 2022, Vol. 43
2022, Vol. 43文章信息
- 苏宇, 湛浩然, 孙鑫, 陈茹, 孙丽, 郝金娟, 张效鹏, 田雨, 陈瑞.
- Su Yu, Zhan Haoran, Sun Xin, Chen Ru, Sun Li, Hao Jinjuan, Zhang Xiaopeng, Tian Yu, Chen Rui
- 全球针对家族史高危人群的结直肠癌筛查指南推荐意见的系统综述
- Global guidelines of colorectal cancer screening in high-risk population with family history of colorectal cancer: a systematic review
- 中华流行病学杂志, 2022, 43(9): 1469-1478
- Chinese Journal of Epidemiology, 2022, 43(9): 1469-1478
- http://dx.doi.org/10.3760/cma.j.cn112338-20220422-00331
-
文章历史
收稿日期: 2022-04-22




2. 国家癌症中心/国家肿瘤临床医学研究中心/中国医学科学院北京协和医学院肿瘤医院, 北京 100021;
3. 人民卫生出版社有限公司, 北京 100021;
4. 北京医院/国家老年医学中心/中国医学科学院老年医学研究院, 北京 100730;
5. 北京大学肿瘤医院暨北京市肿瘤防治研究所/胃肠肿瘤中心一病区/恶性肿瘤发病机制及转化研究教育部重点实验室, 北京 100142
2. National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China;
3. People's Medical Publishing House, Beijing 100021, China;
4. Beijing Hospital/National Center of Gerontology/Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing 100730, China;
5. Gastrointestinal Cancer Center, Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Peking University Cancer Hospital and Institute, Beijing 100142, China
结直肠癌是临床上常见的消化系统恶性肿瘤,在全球范围内其发病率居于恶性肿瘤第3位,死亡率高居第2位[1]。在我国,结直肠癌的发病率呈逐年上升趋势,成为我国消化系统中发病率第1位、死亡率第4位的恶性肿瘤,严重威胁人民的生命健康,造成沉重的社会负担[2]。筛查是实现结直肠癌早诊早治的关键前提,大量研究证实,连续性的结直肠癌筛查可以有效降低结直肠癌的发病率和死亡率[3-4]。目前部分欧美国家已经建立起较为完善的结直肠癌筛查体系,而我国的结直肠癌筛查开展于20世纪70年代,目前仅在部分省市或地区开展区域性的结直肠癌筛查[5]。研究证据表明,结直肠癌的发生发展除了与环境因素、生活方式有关,还与结直肠癌家族史显著相关,且受患病亲属关系和数量的影响[6-8]。尽管在全球现行的结直肠癌筛查指南中,家族史常常作为风险分层的高危因素,然而仅有部分指南根据详细的家族史分类做出具体筛查推荐,而多数筛查指南未能针对结直肠癌家族史高危人群提供更深层次的建议。本研究采用系统综述的方式对全球现行筛查指南中针对具有非遗传性结直肠癌家族史人群的筛查推荐意见进行整理汇总,排除林奇综合征或家族性腺瘤病等高外显遗传性结直肠癌综合征的推荐意见,深入了解指南制定和更新现状,系统梳理筛查方案,为我国针对家族史高危人群的结直肠癌筛查策略的更新提供参考依据。
