 2023, Vol. 44
2023, Vol. 44文章信息
- 魏港吉, 陈晓芳, 陈小芳, 伍霞, 常晓宇, 裴培, 吴先萍.
- Wei Gangji, Chen Xiaofang, Chen Xiaofang, Wu Xia, Chang Xiaoyu, Pei Pei, Wu Xianping
- 吸烟对四川省30岁及以上居民慢性阻塞性肺疾病发病风险影响的前瞻性研究
- Relationship between smoking and the risk of morbidity of chronic obstructive pulmonary diseases among residents aged 30 years and above in Sichuan Province: a prospective study
- 中华流行病学杂志, 2023, 44(5): 778-785
- Chinese Journal of Epidemiology, 2023, 44(5): 778-785
- http://dx.doi.org/10.3760/cma.j.cn112338-20221123-00994
-
文章历史
收稿日期: 2022-11-23




2. 四川省彭州市疾病预防控制中心, 彭州 611930;
3. 四川省疾病预防控制中心, 成都 610041;
4. 北京大学公众健康与重大疫情防控战略研究中心, 北京 100191
2. Pengzhou Center for Disease Control and Prevention, Sichuan Province, Pengzhou 611930, China;
3. Sichuan Provincial Center for Disease Control and Prevention, Chengdu 610041, China;
4. Peking University Center for Public Health and Epidemic Preparedness & Response, Beijing 100191, China
慢性阻塞性肺疾病(COPD)作为一种常见的可以预防和治疗的慢性、进行性加重的呼吸系统疾病,是目前全球第三大死因,全球≥40岁人群中COPD患病率达到9%~10%[1]。由于其患病人数众多,病程长,造成的社会及经济负担重,已成为重要的公共卫生问题[2]。我国西南地区 > 40岁居民COPD患病率较高,其中四川省COPD患病率约为24%,远高于其他地区[3]。研究发现,吸烟是造成慢性支气管炎症和气道阻塞发生的主要原因,我国≥15岁吸烟人数高达3.16亿[4-5]。因此,明确四川省≥30岁居民吸烟与COPD发病之间的关系极其重要。本研究旨在利用中国慢性病前瞻性研究(CKB)四川省调查的基线数据、重复调查数据和随访数据,探讨四川省≥30岁居民吸烟对COPD发病风险的影响,为有针对性地在本地区开展预防干预提供科学依据。
对象与方法1. 调查对象:来源于CKB项目2004-2008年开展的基线调查中全国10个项目点之一的四川省彭州市,并将55 686名(30~79岁)具有完整基线调查数据者列为调查对象,其中剔除基线调查有肺结核、肺气肿、支气管炎、哮喘和肺癌病史或符合COPD全球创议标准(1级及以上)[剔除1秒用力呼气容积(FEV1)≥80%的预计值,FEV1/FVC(用力肺活量) < 70%]9 146名,项目详细介绍见文献[6-8]。
2. 调查内容及方法:通过调查员面对面问卷调查获得一般人口学信息(年龄、性别、文化程度、职业、婚姻状况、家庭年收入)、当前做饭频率、当前有无排烟装置、吸烟状况、日均吸烟量、当前吸烟类型、开始吸烟类型、开始吸烟年龄、烟吸入部位。通过体格检查获得身高、体重、BMI等指标,通过个体每天4类体力活动水平相加得到日均总体力活动水平[用代谢当量(MET)-h/d表示][9-10]。根据被动吸烟问卷得到所有调查对象的被动吸烟暴露频率(每周在家/工作场合等地被动吸烟每次持续5 min以上的天数)。根据吸烟问卷中的当前吸烟状态、既往吸烟习惯、累计吸烟量是否超过100支、调查当天是否吸过烟和戒烟时间5个问题将吸烟状况划分为从不吸、偶尔吸、戒烟和当前吸,并根据自报吸烟种类及对应量计算个体的日均吸烟量,日均吸烟量(g)=(过滤嘴香烟量+无过滤嘴香烟量+2×雪茄量)+5/3×(手卷烟/旱烟量+烟斗/水烟量)[11]。在完成基线调查后,使用与基线调查类似的程序,于2013-2014年随机抽取5%~6%的基线调查数据者进行重复调查,根据纳入排除标准,纳入2 339名重复调查数据者以校正基线调查的结果。
3. 结局评价:随访从调查对象完成基线调查之日开始算起,直到出现发病、死亡、失访或截至2017年12月31日。发病情况通过多种途径获取,主要通过当地死亡和常规疾病监测系统、全民医疗保险数据库,并结合利用CKB项目的主动定向监测进行补充完善。发病采用国际疾病分类第十版,终点为COPD(J41~J44)发病。
