycaemia (IFG) was defined as (1) FPG levels between 110 mg/dL (6.1 mmol/L) and 126 mg/dL (7.0 mmol/L) and (2) 2hPG levels <140 mg/dL (7.8 mmol/L). Impaired glucose tolerance (IGT) was defined as (1) FPG levels <126 mg/dL (7.0 mmol/L) and (2) 2hPG levels between 140 mg/dL (7.8 mmol/L) and 200 mg/dL (11.1 mmol/L). Prediabetes (or impaired glucose regulation,IGR) was defined as IFG and/or IGF.
Awareness was defined as the proportion of individuals with self-reported diabetes among all patients with diabetes. Treatment was defined as the proportion of individuals taking diabetes therapy among all patients with diabetes. Control was defined as the proportion of individuals with HbA1c less than 7.0% among diabetes patients taking treatment. Management was defined as the proportion of individuals participating in community diabetes management among self-reported diabetes patients.
Statistical AnalysisAll statistical analyses were performed using SPSS software,version 17.0. With the exception of descriptive data and crude rate calculations,the other analyses were weighted to represent the Shanghai adult population aged 35 and older. Weighted coefficients,which were used for the complex sampling point value of prevalence,were derived from the survey sampling scheme,which was the reciprocal of the probability of a particular individual selected,and a post-stratification factor that adjusted for age and sex in accordance with 2010 Shanghai population census data. Descriptive data are presented as means (95% CI). The crude,weighted prevalence (95% CI) of diabetes,prediabetes,and subtypes based on various criteria are described for the whole population and subgroups. The weighted proportion of awareness,treatment,control,and management were generated for the whole population and subgroups. Chi-squared tests were conducted to test differences in prevalence based on sex,age,location,and other variables. Odds ratios (ORs) for diabetes and prediabetes were calculated for trend based on age,BMI,and WC as continuous variables by univariate logistic regression. Logistic regressionanalyses were used to assess the association of demographic,lifestyle,and physical factors with the ORs of diabetes and prediabetes. All P values are two-tailed,P <0.05 was considered statistically significant.
RESULTSIn our study,18,736 individuals were included in the final analysis. There were 7504 men (40.1%) and 11,232 women (59.9%). The general characteristics and risk factors of the study population are presented in Table 1.
|
|
Table 1. Characteristics of Shanghai Adults Aged 35 and Older |
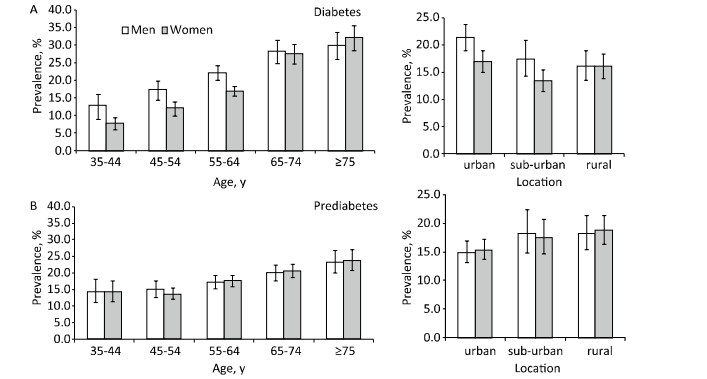
In Shanghai residents aged 35 and older,the weighted prevalence of diabetes was 17.6% (95% CI: 16.4%-18.8%),with the prevalence in men (19.3%) being higher than that in women (15.8%) (χ2=39.98,P<0.001). The self-reported diabetes weighted prevalence was 12.0% (95% CI: 10.8%-13.2%),with the prevalence of 13.3% in men and 10.6% in women (χ2=30.89,P=0.001). The prevalence of total diabetes differed significantly based on location (P<0.05) and education group (P<0.001),as did the rate of self-report diabetes (Table 2 and Figure 1). Furthermore,total diabetes prevalence increased with age (OR=1.04,95% CI: 1.04-1.05),BMI (OR=1.14,95% CI: 1.11-1.16),and WC (OR=1.06,95% CI: 1.05-1.07).

