 2022, Vol. 43
2022, Vol. 43文章信息
- 吴倩, 关颖, 徐春泽, 王娜, 刘星, 江峰, 赵琦, 孙中兴, 赵根明, 姜永根.
- Wu Qian, Guan Ying, Xu Chunze, Wang Na, Liu Xing, Jiang Feng, Zhao Qi, Sun Zhongxing, Zhao Genming, Jiang Yonggen
- 血尿酸与糖尿病前期和新检出2型糖尿病的关系
- Relationship of serum uric acid with prediabetes and newly detected type 2 diabetes mellitus
- 中华流行病学杂志, 2022, 43(10): 1603-1610
- Chinese Journal of Epidemiology, 2022, 43(10): 1603-1610
- http://dx.doi.org/10.3760/cma.j.cn112338-20220117-00041
-
文章历史
收稿日期: 2022-01-17




2. 上海市松江区疾病预防控制中心, 上海 201620
2. Songjiang District Center for Disease Control and Prevention of Shanghai, Shanghai 201620, China
2型糖尿病是一种以血糖代谢紊乱为特征的慢性疾病,40年来,随着我国人口老龄化与生活方式的变化,2型糖尿病从少见病变成一种常见、高发疾病[1]。国际糖尿病联盟在2021年公布的数据表明[2],2021年中国2型糖尿病患病人数达到1.4亿,高居全球首位,且患病率逐年升高。有研究显示中国成年人2型糖尿病患病率从2013年的10.9%增加到2018年的12.4%;糖尿病前期的患病率从2013年的35.7%增加到2018年的38.1%[3]。
尿酸是人体内嘌呤代谢的终产物。尿酸氧化酶是一种负责将尿酸转化为尿囊素的酶,由于缺乏尿酸氧化酶,人类易患高尿酸血症[4]。近年来,随着研究者对血尿酸研究的加深,发现血尿酸与众多疾病存在关联,持续的高尿酸除了是导致痛风的直接原因以外,还有越来越多的研究表明尿酸与肾脏疾病[5]、高血压[6]、MS[7]、心血管疾病[8]等有关联。有研究结果显示,血尿酸升高与2型糖尿病呈正相关[9];也有研究显示,血尿酸升高与血糖之间呈负相关[10],一些研究表明血尿酸与2型糖尿病之间的关系呈现出性别的差异性[11],且血尿酸与血糖之间的关系在诊断为2型糖尿病前期后也出现不一致性[10]。因此本研究依托于一项大型的以社区为基础的成年人横断面调查,研究血尿酸浓度与新检出2型糖尿病和糖尿病前期之间的关系。
对象与方法1. 研究对象:来自上海市“高峰计划”松江区人群队列[12],该队列建于2016年4月至2017年12月,队列现场分别来自上海市松江区中山、新桥、佘山、泖港镇整群随机抽取的1/3居委会或行政村。研究对象具体纳入排除标准流程见图 1,最终纳入符合纳入排除标准的研究对象30 375名。本项目已通过复旦大学公共卫生学院医学研究伦理委员会批准(批准文号:IRB#2016-04-0586),调查开始之前已经取得研究对象的同意,并签署知情同意书。

|
| 图 1 30 375名研究对象纳入排除流程 |
2. 资料收集:
(1)问卷调查:通过调查问卷收集研究对象的基本人口学特征(年龄、性别、文化程度等)、日常生活习惯(吸烟、饮酒、锻炼等)和慢性病史(高血压、2型糖尿病、脂肪肝等)等资料。
(2)体格检查:身高、体重、血压等采用标准方法测量,身高测量采用金属立柱式身高计(精确到0.1 cm),体重测量采用电子体重秤(精确到0.1 kg);测量血压时要求研究对象静坐5 min以上,安静状态下测量右臂肱动脉的血压,测量3次取平均值[血压精确到1 mmHg(1 mmHg=0.133 kPa)]。