资料与方法1. 资料来源:系统检索中国知网、万方数据知识服务平台、PubMed、Embase、Cochrane Library、Web of Science,手工检索国际指南协作网(Guideline International Network)、美国癌症协会、世界胃肠病组织等专业机构的官网,以及主要国家卫生系统官网刊登的结直肠癌筛查指南/共识作为补充,并且手工检索通过引文追溯得到的指南/共识文献。语种限定为中文和英文。计算机检索时限均为建库至2022年5月24日。
2. 文献检索式:英文:[(colorectal cancer) AND (screening) AND (family history)] AND [(guideline) OR (recommendation)],中文:[“结直肠癌”和“筛查”和“家族史”和(“指南”或“共识”或“推荐”)]。
3. 文献筛选:
(1) 纳入标准:公开发布的原创的与结直肠癌筛查相关的指南/共识/推荐意见;有多次更新版本的,则纳入最新版本;由官方或专业组织制定的均纳入;语种限定为中文或英文。
(2) 排除标准:仅关于指南/共识/意见的介绍、评价、解读等文献,未包含筛查方案;重复文献;非最新版本;指南/共识/意见的翻译版本或限定语种之外的版本;非结直肠癌、非筛查类和非独立内容呈现的指南/共识/意见;非针对高危人群的指南/共识/意见;会议摘要或无全文的文献。最终共纳入文献20篇,文献筛选过程见图 1。

|
| 图 1 文献筛选流程 |
4. 资料提取:制定文献信息摘录表,包括指南的基本信息(发布组织所在地区、发布时间、发布机构、指南名称、指南版本)和高危人群的结直肠癌筛查推荐意见(家族史详细分类、筛查起止年龄、筛查方式、筛查周期)。对所有针对结直肠癌家族史高危人群筛查指南的发布情况、筛查推荐意见进行系统汇总。
5.数据分析:在初步筛选文献时,制定统一的筛选流程与说明,利用Endnote X9软件对检索到的文献进行管理,排除重复文献。筛选时,阅读题目与摘要,在排除不相关的文献后,进行全文阅读,以确定最终是否被纳入。由两位研究者独立筛选文献和提取资料,并交叉核对,如有意见不统一,则讨论决定或交由第三人协助裁定。
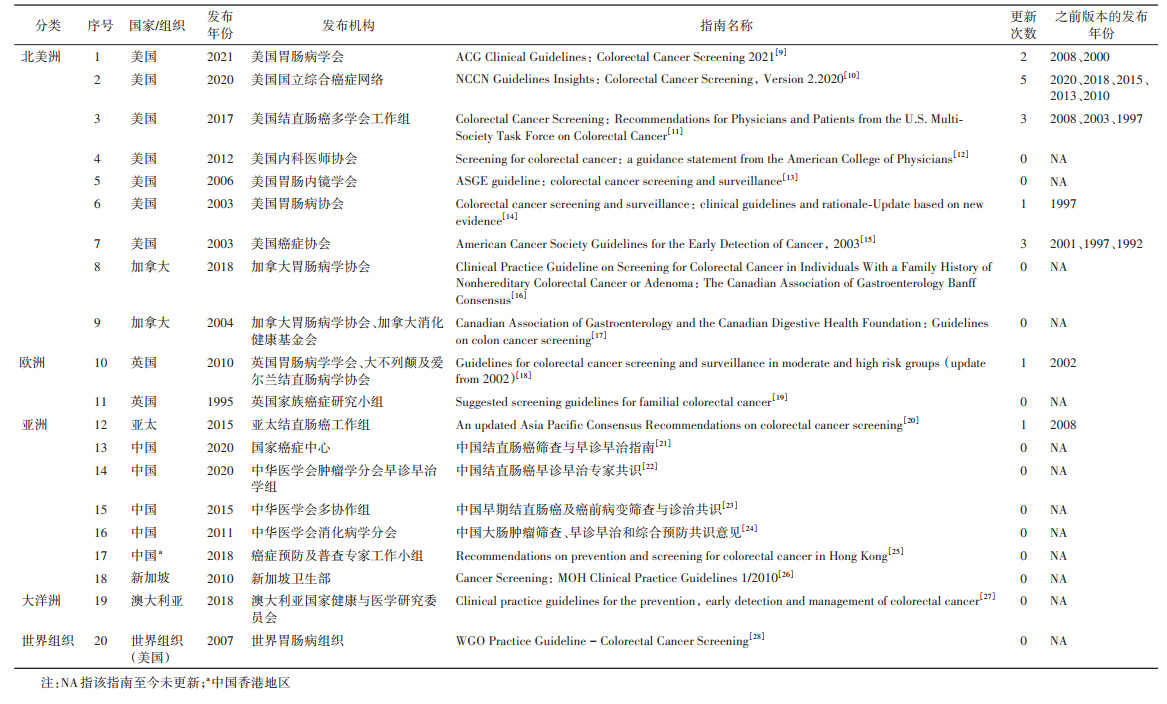
结果1. 基本信息:目前全球主要国家均发布了针对结直肠癌家族史高危人群的筛查指南。共纳入指南20部,发布时间范围为1995-2021年。所有纳入指南均为较权威的国家或地区性规划的指导文件或专业学术机构发布的推荐文件。见表 1。按发布指南的国家/地区/机构、发布时间、发布机构、指南名称以及更新情况对各指南的基本信息进行梳理。
2. 结直肠癌筛查指南中针对家族史高危人群的推荐内容:目前,全球现行结直肠癌筛查指南中的意见都推荐为不同风险分层的人群开展不同的结直肠癌筛查策略,其中,结直肠癌家族史常常作为筛查指南中主要的风险分层因素,具体包括患病亲属关系、数量和诊断年龄。研究表明,患结直肠癌的亲属关系等级越高、数量越多、发病年龄越小,个体的发病风险将会显著增加[6]。多数指南对结直肠癌患病亲属关系等级及数量给出了明确界定,其中部分指南还进一步对患病亲属的诊断年龄进行了详细阐述。针对结直肠癌家族史高危人群的筛查推荐意见见表 2。
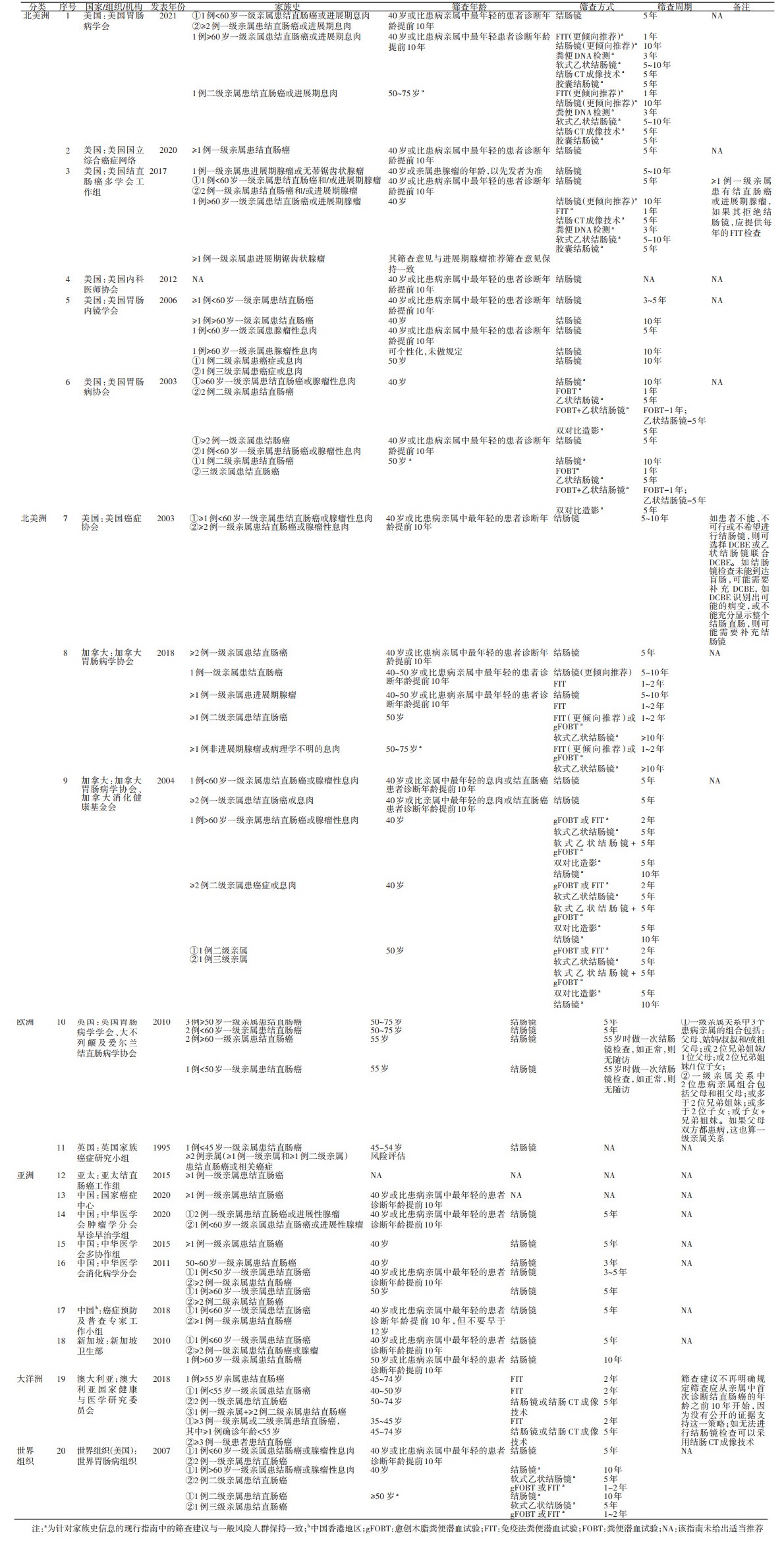
对于1例一级亲属患病的家族史情况,最常见的是以患病亲属诊断年龄60岁作为切点划分,英国对于一级亲属诊断年龄的切点值提前到45岁或50岁[18-19],我国中华医学会消化病学分会建议为50岁或60岁[24],澳大利亚则将此年龄切点值提前到55岁[27]。对于一级亲属在60岁前患结直肠癌的情况,北美地区(美国[9, 11, 14-15]、加拿大[17])、亚洲地区(中国[22, 25]、新加坡[26])、世界胃肠病组织的结直肠癌筛查指南均建议对具有该家族史的个体在40岁或比患病亲属诊断年龄提前10年开始筛查[28],仅采用结肠镜作为筛查方式,建议筛查周期为5年或5~10年,我国中华医学会消化病学分会[24]与美国胃肠内镜学会[13]则建议结肠镜筛查周期缩短到3~5年。对于一级亲属在60岁及以上患结直肠癌的情况,美国[9, 11, 14]、加拿大[17]、世界胃肠病组织[28]在所发布的指南中建议将筛查的起始年龄提前到40岁;对于筛查方式的推荐与其对一般风险人群的筛查意见保持一致,如采用包括免疫法粪便潜血试验(FIT)、结肠镜等多种筛查方式。
