 2023, Vol. 44
2023, Vol. 44文章信息
- 王志如, 李惟怡, 姜红如, 贾小芳, 黄绯绯, 胡霄, 王惠君, 张兵, 王志宏.
- Wang Zhiru, Li Weiyi, Jiang Hongru, Jia Xiaofang, Huang Feifei, Hu Xiao, Wang Huijun, Zhang Bing, Wang Zhihong
- 中国四省7~17岁儿童青少年心血管代谢性危险因素的流行特征
- Epidemiological characteristics of cardio-metabolic risk factors among children and adolescents aged 7-17 years in 4 provinces of China
- 中华流行病学杂志, 2023, 44(4): 592-597
- Chinese Journal of Epidemiology, 2023, 44(4): 592-597
- http://dx.doi.org/10.3760/cma.j.cn112338-20220927-00814
-
文章历史
收稿日期: 2022-09-27




《中国心血管健康与疾病报告2021概要》显示,我国心血管病(CVD)患病率呈持续上升状态,2019年我国农村、城市居民死因中,CVD所占的比例分别为46.74%和44.26%,在城乡居民死亡构成比中均占首位[1]。主要的心血管代谢性危险因素包括高腰围、中心性肥胖、TG升高、TC升高、LDL-C升高、HDL-C降低、血压升高、血糖升高等,可以通过一级预防措施有效控制[2-3]。研究表明,儿童时期心血管危险因素与成年人心血管危险因素和疾病风险增加有关联[4-5],从儿童时期监测并控制心血管危险因素,可以降低成年人CVD的风险,有效减轻我国CVD的负担[6]。本研究拟利用“神经系统疾病专病社区队列研究”(Community-based Cohort Study on Nervous System Disease,CCSNSD)2018年调查数据,分析7~17岁儿童青少年心血管代谢性危险因素的流行特征,探讨不同人口经济因素之间危险因素的差异。
资料与方法1. 资料来源:利用CCSNSD数据,于2018年在河北省、浙江省、陕西省和湖南省(四省)开展基线调查。采用分层多阶段整群随机抽样的方法,在四省分别抽取2个城市点及2个县城点,每个城市点选择1个城市居委会和1个郊区村,每个县城点选择1个县城居委会和1个村,共在32个调查点选择研究对象。选取7~17岁儿童青少年中具有完整血样检测者1 827名,剔除人口经济特征数据缺失者40名,体检结果缺失者35名,剔除数据异常者5名,最终纳入1 747名。调查内容包括问卷调查(包括人口经济状况、生活方式、食物频率、健康风险因素筛查等)、体格测量和生物样采集。该课题通过中国CDC营养与健康所伦理委员会审查(批准文号:2017020),调查对象均签署了知情同意书。
2. 心血管代谢性危险因素的评价:
(1)体检:现场调查员进行统一培训。身高测量采用SECA206型卷筒式量高尺,体重测量采用SECA882电子体重秤,腰围、臀围测量采用无弹性软尺,血压测量采用标准汞柱式血压计。体检现场抽取研究对象空腹静脉血并进行生化检测,检测指标包括血脂、血糖和尿酸,由第三方检测公司负责检测。
(2)心血管危险因素判定标准:①高腰围:依据《7岁~18岁儿童青少年高腰围筛查界值》(WS/T 611-2018),以不同性别儿童青少年年龄别腰围P90作为界值点,判断儿童高腰围[7];②中心性肥胖:依据《学龄儿童青少年超重与肥胖筛查》(WS/T 586-2018)性别年龄别BMI超重与肥胖的界值分为非超重肥胖、超重、肥胖[8],在肥胖儿童中利用高腰围判断中心性肥胖;③血脂异常:依据我国《儿童青少年血脂异常防治专家共识》推荐的诊断标准予以判定,即TG≥1.70 mmol/L为TG升高,HDL-C≤1.04 mmol/L为HDL-C降低,TC≥5.18 mmol/L为TC升高,LDL-C≥3.37 mmol/L为LDL-C升高[9];④血压升高:依据《7岁~18岁儿童青少年血压偏高筛查界值》(WS/T 610-2018),SBP和(或)DBP≥同性别、同年龄、同身高百分位人群P95血压为血压偏高[10];⑤血糖升高:依据国际糖尿病联盟(IDF)发布的针对儿童青少年的诊断标准,FPG≥5.6 mmol/L为血糖升高[11];⑥将中心性肥胖、血脂异常、血压升高、血糖升高中具有≥2项者判定为危险因素聚集。
(3)人口经济学因素:经体检获得身高、体重信息;经培训考核合格的现场调查员入户通过问卷调查获得相关数据信息,包括年龄、性别、城乡、地区(北方:陕西省、河北省;南方:湖南省、浙江省)、家庭人均月收入(低:< 1 000元;中:1 000~元;高:≥4 000元)。
