 2022, Vol. 43
2022, Vol. 43文章信息
- 张鑫, 刘少博, 从祥丰, 张润, 王文绢, 李剑虹.
- Zhang Xin, Liu Shaobo, Cong Xiangfeng, Zhang Run, Wang Wenjuan, Li Jianhong
- 中国成年人糖尿病前期发病状况及其影响因素研究
- Study on the incidence and influencing factors of prediabetes in Chinese adults
- 中华流行病学杂志, 2022, 43(10): 1582-1589
- Chinese Journal of Epidemiology, 2022, 43(10): 1582-1589
- http://dx.doi.org/10.3760/cma.j.cn112338-20211207-00957
-
文章历史
收稿日期: 2021-12-07




糖尿病前期又称糖调节受损,是位于正常血糖与糖尿病之间的一种疾病前状态,包括空腹血糖受损(impaired fasting glucose,IFG)和/或糖耐量受损(impaired glucose tolerance,IGT)。据国际糖尿病联盟(International Diabetes Federation,IDF)统计,2021年全球IGT患者约有5.410亿,预计到2030年为2.227亿,到2045年达7.303亿;2021年全球IFG患者约有3.190亿,预计到2030年达3.697亿,到2045年达4.408亿[1]。2018年,我国糖尿病前期患病率高达38.1%。糖尿病前期是糖尿病的危险因素[2],相比IFG而言,IGT的危险性更高,更易发展成为糖尿病[3-4]。IGT以糖负荷后高血糖为特征,每年约有4%~10%的IGT人群转化为2型糖尿病患者[5],同时糖尿病前期也是心血管疾病发生和死亡的重要危险因素[6-8]。目前我国对糖尿病前期进行的全国性队列研究较少。本研究基于2010年中国慢性病及其危险因素监测中的10省份数据,于2016-2017年进行随访调查,探讨我国成年人糖尿病前期发病状况及其影响因素。
对象与方法1. 研究对象: 2010年中国慢性病及其危险因素监测在全国162个监测点(包括新疆生产建设兵团农二师)开展,采用多阶段分层整群抽样方法选择≥18岁居民作为调查对象。采用与规模成比例的抽样方法,从每个监测点随机抽取4个乡镇(街道、团);从每个乡镇(街道、团)随机抽取3个行政村(居委会、连);从每个行政村(居委会、连)随机抽取1个居民小组(约50户),最后采用KISH表法从每户中随机抽取1人。