|
Download:
|
| Figure 1. Weighted prevalences of diabetes (A) and prediabetes (B) in Shanghai adults aged 35 and older,according to age groups and locations (%). (Error bars indicate 95% confidence intervals). | |
{kind=link}
|
|
Table 2. Crude and Weighted Prevalences (95% CI) of Diabetes among Shanghai Adults Aged 35 and Older |
The overall weighted prevalence of prediabetes was 16.5% (95% CI: 15.3%-17.8%),with prevalences of 16.5% in men and 16.6% in women,15.2% in urban residents,18.0% in suburban residents,and 18.5% in rural residents. No significant differences were found among the weighted prevalences based on sex (χ2=0.01,P=0.943) or location (χ2=29.90,P=0.052) (Table 3 and Figure 1),but prevalence increased with age (OR=1.03,95% CI: 1.02-1.03),BMI (OR=1.12,95% CI: 1.09-1.14),and WC (OR=1.04,95% CI: 1.03-1.05). The weighted prevalences of IFG and IGT were 5.1% (95% CI: 4.4%-5.9%) and 11.4% (95% CI: 10.4%-12.5%).
|
|
Table 3. Crude and weighted prevalences (95% CI) of IFG,IGT,and IGR among Shanghai adults aged 35 and older |
The weighted proportion of awareness was 68.1% (95% CI: 64.3%-71.6%),with 68.7% in men and 67.3% in women (χ2=0.84,P=0.558). Among all diabetic patients,63.5% of patients (95% CI: 60.0%-66.9%) were receiving treatment,with 63.8% of men and 63.1% of women receiving treatment (χ2=0.20,P=0.778). For all treatments,the weighted rate of oral medication was the highest (76.1%),and the proportions of patients using nutrition therapy,physical activity,glucose monitoring,and insulin were lower (41.7%,26.3%,24.6%,and 12.7 %,respectively). Among all patients,only 35.1% of individuals (95% CI: 32.4%-37.8%) had their HbA1c controlled under 7.0%,33.6% of men and 36.8% of women (χ2=11.43,P=0.075). The weighted proportions of diabetes awareness,treatment,and control differed in urban,sub-urban,and rural residents (P<0.05). The weighted rate of diabetes management was 46.8% (95% CI: 40.5%-53.1%),which was higher in women (52.1%) than in men (42.5%) (χ2=23.33,P=0.007). The weighted prevalences of awareness,treatment,control,and management were all different significantly among age groups (Table 4).
|
|
Table 4. Weighted awareness,treatment,control,and management rates (95% CI) of diabetes among Shanghai adults aged 35 and older |
By logistic regression analysis,overweight,obesity,central obesity,insufficient activity,and elevated systolic blood pressure were all significantly associated with increased risk of diabetes after adjusting for sex,age,and education. In addition,overweight,obesity,central obesity,and elevated systolic blood pressure also positively correlated with an increased risk of prediabetes (Table 5). Urban residence,cigarette smoking,alcohol consumption,and diastolic pressure were not significantly associated with risk of diabetes or prediabetes.
|
|
Table 5. Risk factors for diabetes and prediabetes in Shanghai adults aged 35 and older |
Diabetes has become a major public health problem in the general population of China. Previous studies indicated that China is now among the countries with the highest diabetes prevalence in Asia and has the largest absolute diabetes population in the world[1],which results in a considerable impactcaused by diabetes. The disability adjusted life years (DALYS) for diabetes increased from 0.71 per population in 1980 to 19.12 per population in 2010,which is nearly a 30-fold increase[15, 16]. As one of the most economically developed areas in China,Shanghai has a higher prevalence of diabetes,which is increasing rapidly and continuously. In 1980,the diabetes prevalence in Shanghai was 1.0%[9]. A recent study reported that the age-standardized prevalence of diabetes has increased from 9.7% in 2002 to 12.6% in 2009 in Shanghai adults aged 35-74[11]. Our study indicated that the prevalence of diabetes was 17.6% in adults aged 35 or older from Shanghai in 2013. The prevalence increased with age and was higher among men. Furthermore,there were many cases of prediabetes (16.5%). All these facts suggest a large and growing burden of diabetes in Shanghai.
Population aging,urbanization,decreasing physical activity,and a consequent obesity epidemic have contributed to the rapid increase in diabetes[17, 18]. As one of the most rapidly aging cities in China,Shanghai had 3.87 million adults who were at least 60 years old in 2013,accounting for more than a quarter of its residents[19]. Our survey showed that prevalence of diabetes and prediabetes was significantly higher among the elderly population in Shanghai. Urbanization is associated with changes in lifestyle that lead to physical inactivity and nutritional changes. These include consumption of processed foods,which are generally high in fat,sugar,and highly refined carbohydrates. In Shanghai,more than half of families consumed excess oil and salt,and their fruit and vegetable intakes were insufficient. Physical activity was low,while sedentary behavior was more common[20],which are associated with an increased risk of being overweight or obese. The rate of overweight among Shanghai residents aged 15-69 years has increased over time (27.3% in 2007,29.0% in 2010,and 32.1% in 2013),as did the obesity rate (7.1% in 2007,7.4% in 2010,and 9.4% in 2013)[20]. Additionally,the central obesity epidemic closely correlated with type 2 diabetes[21, 22]. In our study,both overweight and obesity were strongly associated with increasing prevalence of diabetes and prediabetes. The recent study also indicated that overconsumption of oil and salt was more common in rural areas[20]. With increasing wealth and development throughout the country,the prevalence of diabetes in rural areas has risen rapidly,and the urban-rural gaps in the distributions of overweight,obesity,physical inactivity,and hypertension have diminished[17]. Rural area may encounter greater risks than expected.