3.统计学分析:应用SAS 9.3软件进行数据清理和分析。7~17岁儿童青少年不同人口经济特征的各心血管代谢性危险因素检出率及聚集性的单因素分析采用χ2检验;不同家庭人均月收入、不同BMI水平的儿童青少年各心血管代谢性危险因素及危险因素聚集的趋势分析采用Cochran-Armitage趋势检验。应用多因素logistic回归分析人口经济学因素与各心血管代谢性危险因素及聚集性的关系。双侧检验,检验水准α=0.05。
结果1. 基本情况:共纳入1 747名7~17岁儿童青少年,其中男生951名(54.44%)、女生796名(45.56%);7~岁占42.93%,13~17岁占57.07%;北方和南方地区分别占51.63%、48.37%;城市和农村分别占36.23%、63.77%;家庭人均月收入低、中、高分别占15.51%、62.68%、21.81%;非超重肥胖、超重、肥胖组分别占76.24%、13.51%、10.25%。见表 1。

2. 不同人群心血管危险因素和聚集性检出率:心血管危险因素检出率由高到低依次为高腰围(29.08%)、HDL-C降低(15.28%)、血压升高(13.17%)、TG升高(13.05%)、血糖升高(11.79%)、中心性肥胖(7.33%)、TC升高(6.53%)、LDL-C升高(5.15%)。儿童青少年中危险因素聚集检出率为18.37%。男生TG升高、血糖升高和危险因素聚集检出率高于女生;13~17岁年龄组的高腰围、HDL-C降低检出率高于7~岁年龄组,中心性肥胖检出率低于7~岁年龄组;南方地区儿童青少年TC、LDL-C、TG升高和HDL-C降低的检出率均高于北方,但高腰围和中心性肥胖检出率低于北方(均P < 0.05);随家庭人均月收入提高,TC、LDL-C、TG升高和危险因素聚集的检出率逐渐增加(趋势P < 0.05);随BMI增加,高腰围、TG升高、HDL-C降低、血糖升高、血压升高、危险因素聚集的检出率均呈增长趋势(趋势P < 0.05)。见表 1。
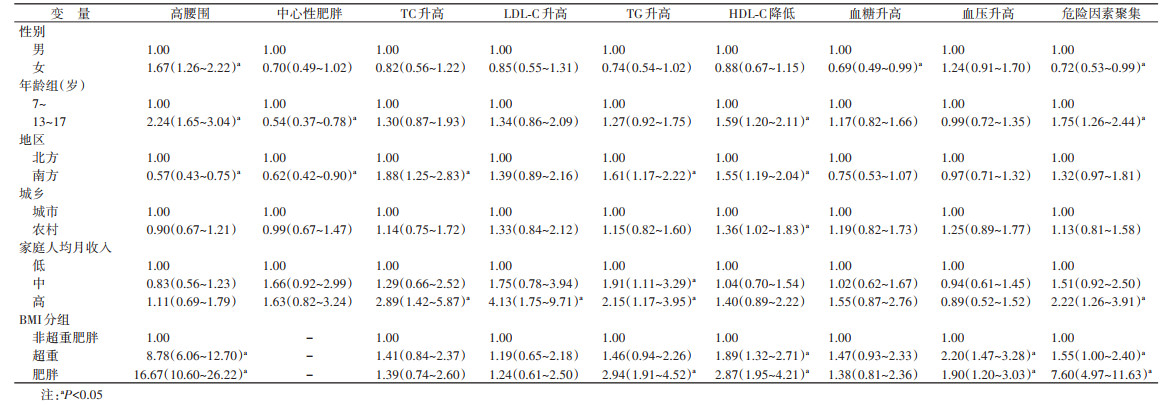
3. 人口经济特征与代谢性危险因素和聚集性的多因素分析:多因素logisitic回归分析结果显示,我国四省7~17岁儿童青少年中,女性高腰围发生的风险高于男性(OR=1.67,95%CI:1.26~2.22),血糖升高和危险因素聚集的风险低于男性(OR=0.69,95%CI:0.49~0.99;OR=0.72,95%CI:0.53~0.99);13~17岁年龄组高腰围、HDL-C降低、危险因素聚集的风险高于7~岁年龄组(OR=2.24,95%CI:1.65~3.04;OR=1.59,95%CI:1.20~2.11;OR=1.75,95%CI:1.26~2.44),中心性肥胖的风险低于7~岁年龄组(OR=0.54,95%CI:0.37~0.78);南方地区儿童青少年TC升高、TG升高、HDL-C降低的风险高于北方(OR=1.88,95%CI:1.25~2.83;OR=1.61,95%CI:1.17~2.22;OR=1.55,95%CI:1.19~2.04),但高腰围和中心性肥胖风险低于北方(OR=0.57,95%CI:0.43~0.75;OR=0.62,95%CI:0.42~0.90);农村儿童青少年HDL-C降低的风险高于城市(OR=1.36,95%CI:1.02~1.83)。以家庭人均月收入低为参照,家庭人均月收入高的儿童青少年发生TC升高、LDL-C升高、TG升高、危险因素聚集的风险性高(OR=2.89,95%CI:1.42~5.87;OR=4.13,95%CI:1.75~9.71;OR=2.15,95%CI:1.17~3.95;OR=2.22,95%CI:1.26~3.91),家庭人均月收入中等的儿童青少年TG升高的风险高(OR=1.91,95%CI:1.11~3.29)。以非超重肥胖组为参照,超重组高腰围、HDL-C降低、血压升高、危险因素聚集的风险升高(OR=8.78,95%CI:6.06~12.70;OR=1.89,95%CI:1.32~2.71;OR=2.20,95%CI:1.47~3.28;OR=1.55,95%CI:1.00~2.40),肥胖组高腰围、TG升高、HDL-C降低、血压升高、危险因素聚集的风险升高(OR=16.67,95%CI:10.60~26.22;OR=2.94,95%CI:1.91~4.52;OR=2.87,95%CI:1.95~4.21;OR=1.90,95%CI:1.20~3.03;OR=7.60,95%CI:4.97~11.63)。见表 2。
本研究利用CCSNSD 2018年的调查数据分析我国四省7~17岁儿童青少年心血管代谢性危险因素的流行特征,并研究人口经济学因素与其的关系。心血管代谢性危险因素检出率由高到低依次为高腰围、HDL-C降低、血压升高、TG升高、血糖升高、中心性肥胖、TC升高、LDL-C升高。危险因素聚集的检出率为18.37%。地区、家庭人均月收入和BMI是其主要影响因素。