本研究从2010年中国慢性病及其危险因素监测调查中,抽取河北、吉林、黑龙江、浙江、江西、河南、湖南、四川、贵州、陕西10省份,每个省份选择2个监测点(城市和农村各1个),将每个监测点中符合要求(血糖正常)的10 874人作为调查对象,于2016-2017年进行随访调查,最终随访7 048人。剔除基线随访不匹配者1 305人,年龄 < 18岁者22人,糖尿病或糖尿病前期信息不明者34人,基线血糖缺失者9人,随访血糖缺失者100人,最终纳入5 578名调查对象。本研究通过了中国CDC慢性非传染性疾病预防控制中心伦理审查委员会的审查(审批号: 201524B),调查对象均签署了知情同意书。
2. 调查内容: 基线和随访调查均包括询问调查、身体测量和实验室检测三部分。询问调查以面对面询问的方式进行。问卷内容包括个人基本信息、生活方式(吸烟、饮酒、饮食、身体活动水平等)、慢性病发生、诊断及控制情况。身体测量包括身高、体重、腰围和血压。实验室检测要求每位调查对象采集3管空腹10~12 h后静脉血5~6 ml,再采集1管服用75 g葡萄糖2 h后静脉血1 ml。检测指标包括FPG、糖负荷后2 h血糖、糖化血红蛋白和血脂。
3. 糖尿病前期诊断标准: 根据1999年WHO制定的标准[9],即FPG < 7.0 mmol/L且糖负荷后2 h血糖处于7.8~11.1 mmol/L(为IGT),和/或FPG处于6.1~7.0 mmol/L且糖负荷后2 h血糖 < 7.8 mmol/L(为IFG)。
4. 危险因素定义与分组: ①糖尿病家族史: 为一级亲属家族史,即在研究对象的父母、子女或兄弟姐妹中至少有一位患有糖尿病。②BMI(kg/m2): 根据《中国成人超重和肥胖症预防控制指南》[10],将BMI分为低体重(< 18.5),正常体重(18.5~),超重(24.0~),肥胖(≥28.0)。③血脂异常: 根据《中国成人血脂异常防治指南(2016年修订版)》[11],只要TC、HDL-C、LDL-C和TG中有一项超过诊断标准则判定为血脂异常。其中TG≥2.26 mmol/L为TG异常,TC≥6.22 mmol/L为TC异常,LDL-C≥4.14 mmol/L为LDL-C异常,HDL-C < 1.04 mmol/L为HDL-C异常。④高血压: SBP≥140 mmHg(1 mmHg=0.133 kPa)和(或)DBP≥90 mmHg,或近2周正在服用抗高血压药物者定义为高血压[12]。⑤中心性肥胖: 男性腰围≥85 cm或女性腰围≥80 cm。⑥吸烟: 调查时仍在吸烟的成年人为吸烟者。⑦饮酒: 在过去12个月内,喝过购买或自制的任何含有乙醇成分(包括白酒、啤酒、红酒、葡萄酒、果酒、黄酒和青稞酒等)的饮料[13]。⑧身体活动不足: 按Ainsworth等[14]提出的体育活动纲要,依据身体活动代谢当量(MET)值将身体活动水平分为高、中、低强度,对应的MET值分别为8.0、4.0、3.3。每周身体活动量=各种强度的MET值×每周活动频率(d/周)×每周活动时间(min/d)。身体活动量 < 600 MET-min/周为身体活动不足。