4. 统计学分析:数据采用SAS 9.4软件进行整理和分析,计数资料采用例数(%)进行描述,组间比较采用χ²检验;利用Cox比例风险回归模型分析吸烟和COPD的关系,等级变量设定为哑变量计算各组HR值和95%CI。采用Rosner回归校准法,校正回归稀释偏倚。双侧检验,检验水准α=0.05。
结果1. 一般情况:共纳入46 540名30~79岁研究人群进行分析,男性17 306名(37.19%),女性29 234名(62.81%),年龄为(50.38±10.17)岁。文化程度以小学及以下为主(62.69%);家庭年收入以 < 20 000元为主(90.51%);职业以农林牧渔劳动者为主(87.91%);已婚者居多(91.91%)。46 540名调查对象中,男性当前吸烟占比(67.31%)高于女性(8.67%),男性戒烟的占比(10.63%)高于女性(3.09%)。男性吸烟者日均吸烟量整体上高于女性,男、女性当前吸烟类型均以香烟为主。见表 1。

2. 不同特征人群COPD发病情况:调查对象累计随访509 254.18人年(平均随访10.94年),共3 101名新发COPD,累积发病率为6.66%。从不同特征人群来看,女性、其他职业、分居/离异/丧偶和从未结婚者COPD发病率较高;COPD发病率随着年龄的增加、家庭年收入的减少、文化程度的降低而升高。从不同吸烟状况来看,戒烟者COPD发病率最高,其次为当前吸烟者。见表 2。

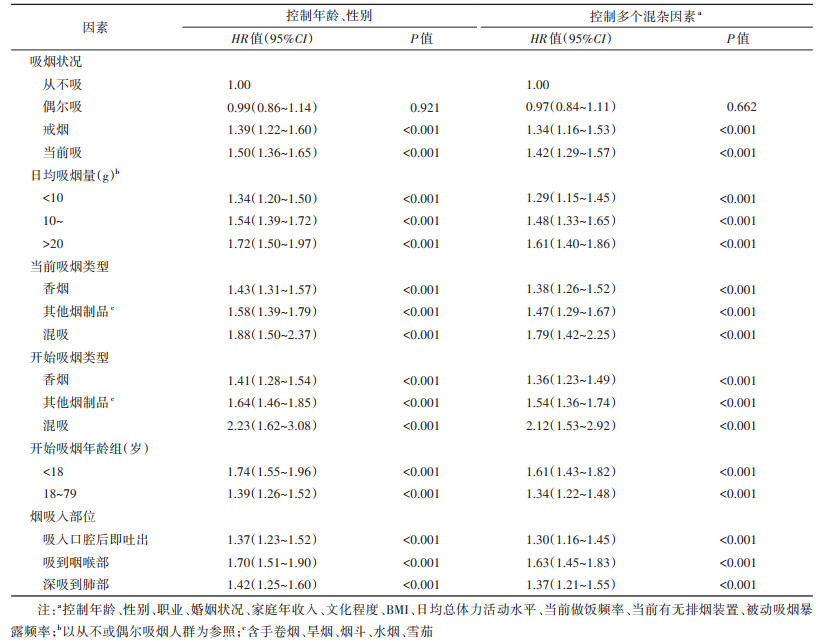
3. COPD发病风险的多因素分析:控制年龄、性别、职业、婚姻状况、家庭年收入、文化程度、BMI、日均总体力活动水平、当前做饭频率、当前有无排烟装置、被动吸烟暴露频率等因素,利用Cox比例风险回归模型分析吸烟对COPD发病风险的影响。经时协变量法检验,吸烟相关变量满足比例风险假定。分析结果显示,与从不吸烟人群相比,当前吸烟、戒烟增加COPD的发病风险,HR值分别为1.42(95%CI:1.29~1.57)和1.34(95%CI:1.16~1.53)。与从不或偶尔吸烟人群相比,日均吸烟量越大,COPD发病风险越高,日均吸烟量 > 20 g的COPD发病风险最高,HR值为1.61(95%CI:1.40~1.86);当前吸烟类型为混吸、开始吸烟类型为混吸增加COPD的发病风险,HR值分别为1.79(95%CI:1.42~2.25)和2.12(95%CI:1.53~2.92),且其他烟制品COPD发病风险高于香烟;开始吸烟年龄 < 18、≥18岁增加COPD的发病风险,HR值分别为1.61(95%CI:1.43~1.82)和1.34(95%CI:1.22~1.48);吸烟时吸入口腔后即吐出、吸到咽喉部和深吸到肺部增加COPD的发病风险,HR值分别为1.30 (95%CI:1.16~1.45)、1.63(95%CI:1.45~1.83)和1.37(95%CI:1.21~1.55)。见表 3。
4. 男、女性人群吸烟对COPD发病风险的多因素分析:日均吸烟量、开始吸烟年龄和烟吸入部位对COPD发病均有影响,性别差异尤为突出,在控制年龄、职业、婚姻状况、家庭年收入、文化程度、BMI、日均总体力活动水平、当前做饭频率、当前有无排烟装置、被动吸烟暴露频率因素,校正回归稀释偏倚后,与从不吸烟人群相比,男性吸烟增加COPD的发病风险,当前吸烟的COPD发病风险最高,aHR值为1.56(95%CI:1.41~1.73)。与从不或偶尔吸烟人群相比,男性日均吸烟量越大,COPD发病风险越高;男性当前吸烟类型为混吸、开始吸烟类型为混吸COPD的发病风险最高,aHR值分别为2.09(95%CI:1.88~2.32)和2.42(95%CI:2.07~2.82),且其他烟制品COPD发病风险高于香烟;男性开始吸烟年龄 < 18、≥18岁增加COPD的发病风险,aHR值分别为1.69(95%CI:1.56~1.83)和1.34(95%CI:1.25~1.43);男性吸烟时吸入口腔后即吐出、吸到咽喉部或深吸到肺部增加COPD的发病风险,aHR值分别为1.39(95%CI:1.31~1.48)、1.89(95%CI:1.76~2.02)和1.31(95%CI:1.22~1.42)。与从不吸烟人群相比,女性当前吸烟、戒烟增加COPD的发病风险,aHR值分别为1.58(95%CI:1.50~1.67)和1.41(95%CI:1.30~1.53),偶尔吸烟降低COPD的发病风险,aHR值为0.88(95%CI:0.82~0.95)。与从不或偶尔吸烟人群相比,女性日均吸烟量越大,COPD发病风险越高;女性当前吸烟类型为混吸降低COPD的发病风险,aHR值为0.60(95%CI:0.38~0.94),开始吸烟类型为混吸者COPD发病风险最高,aHR值为2.04(95%CI:1.41~2.97);女性开始吸烟年龄 < 18、≥18岁增加COPD的发病风险,aHR值分别为2.00(95%CI:1.87~2.14)和1.55(95%CI:1.48~1.62);女性吸烟时吸入口腔后即吐出、吸到咽喉部或深吸到肺部增加COPD的发病风险,aHR值分别为1.41(95%CI:1.34~1.49)、2.13(95%CI:2.01~2.26)和1.94(95%CI:1.84~2.05)。见表 4。