1991-2018年,随着我国社会经济的不断进步,儿童青少年膳食模式从以谷类、蔬菜和薯类为主的传统模式逐渐向以甜点、快餐、动物性食物等为主的西方模式转变[12]。这种膳食模式的转变以及居民消费水平的提高,使得儿童青少年可能摄入更多的脂类和能量,从而导致血脂异常等代谢性危险因素的检出率上升。而且,对于以肉类和水产类为主的肉类模式,南方地区儿童青少年该膳食模式的因子得分上升速度高于北方[12],这也是本研究中南方地区血脂异常检出率高于北方的主要原因。此外,收入对膳食结构的影响也进一步导致了代谢性危险因素的差异,我国18~35岁成年人[13]、≥60岁老年人[14]的高收入人群中都存在摄入脂类过多的现象。本研究中,除HDL-C降低外,其余3项血脂异常检出率和风险均随着家庭人均月收入提高而增加,这与高收入人群消费水平高,摄入脂类过多有关。
本研究中,高腰围是儿童青少年心血管代谢性危险因素中最突出的问题。IDF发布的儿童青少年代谢综合征专家共识中,将高腰围作为代谢综合征定义的必要条件之一[11]。随着腰围百分位数的增加,多种心血管危险因素及聚集的风险升高[15-16]。中国健康与营养调查数据显示,我国6~17岁儿童青少年的平均腰围在1993-2015年增加了4.04 cm,并且呈现增长趋势,高腰围(腰围 > P90)的检出率由1993年的5.0%上升到2015年的19.3%[17],结合本研究的检出率29.08%,提示我国儿童青少年高腰围仍呈现上升趋势。本研究根据BMI水平和高腰围共同判定中心性肥胖,检出率为7.33%,但我国对于儿童青少年中心性肥胖还没有统一的判定标准。Hosseini等[18]以腰围身高比≥0.5为标准,Liu等[19]以腰围P90为标准,对伊朗(5~19岁,2003-2015年)和美国(2~19岁,2011-2017年)人群中心性肥胖进行判定,均显示中心性肥胖呈现上升趋势。这表明无论在发展中国家还是发达国家,儿童青少年的高腰围和中心性肥胖都已成为不容忽视的问题,也提示我国应尽快制定儿童青少年中心性肥胖的判定标准,从而更有针对性地预防和干预。
儿童青少年超重、肥胖已经成为全球关注的问题,多项研究发现其与心血管危险因素有关[20-21],而且儿童期的超重肥胖与成年人期的CVD风险有关[4-5]。本研究中随着儿童青少年BMI的增加,多项危险因素的检出率呈上升趋势。值得注意的是,非超重肥胖组中有17.72%的儿童青少年存在高腰围的情况,有研究表明,单纯高腰围的儿童青少年比一般性肥胖的儿童青少年心血管代谢性危险因素检出率更高[22],这提示应注意非超重肥胖儿童青少年的代谢性危险因素状况。
本研究存在局限性。首先,所利用的CCSNSD数据只涉及我国四省,且调查的儿童青少年人数较少,代表性不足,无法全面反映我国儿童青少年心血管代谢性危险因素的整体情况;其次,本研究为横断面研究,对各危险因素及其聚集只能起到筛查作用,不能确定因果关系,未来应通过前瞻性研究进一步分析儿童青少年的心血管代谢性危险因素;最后,本研究城乡、家庭人均月收入之间的分布不均衡,可能对结果产生一定的影响。因此,本研究结果外推时需谨慎。
综上所述,2018年我国四省7~17岁儿童青少年高腰围、HDL-C降低、血压升高在心血管代谢性危险因素中较为突出,地区、家庭人均月收入、BMI是心血管代谢性危险因素的主要影响因素。我国儿童青少年心血管代谢性危险因素现状仍不容乐观,应在儿童时期控制危险因素,定期监测各危险因素水平,针对其不同时期生理特点及不同地区膳食模式等进行干预,以促进儿童青少年身心健康,减轻我国未来CVD负担。
利益冲突 所有作者声明无利益冲突
作者贡献声明 王志如:数据分析、论文撰写;李惟怡、姜红如、贾小芳、黄绯绯、胡霄、王惠君:论文指导、论文修改;张兵、王志宏:研究设计、论文修改、经费支持
志谢 感谢“神经系统疾病专病社区队列研究”项目组所有参与的工作人员和调查对象对本课题组工作的支持与配合
| [1] |
中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2021概要[J]. 中国循环杂志, 2022, 37(6): 553-578. The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2021: an updated summary[J]. Chin Circ J, 2022, 37(6): 553-578. DOI:10.3969/j.issn.1000-3614.2022.06.001 |
| [2] |