5. 统计学方法: 利用SAS软件进行数据整理与分析。对于连续性资料,符合正态分布或近似正态分布,用
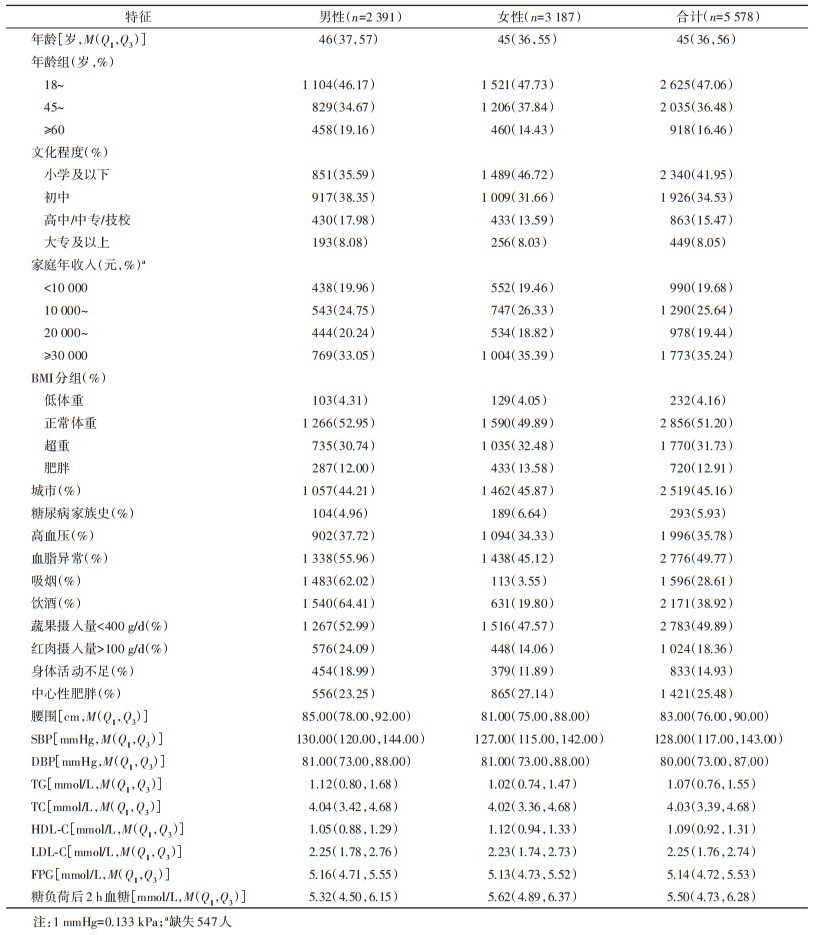
1. 基线特征: 5 578名研究对象中,男性2 391人,女性3 187人。年龄中位数为45岁,其中18~44岁年龄组占比最多(47.06%);文化程度多为小学及以下(41.95%)和初中(34.53%);超重、肥胖、糖尿病家族史、高血压、血脂异常的检出率分别为31.73%、12.91%、5.93%、35.78%、49.77%;28.61%的人群吸烟,男性吸烟者1 483人(92.92%);38.92%的人群饮酒,男性饮酒者1 540人(70.94%);约一半人群(49.89%)蔬果摄入量 < 400 g/d;18.36%的人群红肉摄入量 > 100 g/d;14.93%的人群身体活动不足。见表 1。
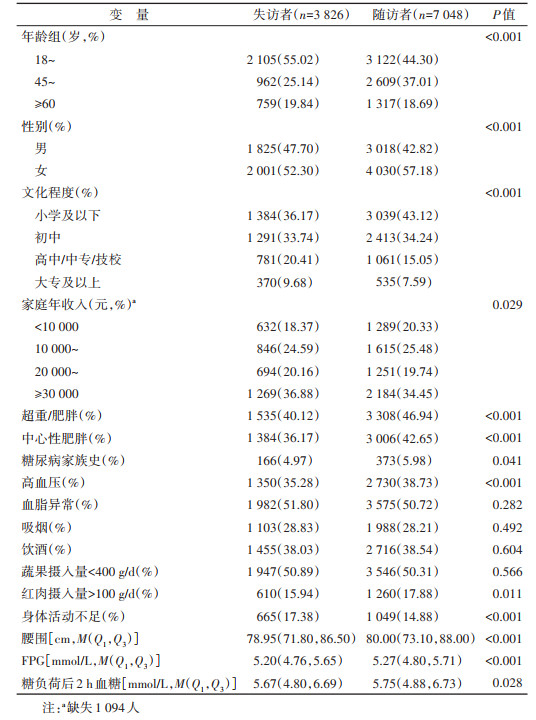
2. 失访人群与随访人群基线特征比较: 与随访人群相比,失访人群的腰围、FPG水平、糖负荷后2 h血糖水平偏低;45~59岁年龄组、女性、初中及以下文化程度、家庭年收入 < 20 000元、超重/肥胖、中心性肥胖、有糖尿病家族史、高血压患者以及红肉摄入量 > 100 g/d者比例较低,差异有统计学意义(均P < 0.05)。失访人群与随访人群在吸烟、饮酒、血脂异常以及蔬果摄入量 < 400 g/d分布上,两组人群差异无统计学意义(均P > 0.05)。见表 2。
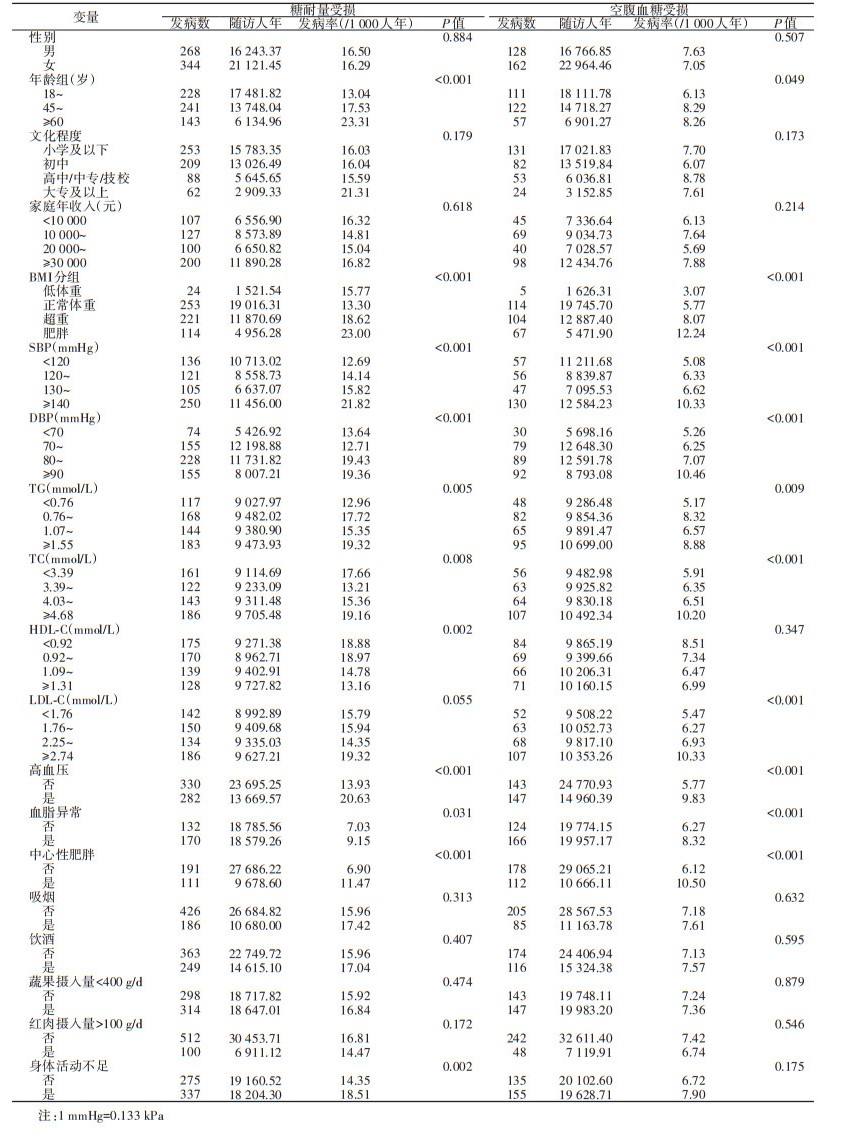
3. 糖尿病前期发病状况: 随访期间IGT发生612人(男性268人,女性344人),总计随访37 364.82人年,IGT发病率为16.4/1 000人年。不同年龄、BMI、SBP、DBP、TC、TG、HDL-C、身体活动水平、中心性肥胖、高血压、血脂异常,IGT发病率的差异有统计学意义(均P < 0.05)。不同性别、文化程度、家庭年收入、吸烟、饮酒、蔬果摄入量、红肉摄入量、LDL-C水平,IGT发病率的差异无统计学意义(均P > 0.05)。随访期间IFG发生290人(男性128人,女性162人),总计随访39 731.31人年,IFG发病率为7.3/1 000人年。不同年龄、BMI、SBP、DBP、TG、TC、LDL-C、中心性肥胖、高血压、血脂异常,IFG发病率的差异有统计学意义(均P < 0.05)。不同性别、文化程度、家庭年收入、吸烟、饮酒、蔬果摄入量、红肉摄入量、身体活动水平、HDL-C水平,IFG发病率的差异无统计学意义(均P > 0.05)。见表 3。