(3)实验室数据:所有研究对象需空腹至少8 h,于第二天早上由专业护士抽取静脉血,检测FPG、糖化血红蛋白(Hb1Ac)、血尿酸、TG、TC、LDL-C、HDL-C等指标。TC水平通过酶比色法(罗氏Cobas C501全自动生化分析仪)进行测定,LDL-C、HDL-C和TG则通过比色法(罗氏Cobas C501全自动生化分析仪)测定,FPG采用己糖激酶法(罗氏P800生化分析仪)测定,血清肌酐采用酶法(罗氏Cobas C702全自动生化分析仪)测定,血尿酸水平采用比色法(罗氏Cobas C702全自动生化分析仪)测定,HbA1c水平采用高效液相色谱法(东曹G8全自动糖化血红蛋白分析仪)测定。实验室检测统一由迪安医学检验中心完成。
3. 相关定义:新检出2型糖尿病:FPG≥7.0 mmol/L和(或)Hb1Ac≥6.5%,且自报之前未被诊断为2型糖尿病[13];糖尿病前期:6.1 mmol/L≤FPG < 7.0 mmol/L和(或)5.7%≤Hb1Ac < 6.5%,且自报之前未被诊断为2型糖尿病[13];高血压:SBP≥140 mmHg和(或)DBP≥90 mmHg,或自报有高血压病史;慢性肾病:自报有慢性肾病史;脂肪肝:自报有脂肪肝史;肾功能下降:根据校正的肾脏病饮食改良公式估算肾小球滤过率[14]:eGFR(ml/min/1.73 m2)=175×[血清肌酐(μmol/L)/88.4]-1.234×(年龄-0.179)×0.79(女性),以eGFR < 60 ml/min/1.73 m2为标准;BMI=体重(kg)/身高(m)2。
4. 质量控制:“高峰计划”松江区人群队列调查的实施过程及质量控制由松江区CDC和复旦大学公共卫生学院统筹。对于开展现场调查的各个街道(镇),由社区卫生服务中心负责该街道(镇)的调查实施和质量控制。制定统一的调查表和调查问卷填写细则,在进行调查前,由松江区CDC医生及复旦大学公共卫生学院现场指导老师对调查员进行统一、严格的培训,以确保调查质量。
5. 统计学分析:使用SPSS 26.0软件进行数据分析及处理,分类变量和等级变量分别采用χ2检验和Wilcoxon秩和检验进行组间比较。定量资料的数据先对其正态性进行检验,符合正态分布的数据资料使用x±s表示,并使用t检验及方差分析进行组间比较;不符合正态分布的数据资料使用M(Q1,Q3)表示,使用非参数检验(如秩和检验)进行组间比较。采用非条件logistic回归模型分析血尿酸水平对新检出2型糖尿病和糖尿病前期的影响。采用R软件用限制性立方样条(restricted cubic spline,RCS)曲线分析血尿酸水平与新检出2型糖尿病及糖尿病前期的非线性剂量反应关系。检验水准α=0.05,双侧检验,以P < 0.05为差异有统计学意义。
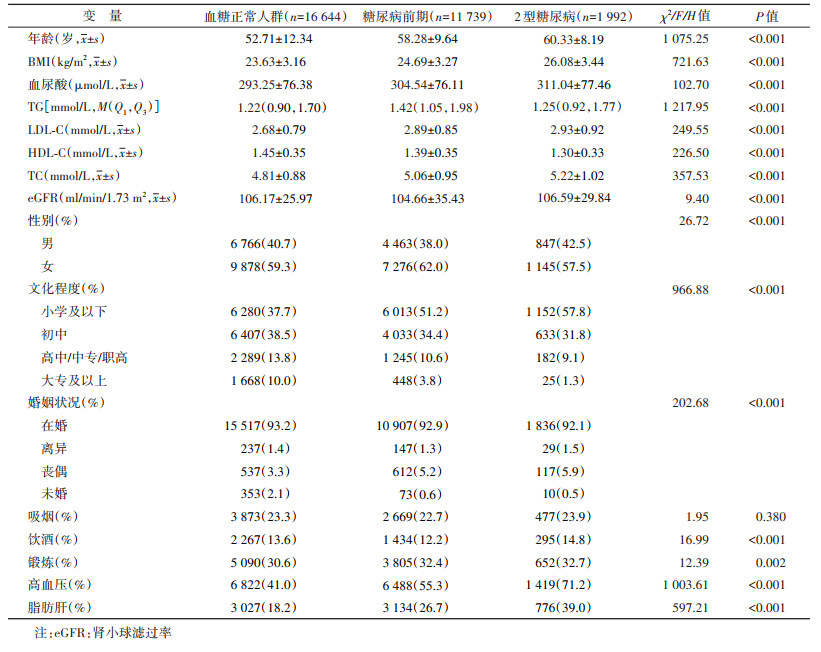
结果1. 一般特性:在30 375名研究对象中,女性18 299名(60.2%),男性12 076名(39.8%),年龄为(55.36±11.52)岁。基线调查新检出2型糖尿病、糖尿病前期患者分别为1 992名和11 739名,检出率为6.6%和38.6%。与血糖正常人群相比,2型糖尿病与糖尿病前期患者年龄较大,小学及以下文化程度所占比例较高,高血压、脂肪肝患病率较高,具有更高的BMI、血尿酸、TC、LDL-C、TG浓度,HDL-C浓度较低。研究对象具体特征见表 1。
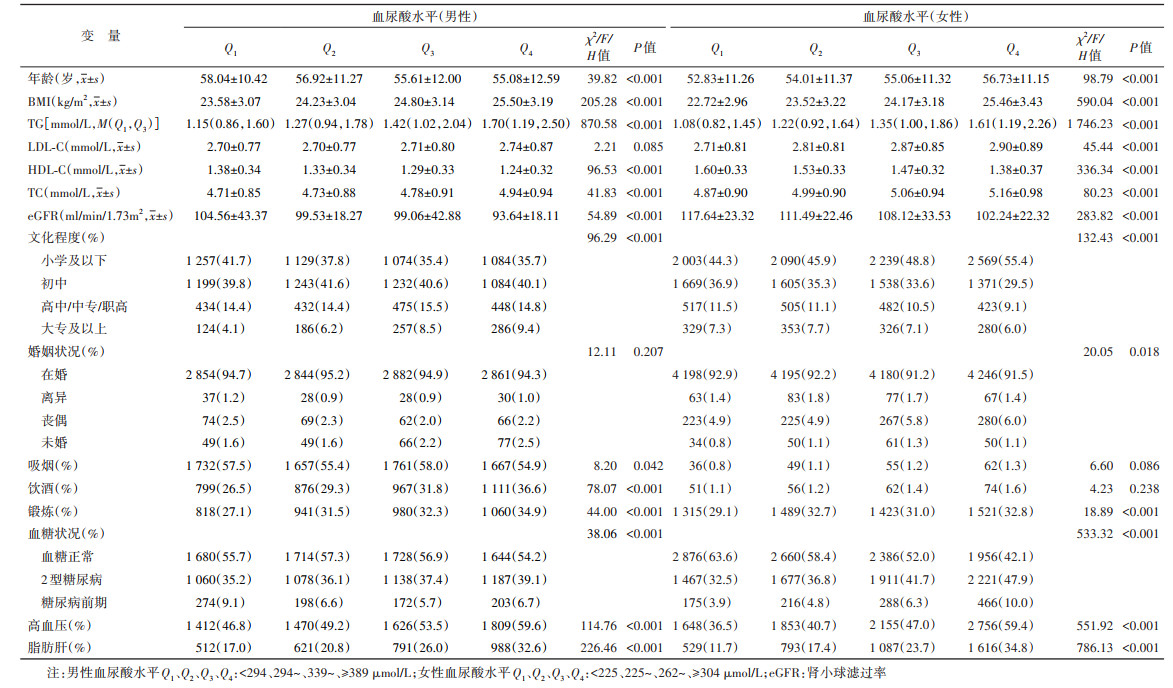
2. 血尿酸四分位数水平的基本情况:30 375名调查对象血尿酸水平M为290 µmol/L,其中女性血尿酸水平M为262 µmol/L,男性血尿酸水平M为339 µmol/L。将性别分层,根据血尿酸四分位数将调查对象分为4组时发现,在女性中,相较于Q1,Q2、Q3、Q4 3组研究对象年龄较大,但男性则相反。女性和男性的饮酒者比例均随血尿酸的浓度增加而增加,高血压和脂肪肝患病率也均随血尿酸浓度增加而增加,同时BMI、TG、TC浓度也均随血尿酸浓度增加而增加,但HDL-C和eGFR均随血尿酸浓度增加而降低。见表 2。