对于≥2例一级亲属患病的家族史情况,多数指南未界定患病亲属的年龄切点值,其推荐意见通常同有1例60岁前患病的一级亲属家族史的意见一致[9, 11, 14-15, 17, 22, 25-26, 28]。仅英国在其发布的指南中专门界定了以50岁或60岁作为该家族史风险分层的切点值[18]。
对于涉及一、二级亲属均患病的家族史情况,仅有英国家族癌症研究小组[19]与澳大利亚[27]在所发布的指南中给出了相应推荐意见,其中英国家族癌症研究小组建议对个体进行随访检查以评估其发病风险进而采用不同的筛查方案[19]。
对于涉及二、三级亲属家族史的现行指南(如美国[9, 13-14]、加拿大[16-17]、英国[19]、中国[24]、澳大利亚[27]、世界胃肠病组织[28]),均未对患病亲属诊断年龄的切点值进行详细界定,只对患病亲属的数量给出了相应划定。具体来说,对于1例二级或三级亲属患病的家族史情况,美国[9, 13-14],加拿大[16-17],世界胃肠病组织[28]的结直肠癌筛查指南均建议从50岁开始筛查,采用包括结肠镜在内的多种筛查方式。对于≥2例二级或三级亲属患病的家族史情况,美国胃肠病协会[14]、加拿大[17]与世界胃肠病组织[28]在所发布的指南中建议将筛查起始年龄提前到40岁,筛查方式与其对一般风险人群的筛查意见保持一致,然而我国中华医学会消化病学分会建议从50岁开始筛查,仅采用结肠镜作为筛查方式[24]。
我国国家癌症中心于2020年发表的指南中仅推荐具有多于1例一级亲属患结直肠癌家族史的人群在40岁或比一级亲属中最年轻的患者诊断年龄提前10年进行筛查[21],对于其他家族史风险分层的类别未给出筛查推荐意见。我国中华医学会消化病学分会于2011年发布的指南中指出,针对具有1例≥60岁或≥2例一级亲属患结直肠癌的家族史人群应从50岁开始,每5年进行一次结肠镜筛查[24]。
讨论本研究采用系统综述的方法对全球结直肠癌筛查指南中针对具有结直肠癌家族史高危人群的筛查推荐意见进行回顾分析。目前大部分结直肠癌筛查指南仅涉及一般风险人群,针对家族史高危人群的筛查指南和相关推荐相对较少。纳入的20部指南文件中,均为针对非遗传性结直肠癌家族史高危人群的筛查推荐意见,排除包括林奇综合征或家族性腺瘤病等高外显遗传性结直肠癌综合征的意见。
个体的结直肠癌发病风险取决于患病亲属关系等级、患病亲属的诊断年龄、数量以及个体的年龄[7]。目前多数现行的高危人群筛查指南均将结直肠癌家族史作为风险分层的因素,建议对具有家族史的个体进行更早和更频繁的监测,特别是涉及多个一级患病亲属或有年轻患病亲属的情况。一项Meta分析研究表明,与无结直肠癌家族史的人群相比,具有一级亲属结直肠癌家族史的个体发生结直肠癌的风险增加了约2倍[29]。
在全球现行结直肠癌家族史高危人群筛查指南中,涉及二级亲属与三级亲属家族史的筛查建议与一般风险人群保持一致,有研究表明,二级或三级亲属的结直肠癌家族史没有显著增加个体结直肠癌的发病风险[30]。类似的还有,大部分指南对于≥2例一级亲属家族史的推荐意见与1例一级亲属早发性结直肠癌家族史的推荐意见一致,表明基于这两种家族史分层的结直肠癌发病风险相近[6]。此外,对于一级亲属和二级亲属均患病的家族史情况,有研究表明,1例二级亲属和1例一级亲属(或是另1例二级亲属)的家族史组合,其发病风险也显著增加[6]。然而,目前将这种家族史分类纳入推荐的指南较少,仅有英国[19]和澳大利亚[27]给出了相应的推荐意见。
尽管多数指南对于家族史中亲属关系等级给出了明确分类,但只界定了一级亲属诊断年龄的切点值。在美国[9, 11, 13-15]、加拿大[17]、中国[22, 24-25]、新加坡[26]、世界胃肠病组织[28]各机构发布的指南中均将一级患病亲属诊断年龄60岁作为家族史风险分层的年龄切点值。研究表明,一级亲属患结直肠癌的家族史情况会增加个体罹患结直肠癌的风险[29],而且个体的结直肠癌发病风险与一级亲属确诊年龄之间的关系呈S形,风险下降拐点在60岁[31]。值得注意的是,虽然对于有 < 60岁和≥60岁一级患病亲属家族史的个体,指南推荐的筛查起始年龄一致,但建议的结肠镜筛查周期不同(分别为5年和10年)。