During the early stages of type 2 diabetes,many people remain undiagnosed because there are often few symptoms or symptoms that may not be recognized as being related to diabetes. Our study showed that among all patients with diabetes,68.1% of individuals were aware of their condition,and 63.5% reported receiving treatment for diabetes.However,only 35.1% of patients treated for diabetes had adequate glycemic control. A previous study indicated that diabetes awareness was 30%-40%,and the proportion of treatment was 25.8% in China[7, 8]. In the United States,diabetes affected 29.1 million people in 2012 (9.3% of the population),and about 21.0 million people have been diagnosed diabetes[23]. More than 50% of patients met the glycemic target (glycated hemoglobin <7.0%) in 2005-2010 in U.S[24, 25],which was higher than the rate in our study and reflected improvements in screening and diagnosis,while diabetes care was low in Shanghai.
Given the current increasing prevalence of diabetes and the inadequate glycemic control,diabetes prevention should be a priority for the government of Shanghai. First,as many complications can be detected in early stages by screening,early recognition is critical for prevention. People at high risk for diabetes should be screened,and people with diabetes should be supported by a well-educated health work force that provides regular blood tests,complication examinations,and self-management knowledge and skills education. More effective and efficient methods and criteria for diabetes screening should be further investigated. In addition,lifestyle interventions can prevent or delay diabetes progression[26, 27, 28] and thus reduce the large economic burden of diabetes,which would be cost-effective and cost-saving[29]. In 2014,the WHO issued new guidelines that suggest limiting sugar intake and recommended a daily free sugar intake of less than 10% of the total caloric intake in adults and children. A reduction to 5% of free sugar intake would be even more beneficial[30]. Lifestyle i ntervention policies limiting the intake of sugar,fat,and salt should be adopted by the government to fight against the unrelenting increased rates of type 2 diabetes. Furthermore,health professional training is also an essential issue and should be strengthened to improve the quality of healthcare for diabetes prevention and control[1].
Our study had a few limitations. First,this analysis was based on cross-sectional data,and we cannot determine the causes of underlying trends. Secondly,our study did not include residents less than 35 years old. Thirdly,we did not distinguish between type 1 and type 2 diabetes. However,our study had several strengths,including a representative sample of the adult population in Shanghai and use of oral glucose tolerance tests for all participants without a history of diabetes.
In conclusion,our study provides representative prevalence,related risk factors,awareness,and diabetes data for Shanghai residents. Diabetes and prediabetes are highly prevalent. However,1/3rd of diabetes cases are undiagnosed,and the rate of glycemic control is low. These findings indicate that diabetes is more than a health issue and requires concerted policy action across many sectors aimed at detection,prevention,and treatment of diabetes in Shanghai.
CONFLICT OF INTERESTNo potential conflicts of interest relevant to this article were reported.
AUTHOR CONTRIBUTIONSRY contributed to data acquisition,statistical analysis and draft and revision of the manuscript. YQHand XJY coordinated the study,data acquisition,statistical analysis and quality control. YQD and YHH contributed to data validation and quality control. LR and SY were the guarantors of this work and,as such,had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of thedata analysis. All authors approved the final version.
ACKNOWLEDGMENTSThe authors would like to thank all 1537 research staff from district CDC and community health service centers for their collection of data and blood samples. They also thanked all the study participants for their participation and contribution.