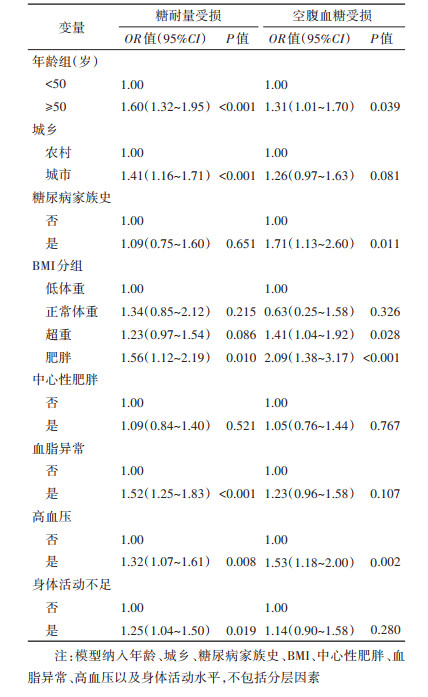
4. 多因素非条件logistic回归分析: 年龄≥50岁(OR=1.60,95%CI: 1.32~1.95)、城市居民(OR=1.41,95%CI: 1.16~1.71)、肥胖(OR=1.56,95%CI: 1.12~2.19)、血脂异常(OR=1.52,95%CI: 1.25~1.83)、高血压(OR=1.32,95%CI: 1.07~1.61)以及身体活动不足(OR=1.25,95%CI: 1.04~1.50)是IGT发病的危险因素;年龄≥50岁(OR=1.31,95%CI: 1.01~1.70)、糖尿病家族史(OR=1.71,95%CI: 1.13~2.60)、超重(OR=1.41,95%CI: 1.04~1.92)、肥胖(OR=2.09,95%CI: 1.38~3.17)以及高血压(OR=1.53,95%CI: 1.18~2.00)是IFG发病的危险因素。见表 4。
我国糖尿病患病率处于增长状态[15]。糖尿病可引起多种并发症,包括肾衰竭、失明、心血管疾病和死亡等[16]。据IDF估计,2019年,全球20~79岁的成年人中,约有420万人死于糖尿病,占总死亡人数的11.3%[17]。糖尿病带来了严重的社会及经济负担。2019年,全球与糖尿病相关的医疗支出总额约为7 600亿美元,其中50~79岁人群支出居多(占69%),2030年预计支出增至每年8 250亿美元[18]。糖尿病前期是糖尿病的危险因素,且该阶段患者的机体就已发生可导致糖尿病并发症的病理生理学变化[19],但IFG与IGT具有不同的病理生理学背景,IGT更易发展为糖尿病[4, 20-21]。目前我国关于糖尿病前期的全国性队列研究较少,因此对我国成年人进行糖尿病前期的发病状况及其影响因素队列研究,对发现我国糖尿病前期的高危人群并采取针对性的干预措施以减少糖尿病及其并发症的发生具有重要意义。
本研究结果显示,我国成年人IGT发病率为16.4/1 000人年,IFG发病率为7.3/1 000人年,相对IFG而言,IGT发病率更高。本研究存在一定的失访,失访人群相对随访人群FPG水平、糖负荷后2 h血糖水平偏低,IGT与IFG的发病率可能会存在高估的现象。但我国糖尿病前期患病率呈上升趋势[2],降低我国糖尿病前期以及糖尿病发生的工作刻不容缓。