对于有结直肠癌家族史的高危人群筛查起始年龄的推荐,现行指南中常采用40岁或比患病亲属中最年轻的患者诊断年龄提前10年开始筛查,一方面可能是为了减少漏诊率,以降低由于漏诊而产生的疾病后果。比如,在美国犹他州的研究中,在40岁的个体中开始筛查,结直肠癌漏诊率较低,仅为3%[32]。另一方面,也可能是由于先前研究证据表明有结直肠癌家族史的人群在35~40岁时发生结直肠癌的风险与一般风险人群在50岁筛查时的发病风险相似[33]。
针对筛查方式的选择,结肠镜作为结直肠癌诊断的金标准,是其他筛查试验阳性的最终途径,也是有结直肠癌家族史的人群最合适的筛查方式。由于结肠镜检查的高敏感性和较好的卫生经济学效果[16],多数针对家族史人群的筛查意见均建议采用结肠镜进行筛查,而且个体在结肠镜检查阴性结果后,可以间隔相对较长时间(如5~10年)再次进行检查[34]。
对结直肠癌家族史高危人群进行针对性筛查有利于降低结直肠癌发病率与死亡率,而且与无家族史的人相比,个体依从性更好,但目前我国针对家族史分类的结直肠癌筛查方案的实施还未广泛开展,需要结合我国实际情况,参考已有的循证指南,制定高质量的结直肠癌高危人群筛查指南,完善我国结直肠癌早诊早治实践。
利益冲突 所有作者声明无利益冲突
作者贡献声明 苏宇:直接参与、收集并分析数据、文章撰写;湛浩然:直接参与、收集并分析数据、文章审阅;孙鑫、陈茹、孙丽、郝金娟:文章审阅、支持性贡献;张效鹏:直接参与、研究指导、文章审阅、工作支持;田雨:直接参与、研究指导、文章审阅、论文修改、工作支持;陈瑞:研究指导、文章审阅、工作支持
| [1] |
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. DOI:10.3322/caac.21660 |
| [2] |
Zheng RS, Zhang SW, Zeng HM, et al. Cancer incidence and mortality in China, 2016[J]. J Natl Cancer Cent, 2022, 2(1): 1-9. DOI:10.1016/j.jncc.2022.02.002 |
| [3] |
Jin P, Wu ZT, Li SR, et al. Colorectal cancer screening with fecal occult blood test: A 22-year cohort study[J]. Oncol Lett, 2013, 6(2): 576-582. DOI:10.3892/ol.2013.1402 |
| [4] |
Brenner H, Stock C, Hoffmeister M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: systematic review and meta-analysis of randomised controlled trials and observational studies[J]. BMJ, 2014, 348: g2467. DOI:10.1136/bmj.g2467 |
| [5] |
Gong YM, Peng P, Bao PP, et al. The implementation and first-round results of a community-based colorectal cancer screening program in Shanghai, China[J]. Oncologist, 2018, 23(8): 928-935. DOI:10.1634/theoncologist.2017-0451 |
| [6] |