COPD的发病率随着年龄增长而升高,且文化程度和经济收入越低,COPD的发病率越高,与既往研究的结论一致[12-15]。COPD发病风险在不同性别之间是否存在差异尚有争议,有研究认为男性COPD发病率高于女性[16-17],也有研究显示,女性COPD发病风险是男性的1.78倍[18]。在本研究中,女性COPD发病率高于男性,原因可能是四川省女性烟草暴露的概率更大[11],且女性呼吸道比男性更加敏感[19]。
本研究在控制年龄、性别、职业、婚姻状况、家庭年收入、文化程度、BMI、日均总体力活动水平、当前做饭频率、当前有无排烟装置、被动吸烟暴露频率混杂因素后,当前吸烟人群COPD的发病风险最高,与已有研究结果一致[20-23]。
吸烟量越大、吸烟年限越长、开始吸烟年龄越小,COPD的发病风险越高[24]。本研究中,开始吸烟年龄 < 18岁人群COPD的发病风险明显高于≥18岁人群,与既往队列研究结果一致[25-27]。Wang等[28]纳入17项横断面研究、3项队列研究、4项病例对照研究,针对中国人群吸烟与COPD的关系进行Meta分析,其结果显示,吸烟量为1~、200~、> 400支/年者COPD的患病风险分别是从不吸烟者的2.49、2.91、4.07倍。本研究与其结果相似,随着日均吸烟量的增加,COPD的发病风险逐渐增加。除此之外,女性人群中,日均吸烟量 < 10、10~、> 20 g的COPD发病风险均高于男性,也证明女性对烟草烟雾的危害更敏感。
本研究发现,吸烟类型为其他烟制品的COPD发病风险高于香烟,与已有研究结果一致[29-30],可能一方面是因为香烟的焦油、尼古丁等有害物质含量相对较低,部分香烟采取过滤嘴设计;另一方面是部分吸烟者虽然在手卷烟、水烟等其他烟制品中使用更少的烟草含量,但吸烟频率高反而增加COPD的发病风险[31]。另外,本研究结果显示,当前吸烟类型为混吸者COPD的发病风险最高,而且开始吸烟类型为混吸者COPD发病风险高于当前吸烟类型为混吸者。提示COPD发病风险可能更易受混吸多种烟制品和混吸年限影响,仍需进行更深入的调查研究。
已有研究显示,吸烟越深入,可替宁、癸烷等有害成分吸入浓度越高,COPD发病危险越大[32-34]。张啸飞等[35]的研究结果显示,吸烟深度对COPD患病有影响。在本研究中,与从不或偶尔吸烟人群相比,吸烟时吸入口腔后即吐出增加COPD的发病风险远低于吸到咽喉部和深吸到肺部,且吸到咽喉部增加COPD的发病风险最高,与既往研究结果存在差异。可能是调查对象自报烟吸入部位,存在一定划分问题,其具体原因需进一步探讨。除此之外,女性人群吸烟时吸入口腔后即吐出、吸到咽喉部和深吸到肺部COPD发病风险均高于男性,也证明女性呼吸系统对烟草烟雾更敏感。此外,利用COPD相关危险因素的单一测量值进行分析会导致危险因素与结局之间的关联因缺乏统计学意义而被忽略[36]。本研究分析结合重复调查数据,校正回归稀释偏倚[37],研究结果与真实情况相近。
本研究存在局限性。吸烟信息源自调查对象自报,可能存在信息偏倚。尽管如此,本研究发现吸烟会增加COPD的发病风险,这种影响与吸烟量、吸烟类型、开始吸烟年龄和烟吸入部位等均存在一定的关系。提示控烟仍是COPD防控的重中之重,应综合考虑吸烟的具体行为特征,以制定针对性策略。
利益冲突 所有作者声明无利益冲突
作者贡献声明 魏港吉:分析/解释数据、论文撰写、统计分析;陈晓芳:分析/解释数据、论文修改;陈小芳、伍霞:采集数据、经费支持;常晓宇、裴培、吴先萍:实施研究、技术支持
志谢 感谢中国慢性病前瞻性管理委员会、项目办公室和四川省项目地区办公室的工作人员
| [1] |
Christenson SA, Smith BM, Bafadhel M, et al. Chronic obstructive pulmonary disease[J]. Lancet, 2022, 399(10342): 2227-2242. DOI:10.1016/S0140-6736(22)00470-6 |
| [2] |
李薇, 杨汀, 王辰. 中国慢性阻塞性肺疾病防治现状及进展[J]. 中国研究型医院, 2020, 7(5): 1-5. Li W, Yang T, Wang C. Current status and progress of prevention and treatment of chronic obstructive pulmonary disease in China[J]. J Chin Res Hosp, 2020, 7(5): 1-5. DOI:10.19450/j.cnki.jcrh.2020.05.001 |
| [3] |
董婷, 胥馨尹, 邓颖, 等. 四川省≥40岁常住居民慢性阻塞性肺疾病患病情况及其影响因素分析[J]. 中国公共卫生, 2021, 37(12): 1762-1765. Dong T, Xu XY, Deng Y, et al. Prevalence and influencing factors of chronic obstructive pulmonary disease among middle-aged and elderly residents in Sichuan Province, 2015[J]. Chin J Public Health, 2021, 37(12): 1762-1765. DOI:10.11847/zgggws1130083 |