中华医学会心血管病学分会, 中国康复医学会心脏预防与康复专业委员会, 中国老年学和老年医学会心脏专业委员会, 等. 中国心血管病一级预防指南[J]. 中华心血管病杂志, 2020, 48(12): 1000-1038. Chinese Society of Cardiology of Chinese Medical Association, Cardiovascular Disease Prevention and Rehabilitation Committee of Chinese Association of Rehabilitation Medicine, Cardiovascular Disease Committee of Chinese Association of Gerontology and Geriatrics, et al. Chinese guideline on the primary prevention of cardiovascular diseases[J]. Chin J Cardiol, 2020, 48(12): 1000-1038. DOI:10.3760/cma.j.cn112148-20201009-00796 |
| [3] |
中华预防医学会, 中华预防医学会心脏病预防与控制专业委员会, 中华医学会糖尿病学分会, 等. 中国健康生活方式预防心血管代谢疾病指南[J]. 中华预防医学杂志, 2020, 54(3): 256-277. Chinese Preventive Medicine Association, Branch of Heart Disease Prevention and Control, Chinese Preventive Medicine Association, Chinese Diabetes Society, et al. Chinese guideline on healthy lifestyle to prevent cardiometabolic diseases[J]. Chin J Prev Med, 2020, 54(3): 256-277. DOI:10.3760/cma.j.issn.0253-9624.2020.03.006 |
| [4] |
Koskinen JS, Kytö V, Juonala M, et al. Childhood risk factors and carotid atherosclerotic plaque in adulthood: the cardiovascular risk in young Finns study[J]. Atherosclerosis, 2020, 293: 18-25. DOI:10.1016/j.atherosclerosis.2019.11.029 |
| [5] |
Drozdz D, Alvarez-Pitti J, Wójcik M, et al. Obesity and cardiometabolic risk factors: from childhood to adulthood[J]. Nutrients, 2021, 13(11): 4176. DOI:10.3390/nu13114176 |
| [6] |
席波. 预防成年期心血管疾病应始于儿童期[J]. 中华预防医学杂志, 2019, 53(7): 657-660. Xi B. Prevention of adult cardiovascular disease should start from childhood[J]. Chin J Prev Med, 2019, 53(7): 657-660. DOI:10.3760/cma.j.issn.0253-9624.2019.07.001 |
| [7] |
中华人民共和国国家卫生健康委员会. WS/T 611-2018 7岁~18岁儿童青少年高腰围筛查界值[S]. 北京: 中国标准出版社, 2018. National Health Commission of the People's Republic of China. WS/T 611-2018 High waist circumference screening threshold among children and adolescents aged 7-18 years[S]. Beijing: China Standard Press, 2018. |
| [8] |
中华人民共和国国家卫生和计划生育委员会. WS/T 586-2018学龄儿童青少年超重与肥胖筛查[S]. 北京: 中国标准出版社, 2018. National Health and Family Planning Commission of the People's Republic of China. WS/T 586-2018 Screening for overweight and obesity among school-age children and adolescents[S]. Beijing: China Standard Press, 2018. |