本研究多因素非条件logistic回归分析结果显示,年龄≥50岁者糖尿病前期发病危险性升高,在我国青岛市和伊朗等进行的多个研究也表明了年龄是糖尿病前期的危险因素[22-24],原因可能是随着年龄的增长身体素质下降,各个器官的功能有所衰退,也可能是随着年龄的增长身体活动减少,体重增加进一步引起糖尿病前期的发病。本研究结果也证明了肥胖与糖尿病前期的发病相关,这与大多数研究结果一致[23, 25-26]。但是由于生活方式的改变,目前学习和大部分的工作静坐时间较长[27],导致我国的肥胖人群队伍仍有扩大趋势[28],故我国应积极倡导并加大控制体重的力度。本研究和其他多项研究均表明高血压是糖尿病前期的危险因素[22-23, 26, 29]。可能是因为高血压与糖尿病前期均属于MS,且二者具有相同的病理学基础—胰岛素抵抗。Salvetti等[30]的研究表明胰岛素抵抗是高血压产生的原因,Schianca等[31]的研究显示在糖尿病前期人群中存在明显的胰岛素抵抗,故高血压患者应注重糖尿病前期的筛查。本研究结果显示血脂异常患者IGT发病风险增高,这与2004和2009年在我国青岛市进行的调查研究[32]以及在西班牙进行的一项前瞻性研究[33]结论一致;血脂异常患者IFG的发病也增高,这与一项对IFG的自然过程综述表明IFG一般有较高的LDL-C和较低的HDL-C表述一致[21],因此我国应进一步呼吁国民注重清淡饮食,适量增加体育运动。我国大庆市20年随访研究结果表明,采用联合生活方式对IGT干预可以使糖尿病发病率降低51%[34],提示对糖尿病前期的预防应采取综合性的干预方式。
本研究存在不足。首先,本研究存在一定的失访,糖尿病前期的发病率可能会出现高估的现象。其次,虽然本研究考虑了大部分的混杂因素,但由于糖尿病前期影响因素较多,基线调查未收集所有的暴露信息,一些未测量指标(如激素水平、焦虑抑郁等)未纳入模型调整,可能会导致残余混杂。
综上所述,年龄≥50岁者、超重/肥胖人群、高血压患者、血脂异常者、身体活动不足者以及有糖尿病家族史者易发生糖尿病前期,相比IFG,IGT发病率较高。为预防糖尿病前期的发生,中老年人群、超重/肥胖人群、患有高血压者以及有糖尿病家族史者应重视糖尿病前期的筛查,加强宣传体育锻炼的重要性。
利益冲突 所有作者声明无利益冲突
作者贡献声明 张鑫: 数据分析、论文撰写;刘少博、从祥丰、张润、王文绢: 数据收集、整理与分析;李剑虹: 研究设计、论文修改、经费支持
| [1] |
International Diabetes Federation Diabetes Atlas 10th edition, 2021, IDF, Brussels[EB/OL]. (2021-12-06) [2021- 12-07]. https://www.idf.org/.