Tian Y, Kharazmi E, Sundquist K, et al. Familial colorectal cancer risk in half siblings and siblings: nationwide cohort study[J]. BMJ, 2019, 364: 1803. DOI:10.1136/bmj.l803 |
| [7] |
Tian Y, Kharazmi E, Brenner H, et al. Calculating the starting age for screening in relatives of patients with colorectal cancer based on data from large nationwide data sets[J]. Gastroenterology, 2020, 159(1): 159-168.e3. DOI:10.1053/j.gastro.2020.03.063 |
| [8] |
Tian Y, Kharazmi E, Brenner H, et al. Importance of family history of colorectal carcinoma in situ versus invasive colorectal cancer: a nationwide cohort study[J]. J Natl Compr Canc Netw, 2021, 19(11): 1252-1257. DOI:10.6004/jnccn.2021.7004 |
| [9] |
Shaukat A, Kahi CJ, Burke CA, et al. ACG clinical guidelines: colorectal cancer screening 2021[J]. Am J Gastroenterol, 2021, 116(3): 458-479. DOI:10.14309/ajg.0000000000001122 |
| [10] |
Provenzale D, Ness RM, Llor X, et al. NCCN guidelines insights: colorectal cancer screening, version 2.2020[J]. J Natl Compr Canc Netw, 2020, 18(10): 1312-1320. DOI:10.6004/jnccn.2020.0048 |
| [11] |
Rex DK, Boland RC, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U. S. multi-society task force on colorectal cancer[J]. Am J Gastroenterol, 2017, 112(7): 1016-1030. DOI:10.1038/ajg.2017.174 |
| [12] |
Qaseem A, Denberg TD, Hopkins Jr RH, et al. Screening for colorectal cancer: a guidance statement from the American College of Physicians[J]. Ann Inter Med, 2012, 156(5): 378-386. DOI:10.7326/0003-4819-156-5-201203060-00010 |
| [13] |
Davila RE, Rajan E, Baron TH. ASGE guideline: colorectal cancer screening and surveillance[J]. Gastrointest Endosc, 2006, 63(4): 546-557. DOI:10.1016/j.gie.2006.02.002 |
| [14] |
Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale-Update based on new evidence[J]. Gastroenterology, 2003, 124(2): 544-560. DOI:10.1053/gast.2003.50044 |