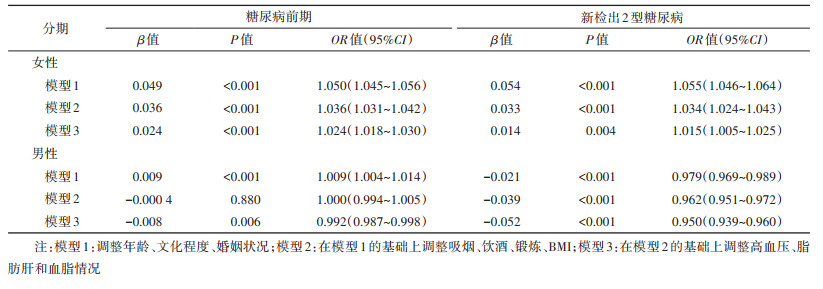
3. 血尿酸与2型糖尿病和糖尿病前期相关分析:以血糖正常人群为对照,分别以是否为新检出2型糖尿病(否=0;是=1)和糖尿病前期(否=0;是=1)为因变量,血尿酸为自变量,分别进行两次独立的二元logistic回归分析,在调整混杂变量之后的分析结果显示,在女性中,研究对象的血尿酸浓度每增加10 µmol/L,患糖尿病前期风险增加2.4%(OR=1.024,95%CI:1.018~1.030),患2型糖尿病风险增加1.5%(OR=1.015,95%CI:1.005~1.025);在男性中,血尿酸浓度每增加10 µmol/L,患糖尿病前期的风险减少0.8%(OR=0.992,95%CI:0.987~0.998),患2型糖尿病风险减少5.0%(OR=0.950,95%CI:0.939~0.960)。见表 3。
在校正年龄、文化程度、婚姻状况、吸烟、饮酒、锻炼、BMI、高血压、脂肪肝、TG、TC、LDL-C、HDL-C、eGFR后,在性别分层的基础上,采用5个节点的RCS模型分析血尿酸连续变化与新检出2型糖尿病和糖尿病前期的关系,女性血尿酸参考值为360 µmol/L,男性血尿酸参考值为420 µmol/L。RCS曲线显示,女性血尿酸水平与新检出2型糖尿病关联呈非线性剂量反应关系(P=0.017),但与糖尿病前期不呈非线性剂量反应关系(P=0.670)。男性血尿酸水平与糖尿病前期、新检出2型糖尿病均呈非线性剂量反应关系(糖尿病前期P=0.040;新检出2型糖尿病P=0.001)。见图 2,3。

|
| 图 2 女性血尿酸连续变化与糖尿病前期、新检出2型糖尿病的关系 |

|
| 图 3 男性血尿酸连续变化与糖尿病前期、新检出2型糖尿病的关系 |
本研究中在女性血尿酸与2型糖尿病和糖尿病前期的关系与已有的研究结果类似,一项日本的横断面研究显示[15],日本女性的血尿酸升高与空腹血糖受损呈正相关,血尿酸每增加1 mg/dl,空腹血糖受损风险增加36%(OR=1.36,95%CI:1.17~1.58),而男性血尿酸升高与空腹血糖受损之间的关联则无统计学意义(95%CI:0.92~1.09),文章中解释这种性别差异可能是由于男性和女性脂肪分布的差异所引起。在日本使用同一数据库的两篇文章显示[16-17],女性血尿酸升高也为2型糖尿病的独立危险因素,但男性血尿酸升高则为2型糖尿病的保护因素。同时从结果中可以看出,女性血尿酸每升高10 µmol/L,糖尿病前期风险增加2.4%(P < 0.001),而2型糖尿病风险增加1.5%(P=0.004),相对而言,血尿酸对2型糖尿病的影响小于糖尿病前期。在荷兰鹿特丹的一项研究也证实这一假设,即血尿酸可能参与导致糖尿病前期的代谢失衡的早期阶段,对诊断为2型糖尿病的晚期阶段影响较小[18]。
在本研究中,logistic回归分析结果和非线性结果均显示男性血尿酸升高与新检出2型糖尿病患病风险呈负相关,即在血尿酸较低时为新检出2型糖尿病的危险因素。但在糖尿病前期中,非线性结果显示男性血尿酸与糖尿病前期的关联无统计学意义。在以往的研究中,关于男性血尿酸与2型糖尿病和糖尿病前期关系的研究结果相互矛盾,有的研究显示血尿酸升高与2型糖尿病和糖尿病前期的关联为正相关[19],有的研究显示为负相关[20],有的研究关联性则无统计学意义[21]。这些研究大多受小样本的限制,且有些研究仅包含男性或者女性,没有根据性别进行分层分析,而有些研究选定的人群是一些特定人群,如工人,而不是一般人群。根据以往研究显示男性血尿酸与2型糖尿病的关系还可能存在种族差异[16]。美国第三次国家健康和营养检查中显示,男性血尿酸浓度与2型糖尿病患病风险呈负相关,与Q1相比,Q4血尿酸会减少患2型糖尿病风险0.32倍(95%CI:0.20~0.51)[22]。