| [9] |
«中华儿科杂志»编辑委员会, 中华医学会儿科学分会儿童保健学组, 中华医学会儿科学分会心血管学组, 等. 儿童青少年血脂异常防治专家共识[J]. 中华儿科杂志, 2009, 47(6): 426-428. The Editorial Board of Chinese Journal of Pediatrics, Chinese Medical Association, Chinese Pediatric Society, The Subspecialty Groups of Child Health Care, Chinese Medical Association, Chinese Pediatric Society, The Subspecialty Groups of Cardiology, et al. The editorial board of Chinese journal of pediatrics children and adolescents[J]. Chin J Pediatr, 2009, 47(6): 426-428. DOI:10.3760/cma.j.issn.0578-1310.2009.06.007 |
| [10] |
中华人民共和国国家卫生健康委员会. WS/T 610-2018 7岁~18岁儿童青少年血压偏高筛查界值[S]. 北京: 中国标准出版社, 2018. National Health Commission of the People's Republic of China. WS/T 610-2018 Reference of screening for elevated blood pressure among children and adolescents aged 7-18 years[S]. Beijing: China Standard Press, 2018. |
| [11] |
Zimmet P, Alberti KGM, Kaufman F, et al. The metabolic syndrome in children and adolescents - an IDF consensus report[J]. Pediatr Diabetes, 2007, 8(5): 299-306. DOI:10.1111/j.1399-5448.2007.00271.x |
| [12] |
张继国, 王志宏, 黄绯绯, 等. 1991-2018年中国儿童青少年膳食模式的变迁[J]. 营养学报, 2021, 43(3): 213-217. Zhang JG, Wang ZH, Huang FF, et al. Changing trends in dietary patterns among Chinese children and adolescents from 1991 to 2018[J]. Acta Nutr Sin, 2021, 43(3): 213-217. DOI:10.3969/j.issn.0512-7955.2021.03.002 |
| [13] |
白晶, 王柳森, 王惠君, 等. 1989-2018年中国十五省(自治区、直辖市)18~35岁成年人膳食能量及宏量营养素摄入状况[J]. 卫生研究, 2022, 51(3): 361-366, 380. Bai J, Wang LS, Wang HJ, et al. Intakes of energy and macronutrient from Chinese 15 provinces (autonomous regions, municipalities) adults aged 18 to 35 in 1989-2018[J]. J Hyg Res, 2022, 51(3): 361-366, 380. DOI:10.19813/j.cnki.weishengyanjiu.2022.03.003 |
| [14] |
王柳森, 张兵, 王惠君, 等. 1991-2015年中国九省(自治区)老年居民膳食能量及宏量营养素摄入状况[J]. 卫生研究, 2019, 48(5): 700-705. Wang LS, Zhang B, Wang HJ, et al. Intakes of energy and macronutrient among the elderly in nine provinces (autonomous region), China during 1991-2015[J]. J Hyg Res, 2019, 48(5): 700-705. DOI:10.19813/j.cnki.weishengyanjiu.2019.05.002 |
| [15] |