| 1. | International Diabetes Federation. Diabetes atlas Seventhedition,2015 [article online]. Available from http://www.diabetesatlas.org. [2016-2-8] |
| 2. | American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2012. Diabetes Care,2013; 36,1033-46. |
| 3. | Yang W,Zhao W,Xiao J,et al. MedicalCare and Payment for Diabetes in China: Enormous Threat and Great Opportunity. PLoS ONE,2012; 7,e39513. doi:10.1371. |
| 4. | National Diabetes Research Group. A mass survey of diabetes mellitus in a population of 300,000 in 14 provinces and municipalities in China. Chin J Intern Med,1981; 20,678-83. (In Chinese) |
| 5. | Pan XR,Yang WY,Li GW,et al. Prevalence of diabetes and its risk factors in China,1994. Diabetes Care,1997; 20,1664-9. |
| 6. | Gu D,Reynolds K,Duan X,et al. Prevalence of diabetes and impaired fasting glucose in theChinese adult population. Diabetologia,2003; 46,1190-8. |
| 7. | Yang W,Lu J,Weng J,et al. Prevalence ofdiabetes among men and women in China. N Engl J Med,2010; 362,1090-101. |
| 8. | Xu Y,Wang L,He J,et al. Prevalence and control of diabetes in Chinese adults. JAMA,2013; 310,948-59. |
| 9. | Shanghai diabetes research group. Diabetes mellitus survey in a population of 100,000 in Shanghai. Acta Academiae Medicinae Primae Shanghai,1980; 7,137-8. (In Chinese) |
| 10. | Li R,Lu W,Jia WP,et al. Cross-sectional investigation of prevalence of type 2 diabetes in Shanghai. Natl Med J China,2006; 86,1675-80. (In Chinese) |
| 11. | Li R,Lu W,Jiang QW,et al. Increasing prevalence of type 2 diabetes in Chinese adults in Shanghai. Diabetes Care,2012; 35,1028-30. |
| 12. | Department of disease prevention and control,the Ministry of health the people's Republic of China. Guidelines for the prevention and control of overweight and obesity in China adults. Beijing,People's Medical Publishing House,2006; 3. (In Chinese) |
| 13. | The World Health Organization Western Pacific Region. The Asia-Pacific perspective: redefining obesity and its treatment [article online]. Available from http://www.wpro.who.int/nutrition/documents/docs/Redefiningobesity.pdf?ua=1. [2016-2-8] |
| 14. | Alberti KG,Zimmet PZ. Definition,diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med,1998; 15,539-53. |
| 15. | Zhang YX,Wang M. The Burden of Disease and the Trend of Diabetes Mellitus in China,1980-2002. Chinese Health Economics,2009; 28,46-8. (In Chinese) |
| 16. | Li YC,Liu XT,Hu N,et al. Disease burden on diabetes in China2010. Chin J Epidemiol,2013; 34,33-6. (In Chinese) |
| 17. | Gong P,Liang S,Carlton EJ,et al. Urbanisation and health in China. Lancet,2012; 379,843-52. |
| 18. | Yang G,Kong L,Zhao W,et al. Emergence of chronic non- communicable diseases in China. Lancet,2008; 372,1697-705. |
| 19. | National Bureau of Statistics of China. Shanghai Statistical Yearbook 2014. Beijing,China Statistics Press,2014; 33. (In Chinese) |
| 20. | Shanghai Municipal Center for Disease Control and Prevention. Report of Shanghai Non-communicable and Chronic Disease Surveillance 2013. Shanghai Popular Science Press,2014; 4. (In Chinese) |
| 21. | Feng RN,Zhao C,Wang C,et al. BMI is strongly associated withhypertension,and waist circumference is strongly associated withtype 2 diabetes and dyslipidemia,in northern Chinese adults. J Epidemiol,2012; 22,317-23. |
| 22. | Ruan Y,Mo M,Joss-Moore L,et al. Increased waist circumference and prevalence of type 2 diabetes and hypertension in Chinese adults: two population-based cross-sectional surveys in Shanghai,China. BMJ Open,2013; 3,e003408. doi: 10.1136. |
| 23. | Centers for Disease Control and Prevention. National diabetes statistic report. 2014. [article online]. Available from http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web. pdf. [2016-2-8] |
| 24. | Ali MK,Bullard KM,Saaddine JB,et al. Achievement of goals in U.S. diabetes care,1999-2000. N Engl J Med,2013; 368,1613-24. |
| 25. | Selvin E,Parrinello CM,Sacks DB,et al. Trends in prevalence and control of diabetes in the United States,1988-1994 and 1999-2010. Ann Intern Med,2014; 160,517-25. |
| 26. | Pan XR,Li GW,Hu YH,et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care,1997; 20,537-44. |
| 27. | Tuomilehto J,Lindström J,Eriksson JG,et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med,2001; 344,1343-50. |
| 28. | Knowler WC,Barrett-Connor E,Fowler SE,et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med,2002; 346,393-403. |
| 29. | Diabetes Prevention Program Research Group. The 10-year cost-effectiveness of lifestyle intervention or metformin for diabetes prevention: an intent-to-treat analysis of the DPP/DPPOS. Diabetes Care,2012; 35,723-30. |
| 30. | World Health Organization. Sugars intake for adults and children Guideline. http://www.who.int/nutrition/ publications/guidelines/sugars_intake/en/. [2016-4-10] |