| [4] |
中华医学会呼吸病学分会慢性阻塞性肺疾病学组, 中国医师协会呼吸医师分会慢性阻塞性肺疾病工作委员会. 慢性阻塞性肺疾病诊治指南(2021年修订版)[J]. 中华结核和呼吸杂志, 2021, 44(3): 170-205. Chronic Obstructive Pulmonary Disease Group, Respiratory Branch, Chinese Medical Association, Chronic Obstructive Pulmonary Disease Working Committee of Respiratory Doctor Branch of Chinese Medical Doctor Association. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021)[J]. Chin J Tuberc Respir Dis, 2021, 44(3): 170-205. DOI:10.3760/cma.j.cn112147-20210109-00031 |
| [5] |
刘朝, 肖丹, 王辰. 戒烟是慢性阻塞性肺疾病防治的最有效措施[J]. 中华结核和呼吸杂志, 2017, 40(12): 894-897. Liu C, Xiao D, Wang C. Tobacco cessation is the most effective intervention for the prevention and treatment of obstructive pulmonary disease[J]. Chin J Tuberc Respir Dis, 2017, 40(12): 894-897. DOI:10.3760/cma.j.issn.1001-0939.2017.12.005 |
| [6] |
Chen ZM, Lee L, Chen JS, et al. Cohort profile: the Kadoorie Study of Chronic Disease in China (KSCDC)[J]. Int J Epidemiol, 2005, 34(6): 1243-1249. DOI:10.1093/ije/dyi174 |
| [7] |
Chen ZM, Chen JS, Collins R, et al. China Kadoorie Biobank of 0.5 million people: survey methods, baseline characteristics and long-term follow-up[J]. Int J Epidemiol, 2011, 40(6): 1652-1666. DOI:10.1093/ije/dyr120 |
| [8] |
李立明, 吕筠, 郭彧, 等. 中国慢性病前瞻性研究: 研究方法和调查对象的基线特征[J]. 中华流行病学杂志, 2012, 33(3): 249-255. Li LM, Lv J, Guo Y, et al. The China Kadoorie Biobank: related methodology and baseline characteristics of the participants[J]. Chin J Epidemiol, 2012, 33(3): 249-255. DOI:10.3760/cma.j.issn.0254-6450.2012.03.001 |
| [9] |
樊萌语, 吕筠, 郭彧, 等. 中国慢性病前瞻性研究: 10个项目地区成人体力活动和休闲静坐时间特征差异的分析[J]. 中华流行病学杂志, 2015, 36(8): 779-785. Fan MY, Lyu J, Guo Y, et al. Regional differences on patterns of physical activity and leisure sedentary time: findings from the China Kadoorie Biobank study, including a million people from 10 regions[J]. Chin J Epidemiol, 2015, 36(8): 779-785. DOI:10.3760/cma.j.issn.0254-6450.2015.08.002 |
| [10] |
Du HD, Bennett D, Li LM, et al. Physical activity and sedentary leisure time and their associations with BMI, waist circumference, and percentage body fat in 0.5 million adults: the China Kadoorie Biobank study[J]. Am J Clin Nutr, 2013, 97(3): 487-496. DOI:10.3945/ajcn.112.046854 |