| [15] |
Smith RA, Cokkinides V, Eyre HJ. American Cancer Society guidelines for the early detection of cancer, 2003[J]. CA Cancer J Clin, 2003, 53(1): 27-43. DOI:10.3322/canjclin.53.1.27 |
| [16] |
Leddin D, Lieberman DA, Tse F, et al. Clinical practice guideline on screening for colorectal cancer in individuals with a family history of nonhereditary colorectal cancer or adenoma: the Canadian association of gastroenterology Banff consensus[J]. Gastroenterology, 2018, 155(5): 1325-1347.e3. DOI:10.1053/j.gastro.2018.08.017 |
| [17] |
Leddin D, Hunt R, Champion M, et al. Canadian association of gastroenterology and the Canadian digestive health foundation: guidelines on colon cancer screening[J]. Can J Gastroenterol, 2004, 18(2): 93-99. DOI:10.1155/2004/983459 |
| [18] |
Cairns SR, Scholefield JH, Steele RJ, et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002)[J]. Gut, 2010, 59(5): 666-689. DOI:10.1136/gut.2009.179804 |
| [19] |
Hodgson SV, Bishop DT, Dunlop MG, et al. Suggested screening guidelines for familial colorectal cancer[J]. J Med Screen, 1995, 2(1): 45-51. DOI:10.1177/096914139500200112 |
| [20] |
Sung JJY, Ng SC, Chan FKL, et al. An updated Asia pacific consensus recommendations on colorectal cancer screening[J]. Gut, 2015, 64(1): 121-132. DOI:10.1136/gutjnl-2013-306503 |
| [21] |
国家癌症中心中国结直肠癌筛查与早诊早治指南制定专家组. 中国结直肠癌筛查与早诊早治指南(2020, 北京)[J]. 中华肿瘤杂志, 2021, 43(1): 16-38. National Cancer Center, China, Expert Group of the Development of China Guidelines for the Screening, Early Diagnosis and Treatment of Colorectal Cancer. China guideline for the screening, early detection and early treatment of colorectal cancer (2020, Beijing)[J]. Chin J Oncol, 2021, 43(1): 16-38. DOI:10.3760/cma.j.cn112152-20210105-00010 |