|
| [2] |
Wang LM, Peng W, Zhao ZP, et al. Prevalence and treatment of diabetes in China, 2013-2018[J]. JAMA, 2021, 326(24): 2498-2506. DOI:10.1001/jama.2021.22208 |
| [3] |
Piller C. Dubious diagnosis[J]. Science, 2019, 363(6431): 1026-1031. DOI:10.1126/science.363.6431.1026 |
| [4] |
巩秋红, 李光伟. 糖尿病的发动机: 轻度血糖升高, 还是高胰岛素需求?——也谈高危人群预防糖尿病[J]. 中华内科杂志, 2019, 58(8): 556-559. Gong QH, Li GW. The engine of diabetes: mild hyperglycemia or increased insulin demands? Prevention of diabetes in high risk population[J]. Chin J Intern Med, 2019, 58(8): 556-559. DOI:10.3760/cma.j.issn.0578-1426.2019.08.002 |
| [5] |
王瑶, 王金平, 李光伟, 等. 糖耐量受损转化为正常糖耐量或演变为糖尿病者血压均下降——来自大庆糖尿病研究的新发现[J]. 中华内分泌代谢杂志, 2008, 24(3): 268-271. Wang Y, Wang JP, Li GW, et al. Blood pressure reduction found in subjects after evolution of impaired glucose tolerance to normal glucose tolerance or diabetes—New information from The Da-Qing IGT and Diabetes Study[J]. Chin J Endocrinol Metab, 2008, 24(3): 268-271. DOI:10.3321/j.issn:1000-6699.2008.03.009 |
| [6] |
王金平, 陈燕燕, 巩秋红, 等. 糖尿病和心血管病预防的破冰之旅——大庆糖尿病预防研究30年[J]. 中国科学: 生命科学, 2018, 48(8): 902-908. Wang JP, Chen YY, Gong QH, et al. Breakthrough in diabetes and cardiovascular disease prevention: a 30-year study of diabetes prevention in Daqing[J]. Sci Sin Vitae, 2018, 48(8): 902-908. DOI:10.1360/N052018-00045 |
| [7] |
Ali MK, Bullard KM, Saydah S, et al. Cardiovascular and renal burdens of prediabetes in the USA: analysis of data from serial cross-sectional surveys, 1988-2014[J]. Lancet Diabetes Endocrinol, 2018, 6(5): 392-403. DOI:10.1016/S2213-8587(18)30027-5 |
| [8] |
Diabetes Prevention Program Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the diabetes prevention program outcomes study[J]. Lancet Diabetes Endocrinol, 2015, 3(11): 866-875. DOI:10.1016/S2213-8587(15)00291-0 |
| [9] |
Alberti KGMM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO consultation[J]. Diabet Med, 1998, 15(7): 539-553. DOI:10.1002/(SICI)1096-9136(199807)15:7<539:AID-DIA668>3.0.CO;2-S |
| [10] |
陈春明, 孔灵芝. 中国成人超重和肥胖症预防控制指南[M]. 北京: 人民卫生出版社, 2006. Chen CM, Kong LZ. Guidelines for the prevention and control of overweight and obesity in Chinese adults[M]. Beijing: People's Medical Publishing House, 2006. |
| [11] |
中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南(2016年修订版)[J]. 中华全科医师杂志, 2017, 16(1): 15-35. Joint Committee Issued Chinese Guideline for the Management of Dyslipidemia. 2016 Chinese guideline for the management of dyslipidemia in adults[J]. Chin J Gen Pract, 2017, 16(1): 15-35. DOI:10.3760/cma.j.issn.1671-7368.2017.01.006 |
| [12] |
王增武, 王文. 中国高血压防治指南(2018年修订版)解读[J]. 中国心血管病研究, 2019, 17(3): 193-197. Wang ZW, Wang W. Interpretation of Chinese guidelines for the management of hypertension (2018 revised edition)[J]. Chin J Cardiovasc Res, 2019, 17(3): 193-197. DOI:10.3969/j.issn.1672-5301.2019.03.001 |