| [11] |
王昕, 吕筠, 郭彧, 等. 中国慢性病前瞻性研究: 10个项目地区成年人群吸烟行为特征差异分析[J]. 中华流行病学杂志, 2015, 36(11): 1200-1204. Wang X, Lyu J, Guo Y, et al. Regional differences in adults' smoking pattern: findings from China Kadoorie Biobank study in 10 areas in China[J]. Chin J Epidemiol, 2015, 36(11): 1200-1204. DOI:10.3760/cma.j.issn.0254-6450.2015.11.004 |
| [12] |
秦国双, 温昊于, 宇传华. 中国COPD的患病发病及YLD现状及趋势[J]. 公共卫生与预防医学, 2019, 30(2): 4-8. Qin GS, Wen HY, Yu CH. The prevalence incidence and YLD status and trend of COPD in China[J]. J Public Health Prev Med, 2019, 30(2): 4-8. DOI:10.3969/j.issn.1006-2483.2019.02.002 |
| [13] |
Leem AY, Park B, Kim YS, et al. Incidence and risk of chronic obstructive pulmonary disease in a Korean community-based cohort[J]. Int J Chron Obstruct Pulmon Dis, 2018, 13: 509-517. DOI:10.2147/COPD.S148618 |
| [14] |
Cho WK, Lee CG, Kim LK. COPD as a disease of immunosenescence[J]. Yonsei Med J, 2019, 60(5): 407-413. DOI:10.3349/ymj.2019.60.5.407 |
| [15] |
郑健, 赵燕霞, 王英田, 等. 北京市顺义区慢性阻塞性肺疾病患病率和相关危险因素调查[J]. 医学信息, 2021, 34(2): 108-112. Zheng J, Zhao YX, Wang YT, et al. Investigation on the prevalence and related risk factors of chronic obstructive pulmonary disease in Shunyi District, Beijing[J]. J Med Inf, 2021, 34(2): 108-112. DOI:10.3969/j.issn.1006-1959.2021.02.029 |
| [16] |
Fang LW, Gao P, Bao HL, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study[J]. Lancet Respir Med, 2018, 6(6): 421-430. DOI:10.1016/S2213-2600(18)30103-6 |
| [17] |
Luoto JA, Elmståhl S, Wollmer P, et al. Incidence of airflow limitation in subjects 65-100 years of age[J]. Eur Respir J, 2016, 47(2): 461-472. DOI:10.1183/13993003.00635-2015 |
| [18] |
Chang JT, Meza R, Levy DT, et al. Prediction of COPD risk accounting for time-varying smoking exposures[J]. PLoS One, 2021, 16(3): e0248535. DOI:10.1371/journal.pone.0248535 |
| [19] |
Silverman EK, Weiss ST, Drazen JM, et al. Gender-related differences in severe, early-onset chronic obstructive pulmonary disease[J]. Am J Respir Crit Care Med, 2000, 162(6): 2152-2158. DOI:10.1164/ajrccm.162.6.2003112 |
| [20] |