| [22] |
中华医学会肿瘤学分会早诊早治学组. 中国结直肠癌早诊早治专家共识[J]. 中华医学杂志, 2020, 100(22): 1691-1698. Early Diagnosis and Early Treatment Group, BranchOncology, Chinese Medical Association. Expert consensus on early diagnosis and treatment of colorectal cancer in China[J]. Natl Med J China, 2020, 100(22): 1691-1698. DOI:10.3760/cma.j.cn112137-20190924-02103 |
| [23] |
中华医学会消化内镜学分会消化系早癌内镜诊断与治疗协作组, 中华医学会消化病学分会消化道肿瘤协作组, 中华医学会消化内镜学分会肠道学组, 等. 中国早期结直肠癌及癌前病变筛查与诊治共识[J]. 中国实用内科杂志, 2015, 35(3): 211-227. The Cooperative Group for Endoscopic Diagnosis and Treatment of Early Cancer in the Digestive System of the Digestive Endoscopy Branch of the Chinese Medical Association, the Cooperative Group for Gastrointestinal Tumors of the Digestive Endoscopy Branch of the Chinese Medical Association, the Enterology Group of the Digestive Endoscopy Branch of the Chinese Medical Association, et al. Chinese consensus: screening, diagnosis and treatment of early colorectal cancer and precancerous lesions[J]. Chin J Pract Inter Med, 2015, 35(3): 211-227. DOI:10.7504/nk2015020301 |
| [24] |
中华医学会消化病学分会. 中国大肠肿瘤筛查、早诊早治和综合预防共识意见[J]. 胃肠病学和肝病学杂志, 2011, 20(11): 979-995. Digestive Branch of Chinese Medical Association. Consensus on Screening, Early Diagnosis, Early Treatment and Comprehensive Prevention of Colorectal Cancer in China[J]. Chin J Gastroenterol Hepatol, 2011, 20(11): 979-995. DOI:10.3969/j.issn.1006-5709.2011.11.001 |
| [25] |
Lam TH, Wong KH, Chan KK, et al. Recommendations on prevention and screening for colorectal cancer in Hong Kong[J]. Hong Kong Med J, 2018, 24(5): 521-526. DOI:10.12809/hkmj177095 |
| [26] |
Ministry of Health, Singapore Government. Cancer Screening: MOH Clinical Practice Guidelines 1/2010[EB/OL]. [2022-05-24]. http://www.moh.gov.sg/cpg.