| [13] |
中华医学会肝病学分会脂肪肝和酒精性肝病学组. 非酒精性脂肪性肝病诊疗指南(2010年修订版)[J]. 胃肠病学和肝病学杂志, 2010, 19(6): 483-487. Chinese Journal of Gastroenterology and Hepatology. Guidelines for management of nonalcoholic fatty liver disease: an updated and revised edition[J]. Chin J Gastroenterol Hepatol, 2010, 19(6): 483-487. DOI:10.3969/j.issn.1006-5709.2010.06.001 |
| [14] |
Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities: an update of activity codes and MET intensities[J]. Med Sci Sports Exerc, 2000, 32(9 Suppl): S498-504. DOI:10.1097/00005768-200009001-00009 |
| [15] |
Ma RCW. Epidemiology of diabetes and diabetic complications in China[J]. Diabetologia, 2018, 61(6): 1249-1260. DOI:10.1007/s00125-018-4557-7 |
| [16] |
李炼. 老年2型糖尿病慢性并发症的临床研究[J]. 中国老年学杂志, 2019, 39(18): 4619-4622. Li L. Clinical study of chronic complications in elderly patients with type 2 diabetes mellitu[J]. Chin J Gerontol, 2019, 39(18): 4619-4622. DOI:10.3969/j.issn.1005-9202.2019.18.076 |
| [17] |
Saeedi P, Salpea P, Karuranga S, et al. Mortality attributable to diabetes in 20-79 years old adults, 2019 estimates: results from the international diabetes federation diabetes atlas, 9th edition[J]. Diabetes Res Clin Pract, 2020, 162: 108086. DOI:10.1016/j.diabres.2020.108086 |
| [18] |
Williams R, Karuranga S, Malanda B, et al. Global and regional estimates and projections of diabetes-related health expenditure: results from the International Diabetes Federation Diabetes Atlas, 9th edition[J]. Diabetes Res Clin Pract, 2020, 162: 108072. DOI:10.1016/j.diabres.2020.108072 |
| [19] |
Koller KR, Day GE, Hiratsuka VY, et al. Increase in diabetes among urban Alaska Native people in the Alaska EARTH follow-up study: a call for prediabetes screening, diagnosis, and referral for intervention[J]. Diabetes Res Clin Pract, 2020, 167: 108357. DOI:10.1016/j.diabres.2020.108357 |
| [20] |
李叶青, 罗秋林, 蒲云飞, 等. 糖耐量受损对冠状动脉临界病变的影响[J]. 检验医学与临床, 2017, 14(11): 1611-1613. Li YQ, Luo QL, Pu YF, et al. Influence of impaired glucose tolerance on coronary borderline lesion[J]. Lab Med Clin, 2017, 14(11): 1611-1613. DOI:10.3969/j.issn.1672-9455.2017.11.033 |
| [21] |
Święcicka-Klama A, Połtyn-Zaradna K, Szuba A, et al. The natural course of impaired fasting glucose[J]. Adv Exp Med Biol, 2021, 1324, 41-50. DOI:10.1007/5584_2020_571 |
| [22] |
王建新, 孙建平, 王枫, 等. 青岛市中老年人糖尿病及糖调节受损的流行现状分析[J]. 预防医学论坛, 2014, 20(4): 256-259. Wang JX, Sun JP, Wang F, et al. Analysis on the prevalence of diabetes and impaired glucose regulation among middle-aged and elderly residents, Qingdao City[J]. Prev Med Trib, 2014, 20(4): 256-259. DOI:10.16406/j.pmt.issn.1672-9153.2014.04.032 |
| [23] |