顾建华, 马晓天, 李吉庆, 等. 健康管理队列慢性阻塞性肺疾病风险预测模型[J]. 山东大学学报: 医学版, 2017, 55(12): 62-65, 70. Gu JH, Ma XT, Li JQ, et al. Risk prediction model of chronic obstructive pulmonary disease in health management cohort[J]. J Shandong Univ: Health Sci, 2017, 55(12): 62-65, 70. DOI:10.6040/j.issn.1671-7554.0.2017.447 |
| [21] |
赵璨, 孙培培, 张二明, 等. 北京十家社区40岁及以上居民吸烟、二手烟暴露与慢性阻塞性肺疾病的关系[J]. 中华临床医师杂志: 电子版, 2021, 15(6): 450-458. Zhao C, Sun PP, Zhang EM, et al. Association of smoking and second-hand smoking with chronic obstructive pulmonary disease among residents aged 40 years or above in 10 communities of Beijing City[J]. Chin J Clin: Electron Ed, 2021, 15(6): 450-458. DOI:10.3877/cma.j.issn.1674-0785.2021.06.009 |
| [22] |
Lytras T, Kogevinas M, Kromhout H, et al. Occupational exposures and 20-year incidence of COPD: the European Community Respiratory Health Survey[J]. Thorax, 2018, 73(11): 1008-1015. DOI:10.1136/thoraxjnl-2017-211158 |
| [23] |
Traulsen LK, Baelum J, Halling A, et al. Risk factors for incident asthma and COPD in a cohort of young adults[J]. Clin Respir J, 2018, 12(3): 1021-1029. DOI:10.1111/crj.12622 |
| [24] |
《中国吸烟危害健康报告2020》编写组. 《中国吸烟危害健康报告2020》概要[J]. 中国循环杂志, 2021, 36(10): 937-952. The Writing Committee of 2020 Report on Health Hazards of Smoking in China. 2020 Report on Health Hazards of Smoking in China: an updated summary[J]. Chin Circ J, 2021, 36(10): 937-952. DOI:10.3969/j.issn.1000-3614.2021.10.001 |
| [25] |
潘东霞, 钱一建, 王春梅, 等. 吸烟与室内空气污染的交互作用对慢性阻塞性肺部疾病影响的分析[J]. 中华流行病学杂志, 2016, 37(11): 1444-1449. Pan DX, Qian YJ, Wang CM, et al. Interaction between smoking and indoor air pollution on chronic obstructive pulmonary diseases[J]. Chin J Epidemiol, 2016, 37(11): 1444-1449. DOI:10.3760/cma.j.issn.0254-6450.2016.11.002 |
| [26] |
Amaral AFS, Strachan DP, Burney PGJ, et al. Female smokers are at greater risk of airflow obstruction than male smokers. UK biobank[J]. Am J Respir Crit Care Med, 2017, 195(9): 1226-1235. DOI:10.1164/rccm.201608-1545OC |
| [27] |
刘鑫. 2014年吉林省国家监测点居民慢性阻塞性肺疾病流行状况及影响因素分析[D]. 长春: 吉林大学, 2018. Liu X. Prevalence of chronic obstructive pulmonary disease and its influencing factors at national surveillance site of Jilin Province in 2014[D]. Changchun: Jilin University, 2018. |
| [28] |
Wang BY, Xiao D, Wang C. Smoking and chronic obstructive pulmonary disease in Chinese population: a meta-analysis[J]. Clin Respir J, 2015, 9(2): 165-175. DOI:10.1111/crj.12118 |