|
| [27] |
National Health and Medical Research Council. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer[EB/OL]. [2022-05-24]. https://wiki.cancer.org.au/australia/Guidelines:Colorectal_ cancer.
|
| [28] |
World Gastroenterology Organisation. WGO Practice Guideline-Colorectal Cancer Screening[EB/OL]. [2021-05-24]. https://www.worldgastroenterology.org/guidelines/global-guidelines/colorectal-cancer-screening.
|
| [29] |
Butterworth AS, Higgins JPT, Pharoah P. Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis[J]. Eur J Cancer, 2006, 42(2): 216-227. DOI:10.1016/j.ejca.2005.09.023 |
| [30] |
Taylor DP, Burt RW, Williams MS, et al. Population-based family history-specific risks for colorectal cancer: a constellation approach[J]. Gastroenterology, 2010, 138(3): 877-885. DOI:10.1053/j.gastro.2009.11.044 |
| [31] |
Samadder NJ, Smith KR, Hanson H, et al. Increased risk of colorectal cancer among family members of all ages, regardless of age of index case at diagnosis[J]. Clin Gastroenterol Hepatol, 2015, 13(13): 2305-2311.e2. DOI:10.1016/j.cgh.2015.06.040 |
| [32] |
Samadder NJ, Curtin K, Tuohy TM, et al. Increased risk of colorectal neoplasia among family members of patients with colorectal cancer: a population-based study in Utah[J]. Gastroenterology, 2014, 147(4): 814-821.e5. DOI:10.1053/j.gastro.2014.07.006 |
| [33] |
Fuchs CS, Giovannucci EL, Colditz GA, et al. A prospective study of family history and the risk of colorectal cancer[J]. N Engl J Med, 1994, 331(25): 1669-1674. DOI:10.1056/NEJM199412223312501 |
| [34] |
Brenner H, Chang-Claude J, Seiler CM, et al. Long-term risk of colorectal cancer after negative colonoscopy[J]. J Clin Oncol, 2011, 29(28): 3761-3767. DOI:10.1200/JCO.2011.35.9307 |