在日本一项研究中,男性血尿酸和Hb1Ac之间存在负线性相关关系,而女性则存在正线性相关关系[23]。另一项关于日本男性的研究中,与Q1相比,Q4血尿酸减少2型糖尿病风险65%(OR=0.35,95%CI:0.28~0.44),在该研究中,作者解释在男性中,低尿酸盐状态可能会通过提高氧化应激水平来诱导糖耐量受损[16]。在中国的一项前瞻性研究中显示,男性血尿酸与糖尿病前期的关联无统计学意义(P=0.30),而女性血尿酸升高则与糖尿病前期呈正相关(P=0.002),该作者认为产生性别差异是由于女性绝经引起的雌激素变化所导致,该研究进一步根据中国女性普遍绝经年龄48岁进行分层,结果显示,< 48岁女性血尿酸与糖尿病前期的关联无统计学意义,而≥48岁女性血尿酸与糖尿病前期呈正相关,进一步佐证其推测[24]。在本研究中,血尿酸与糖尿病和糖尿病前期的关系也表现出性别差异,根据以往流行病学研究表明,血尿酸水平与B细胞功能障碍之间仅在女性中存在相关性[25],这可能解释了血尿酸水平与2型糖尿病风险之间相关性的性别差异[11]。由于本研究未考虑女性绝经和口服避孕药情况,但有研究显示女性绝经状态和口服避孕药也会增加血尿酸水平[11],因此男性和女性的不同雌激素水平也可能是性别差异的一个解释。同时以往研究观察到的血尿酸升高与2型糖尿病之间的负相关结果的可能机制是与2型糖尿病患者高糖水平抑制近端小管中尿酸的再吸收有关,高血糖状态下,胰岛素缺乏增加血尿酸的排泄,导致糖尿病人群比正常人群血尿酸浓度更低[26],而这种机制在男性中更显著[16, 22]。因此关于男性血尿酸与2型糖尿病和糖尿病前期的关系还需要前瞻性研究进一步进行探究。
本研究的优点:①本研究是一项基于社区成年人的大型横断面研究,涉及20~74岁人群,样本量较大,代表性较好;②所有生化指标以及问卷内容都是由专业人员经过培训后按照标准流程进行检测和调查,真实性好;③排除已确诊为2型糖尿病患者以及痛风或高尿酸血症服药者,可排除降糖和降尿酸药物对研究结果的影响。
本研究存在局限性。①本研究为横断面研究,时序关系无法确定,因此无法验证血尿酸与2型糖尿病和糖尿病前期的因果关系;②血尿酸为动态变化指标,仅使用一次测量结果可能存在一定的信息偏倚;③未考虑饮食、基因等混杂因素,可能会影响结论的真实性。
利益冲突 所有作者声明无利益冲突
作者贡献声明 吴倩:数据整理、统计学分析、论文撰写;关颖、徐春泽、王娜、刘星、江峰:采集数据、行政技术或材料支持;赵琦、孙中兴:研究指导、论文修改;赵根明、姜永根:酝酿和设计实验、经费支持
| [1] |
中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2017年版)[J]. 中华糖尿病杂志, 2018, 10(1): 4-67. Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition)[J]. Chin J Diabetes Mellitus, 2018, 10(1): 4-67. DOI:10.3760/cma.j.issn.1674-5809.2018.01.003 |
| [2] |
International Diabetes Federation (IDF). IDF Diabetes Atlas 10th edition[EB/OL]. [2021-12-06]. http://www.diabetesatlas.org.
|
| [3] |
Wang LM, Peng W, Zhao ZP, et al. Prevalence and treatment of diabetes in China, 2013-2018[J]. JAMA, 2021, 326(24): 2498-2506. DOI:10.1001/jama.2021.22208 |
| [4] |