| [29] |
Kocyigit A, Selek S, Celik H, et al. Mononuclear leukocyte DNA damage and oxidative stress: the association with smoking of hand-rolled and filter-cigarettes[J]. Mutat Res, 2011, 721(2): 136-141. DOI:10.1016/j.mrgentox.2011.01.013 |
| [30] |
Pednekar MS, Gupta PC, Yeole BB, et al. Association of tobacco habits, including bidi smoking, with overall and site-specific cancer incidence: results from the Mumbai cohort study[J]. Cancer Causes Control, 2011, 22(6): 859-868. DOI:10.1007/s10552-011-9756-1 |
| [31] |
Zumbado M, Luzardo OP, Rodríguez-Hernández Á, et al. Differential exposure to 33 toxic elements through cigarette smoking, based on the type of tobacco and rolling paper used[J]. Environ Res, 2019, 169: 368-376. DOI:10.1016/j.envres.2018.11.021 |
| [32] |
Chen X, Wang FY, Lin LQ, et al. Association of smoking with metabolic volatile organic compounds in exhaled breath[J]. Int J Mol Sci, 2017, 18(11): 2235. DOI:10.3390/ijms18112235 |
| [33] |
Lidón-Moyano C, Fu M, Pérez-Ortuño R, et al. Impact of the spanish smoking legislation among smokers: a longitudinal study with biomarkers in Barcelona (Spain)[J]. Addict Behav, 2018, 87: 101-108. DOI:10.1016/j.addbeh.2018.06.023 |
| [34] |
Thun MJ, Carter BD, Feskanich D, et al. 50-year trends in smoking-related mortality in the United States[J]. N Engl J Med, 2013, 368(4): 351-364. DOI:10.1056/NEJMsa1211127 |
| [35] |
张啸飞, 程显声, 李景周, 等. 吸烟者慢性阻塞性肺疾病外环境因素的病例对照研究[J]. 中国慢性病预防与控制, 2000, 8(1): 20-22. Zhang XF, Cheng XS, Li JZ, et al. Case-control study on the effects of environmental factors on COPD in smokers[J]. Chin J Prev Control Chronic Dis, 2000, 8(1): 20-22. DOI:10.3969/j.issn.1004-6194.2000.01.009 |
| [36] |
白银晓, 王子悦, 柴昊, 等. 线性回归中回归稀释偏倚校正的模拟研究[J]. 中国卫生统计, 2021, 38(4): 566-571. Bai YX, Wang ZY, Chai H, et al. Simulation study on regression dilution bias correction in linear regression[J]. Chi J Health Stat, 2021, 38(4): 566-571. DOI:10.3969/j.issn.1002-3674.2021.04.023 |
| [37] |
Du HD, Li LM, Bennett D, et al. Fresh fruit consumption and major cardiovascular disease in China[J]. N Engl J Med, 2016, 374(14): 1332-1343. DOI:10.1056/NEJMoa1501451 |