Sadeghi M, Talaei M, Rizi EP, et al. Determinants of incident prediabetes and type 2 diabetes in a 7-year cohort in a developing country: the Isfahan cohort study[J]. J Diabetes, 2015, 7(5): 633-641. DOI:10.1111/1753-0407.12236 |
| [24] |
Yang WY, Lu JM, Weng JP, et al. Prevalence of diabetes among men and women in China[J]. N Engl J Med, 2010, 362(12): 1090-1101. DOI:10.1056/NEJMoa0908292 |
| [25] |
颜玮, 朱丽萍, 陈轶英, 等. 江西省流动人口糖尿病及糖调节受损影响因素分析[J]. 中华疾病控制杂志, 2015, 19(11): 1105-1108. Yan W, Zhu LP, Chen YY, et al. Analysis on influencing factors of diabetes mellitus and impaired glucose regulation among floating population in Jiangxi Province[J]. Chin J Dis Control Prev, 2015, 19(11): 1105-1108. DOI:10.16462/j.cnki.zhjbkz.2015.11.007 |
| [26] |
Hu Z, Gao F, Qin LL, et al. A case-control study on risk factors and their interactions with prediabetes among the elderly in rural communities of Yiyang City, Hunan Province[J]. J Diabetes Res, 2019, 2019, 1386048. DOI:10.1155/2019/1386048 |
| [27] |
Fan S, Chen JC, Huang JF, et al. Physical activity level and incident type 2 diabetes among Chinese adults[J]. Med Sci Sports Exerc, 2015, 47(4): 751-756. DOI:10.1249/MSS.0000000000000471 |
| [28] |
Nie P, Ding LL, Sousa-Poza A. Decomposing adult obesity trends in China (1991-2011)[J]. Econ Hum Biol, 2019, 34: 5-15. DOI:10.1016/j.ehb.2019.02.001 |
| [29] |
席天舒, 潘利, 任晓岚, 等. 甘肃省糖尿病、糖尿病前期患病率及影响因素分析[J]. 中华疾病控制杂志, 2018, 22(10): 987-991. Xi TS, Pan L, Ren XL, et al. The prevalence and associated factors of diabetes and pre-diabetes in Gansu Province[J]. Chin J Dis Control Prev, 2018, 22(10): 987-991. DOI:10.16462/j.cnki.zhjbkz.2018.10.002 |
| [30] |
Salvetti A, Brogi G, Di Legge V, et al. The inter-relationship between insulin resistance and hypertension[J]. Drugs, 1993, 46 Suppl 2: 149-159. DOI:10.2165/00003495-199300462-00024 |
| [31] |
Schianca GPC, Rossi A, Sainaghi PP, et al. The significance of impaired fasting glucose versus impaired glucose tolerance: importance of insulin secretion and resistance[J]. Diabetes Care, 2003, 26(5): 1333-1337. DOI:10.2337/diacare.26.5.1333 |
| [32] |
Cui J, Sun JP, Wang W, et al. Triglycerides and total cholesterol concentrations in association with IFG/IGT in Chinese adults in Qingdao, China[J]. BMC Public Health, 2018, 18(1): 444. DOI:10.1186/s12889-018-5286-z |
| [33] |
Díaz-Redondo A, Giráldez-García C, Carrillo L, et al. Modifiable risk factors associated with prediabetes in men and women: a cross-sectional analysis of the cohort study in primary health care on the evolution of patients with prediabetes (PREDAPS-Study)[J]. BMC Fam Pract, 2015, 16: 5. DOI:10.1186/s12875-014-0216-3 |
| [34] |
Li GW, Zhang P, Wang JP, et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up study[J]. Lancet, 2008, 371(9626): 1783-1789. DOI:10.1016/S0140-6736(08)60766-7 |