Huang H, Huang BT, Li YL, et al. Uric acid and risk of heart failure: a systematic review and meta-analysis[J]. Eur J Heart Fail, 2014, 16(1): 15-24. DOI:10.1093/eurjhf/hft132 |
| [5] |
Fathallah-shaykh SA, Cramer MT. Uric acid and the kidney[J]. Pediatr Nephrol, 2014, 29(6): 999-1008. DOI:10.1007/s00467-013-2549-x |
| [6] |
Yokoi Y, Kondo T, Okumura N, et al. Serum uric acid as a predictor of future hypertension: Stratified analysis based on body mass index and age[J]. Prev Med, 2016, 90: 201-206. DOI:10.1016/j.ypmed.2016.07.007 |
| [7] |
Jeong J, Suh YJ. Association between serum uric acid and metabolic syndrome in Koreans[J]. J Korean Med Sci, 2019, 34(48): e307. DOI:10.3346/jkms.2019.34.e307 |
| [8] |
Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. National health and nutrition examination survey[J]. JAMA, 2000, 283(18): 2404-2410. DOI:10.1001/jama.283.18.2404 |
| [9] |
Wu WC, Lai YW, Chou YC, et al. Serum uric acid level as a harbinger of type 2 diabetes: a prospective observation in Taiwan[J]. Int J Environ Res Public Health, 2020, 17(7): 2277. DOI:10.3390/ijerph17072277 |
| [10] |
Cheng F, Yin X, Duan WH, et al. Different-shaped curves for serum uric acid with and without diabetes: Results from China Health and Retirement Longitudinal Study[J]. J Diabetes, 2019, 11(6): 431-439. DOI:10.1111/1753-0407.12863 |
| [11] |
Lou YM, Qin P, Wang CY, et al. Sex-specific association of serum uric acid level and change in hyperuricemia status with risk of type 2 diabetes mellitus: a large cohort study in China[J]. J Diabetes Res, 2020, 2020, 9637365. DOI:10.1155/2020/9637365 |
| [12] |
Zhao Q, Chen B, Wang RP, et al. Cohort profile: protocol and baseline survey for the Shanghai Suburban Adult Cohort and Biobank (SSACB) study[J]. BMJ Open, 2020, 10(7): e035430. DOI:10.1136/bmjopen-2019-035430 |