Bauer KW, Marcus MD, El Ghormli L, et al. Cardio-metabolic risk screening among adolescents: understanding the utility of body mass index, waist circumference and waist to height ratio[J]. Pediatr Obes, 2015, 10(5): 329-337. DOI:10.1111/ijpo.267.Epub2014Dec17 |
| [16] |
马冠生, 季成叶, 马军, 等. 中国7~18岁学龄儿童青少年腰围界值点研究[J]. 中华流行病学杂志, 2010, 31(6): 609-615. Ma GS, Ji CY, Ma J, et al. Waist circumference reference values for screening cardiovascular risk factors in Chinese children and adolescents aged 7-18 years[J]. Chin J Epidemiol, 2010, 31(6): 609-615. DOI:10.3760/cma.j.issn.0254-6450.2010.06.003 |
| [17] |
Ma SJ, Hou DQ, Zhang YQ, et al. Trends in abdominal obesity among Chinese children and adolescents, 1993-2015[J]. J Pediatr Endocrinol Metab, 2020, 34(2): 163-169. DOI:10.1515/jpem-2020-0461 |
| [18] |
Hosseini M, Yousefifard M, Baikpour M, et al. Age-Period-cohort analysis of abdominal obesity in iranian children and adolescents: the CASPIAN study[J]. Int J Endocrinol Metab, 2020, 18(1): e82866. DOI:10.5812/ijem.82866 |
| [19] |
Liu JH, Zhao Y, Tian YL, et al. Trends in abdominal obesity and central adiposity measures by dual-energy X-Ray absorptiometry among US children: 2011-2018[J]. Front Pediatr, 2022, 10: 903413. DOI:10.3389/fped.2022.903413 |
| [20] |
Callo Quinte G, Barros F, Gigante DP, et al. Overweight trajectory and cardio metabolic risk factors in young adults[J]. BMC Pediatr, 2019, 19(1): 75. DOI:10.1186/s12887-019-1445-3 |
| [21] |
林星光, 方今女, 李医华. 小学生肥胖对心血管代谢危险因素及其聚集现象的影响[J]. 延边大学医学学报, 2015, 38(3): 192-195. Lin XG, Fang JN, Li YH. Influence of obesity in different metabolic factors and their clusters of cardiovascular risk in pupils[J]. J Med Sci Yanbian Univ, 2015, 38(3): 192-195. DOI:10.16068/j.1000-1824.2015.03.012 |
| [22] |
程红, 陈芳芳, 叶佩玉, 等. 2013-2015年中国7城市6~17岁儿童青少年心血管代谢危险因素的流行特征[J]. 中华预防医学杂志, 2018, 52(11): 1130-1135. Cheng H, Chen FF, Ye PY, et al. Characteristics of cardiometabolic risk factors of children and adolescents aged 6-17 years in seven cities in China from 2013 to 2015[J]. Chin J Prev Med, 2018, 52(11): 1130-1135. DOI:10.3760/cma.j.issn.0253-9624.2018.11.007 |