| [13] |
中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2020年版)[J]. 中华糖尿病杂志, 2021, 13(4): 315-409. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 Edition)[J]. Chin J Diabetes Mellitus, 2021, 13(4): 315-409. DOI:10.3760/cma.j.cn115791-20210221-00095 |
| [14] |
胡丹, 樊友文, 涂卫平. 5种肾小球滤过率评估方程在2型糖尿病人群中的应用[J]. 中国实用内科杂志, 2020, 40(9): 744-748. Hu D, Fan YW, Tu WP. Performance of five estimated glomerular filtration rate equations in type 2 diabetes mellitus[J]. Chin J Pract Intern Med, 2020, 40(9): 744-748. DOI:10.19538/j.nk2020090109 |
| [15] |
Yamada T, Fukatsu M, Suzuki S, et al. Elevated serum uric acid predicts impaired fasting glucose and type 2 diabetes only among Japanese women undergoing health checkups[J]. Diabetes Metab, 2011, 37(3): 252-258. DOI:10.1016/j.diabet.2010.10.009 |
| [16] |
Wakabayashi I. Inverse associations between serum urate and glycemic status in a general population and in persons with diabetes mellitus[J]. Diabetol Metab Syndr, 2020, 12: 21. DOI:10.1186/s13098-020-00528-0 |
| [17] |
Wakabayashi I, Daimon T. Associations of blood urate level with glycemic status and other cardiometabolic risk factors in middle-aged women[J]. Womens Health Rep (New Rochelle), 2021, 2(1): 413-421. DOI:10.1089/whr.2021.0029 |
| [18] |
van der Schaft N, Brahimaj A, Wen KX, et al. The association between serum uric acid and the incidence of prediabetes and type 2 diabetes mellitus: The Rotterdam study[J]. PLoS One, 2017, 12(6): e0179482. DOI:10.1371/journal.pone.0179482 |
| [19] |
Nakanishi N, Okamoto M, Yoshida H, et al. Serum uric acid and risk for development of hypertension and impaired fasting glucose or Type Ⅱ diabetes in Japanese male office workers[J]. Eur J Epidemiol, 2003, 18(6): 523-530. DOI:10.1023/a:1024600905574 |
| [20] |
Oda E, Kawai R, Sukumaran V, et al. Uric acid is positively associated with metabolic syndrome but negatively associated with diabetes in Japanese men[J]. Intern Med, 2009, 48(20): 1785-1791. DOI:10.2169/internalmedicine.48.2426 |
| [21] |
Taniguchi Y, Hayashi T, Tsumura K, et al. Serum uric acid and the risk for hypertension and Type 2 diabetes in Japanese men: The Osaka Health Survey[J]. J Hypertens, 2001, 19(7): 1209-1215. DOI:10.1097/00004872-200107000-00005 |
| [22] |
Bandaru P, Shankar A. Association between serum uric acid levels and diabetes mellitus[J]. Int J Endocrinol, 2011, 2011, 604715. DOI:10.1155/2011/604715 |
| [23] |
Kawamoto R, Ninomiya D, Kasai Y, et al. Interaction between gender and uric acid on hemoglobin A1c in community-dwelling persons[J]. J Endocrinol Invest, 2018, 41(4): 421-429. DOI:10.1007/s40618-017-0760-5 |
| [24] |
Liu J, Zhao Z, Mu YM, et al. Gender differences in the association between serum uric acid and prediabetes: a six-year longitudinal cohort study[J]. Int J Environ Res Public Health, 2018, 15(7): 1560. DOI:10.3390/ijerph15071560 |
| [25] |
Shimodaira M, Niwa T, Nakajima K, et al. The relationship between serum uric acid levels and β-cell functions in nondiabetic subjects[J]. Horm Metab Res, 2014, 46(13): 950-954. DOI:10.1055/s-0034-1389996 |
| [26] |
Tuomilehto J, Zimmet P, Wolf E, et al. Plasma uric acid level and its association with diabetes mellitus and some biologic parameters in a biracial population of Fiji[J]. Am J Epidemiol, 1988, 127(2): 321-336. DOI:10.1093/oxfordjournals.aje.a114807 |