 2022, Vol. 43
2022, Vol. 43文章信息
- 石菊芳, 曹梦迪, 严鑫鑫, 曹毛毛, 王宇婷, 李燕婕, 王鑫, 李纪宾, 李霓, 曲春枫, 陈万青.
- Shi Jufang, Cao Mengdi, Yan Xinxin, Cao Maomao, Wang Yuting, Li Yanjie, Wang Xin, Li Jibin, Li Ni, Qu Chunfeng, Chen Wanqing
- 肝癌筛查在我国人群中的可及性:一项探索性分析
- Access to liver cancer screening and surveillance in populations in China: an exploratory analysis
- 中华流行病学杂志, 2022, 43(6): 906-914
- Chinese Journal of Epidemiology, 2022, 43(6): 906-914
- http://dx.doi.org/10.3760/cma.j.cn112338-20211112-00879
-
文章历史
收稿日期: 2021-11-12




2. 国家癌症中心/国家肿瘤临床医学研究中心/中国医学科学院北京协和医学院肿瘤医院分子肿瘤学国家重点实验室/免疫学研究室, 北京 100021
2. State Key Laboratory of Molecular Oncology and Department of Immunology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China
卫生服务可及性在国际范围内日益受到关注[1-2],而可获得性(availability)是其重要组成部分。该概念广泛应用于卫生政策评价领域,为卫生决策提供支持。WHO国际癌症研究署(International Agency for Research on Cancer,IARC)在系列癌症筛查手册中,将可获得性列为筛查技术方案和效果综合评估的重要指标之一,具体主要涉及当地有无相关筛查/监测政策、现有筛查/监测方案、人群覆盖率、筛查参与率和依从率及其影响因素、治疗率、公平性等[3-4]。此外,IARC癌症筛查手册的评价也涉及到可接受度指标(acceptability)。上述指标在我国人群癌症二级预防评价领域存在部分报道,但结果分散。
筛查和监测是癌症二级预防的重要途径。筛查是在一定年龄段的普通人群中开展,针对临床前期或早期疾病阶段,运用快速简便的方法,将未察觉或未诊断的表面健康的人群中那些可能有病的个体,同那些可能无病者鉴别开来的系列医疗卫生服务措施[5]。癌症监测(surveillance)的概念在近几年被更多提及,其要点是针对癌症高危人群,提供连续、系统、纵向的检查[6],以发现早期癌症并进行干预;因生存率低等原因,肝癌较乳腺癌、结直肠癌等其他常见癌种会更多提及监测的概念。此处的高危人群概念为泛指,肝癌的高危人群多指慢性HBV/HCV感染者、有家族史者等,而不同项目/研究间会有具体参考危险因素(年龄因素除外)或筛查技术及结果判定等方面的差异。
肝癌在我国人群中的疾病负担和经济负担重[7-8],客观上需要更高的预防诊治服务可及性。本研究以肝癌的筛查与监测为切入点,围绕IARC使用的具体指标,探索性进行信息检索、整合,初步分析肝癌筛查服务可及性在我国人群中的总体可及性以及各细化指标信息可获得情况和量化值。
资料与方法1. 概述:主要基于文献库的系统综述,辅以核心文献、相关官方网站、方案报告等信息渠道,对我国人群开展肝癌筛查相关指标进行系统整合评估分析。
2. 基于文献库的系统综述:
(1)检索式:①检索文献库包括PubMed、Embase、中国知网和万方数据知识服务平台,检索时间均为建库至2021年10月31日。筛查部分中文检索主题词主要包括“肝癌”“肝肿瘤”以及“筛查”“早诊早治”等,对应英文检索以主题词结合自由词的方式,包括“liver neoplasms”“liver tumor”“hepatocellular carcinoma”“liver cancer”“mass screening”“early diagnosis”“early detection of cancer”“screening”。②筛查相关指标检索:进一步结合可获得性相关主题词如“可及性”“可获得性”“覆盖率”“参与率”“筛查率”“顺应性”“依从率”“接受度”“公平性”等;英文包括“access”“availability”“adherence”“participat*”“equity”“acceptance”等。③监测相关指标检索:基于①检索式,进一步嵌入了肝癌高危人群/监测等限定,如“高危”“population surveillance”“surveillance”“high-risk”等。
(2)文献纳入排除标准:①纳入标准:已公开发表的原始研究、期刊论文、研究对象为我国人群、语言为中文或英文;②排除标准:无关肝癌筛查可获得性或肝癌监测报道、无对应指标报道、重复报道等。
3. 信息摘录时对筛查与监测区别判断:目前国内肝癌二级预防领域文献或项目方案的表达多为广义的筛查(包括狭义的筛查以及后续的监测/随访)。《原发性肝癌的分层筛查与监测指南(2020版)》对监测的定义是连续、系统、随时间纵向推移、定期对高危人群进行检查[9],国内近两年的另两部肝癌共识规范中未见对肝癌监测的具体定义[10-11]。美国、欧洲地区的癌症或肝癌相关协会指南对肝癌监测的作用、宏观概念有不同程度描述(如监测的一般概念和作用等)[12-14],但对肝癌筛查和监测在流程上的具体区别定义未见。为更准确归类,本研究基于具体项目/研究中采用的筛查及阳性管理/随访流程进行判断:若是对高危人群在一个筛查轮次之后开展或推荐的进一步规律性检查,则判定为“监测”方案。
4. 评价指标及其计算:覆盖率(初筛人数÷我国总人口中对应年份和年龄范围的人数×100%)、筛查参与率(参加复筛人数÷初筛阳性人数×100%)、监测依从率(参加监测人数÷复筛阳性需监测人数×100%)、肝癌治疗率(确诊肝癌者实际接受治疗的百分比)。见图 1。

|
| 图 1 基于肝癌干预流程的评价指标示意图 |
1. 一般情况:系统文献检索初筛,肝癌筛查和监测分别检出文献189篇和1 261篇,库间去重、阅读题目和摘要后排除、补充文献后(图 2),最终纳入34篇文献,其中筛查参与率相关27篇(含覆盖率相关1篇),监测依从率相关6篇,筛查接受度相关1篇。更多指标信息来自核心文献/论著、官网、方案报告等渠道。

|
| 图 2 文献检索流程及筛选结果(截至2021年10月31日) |
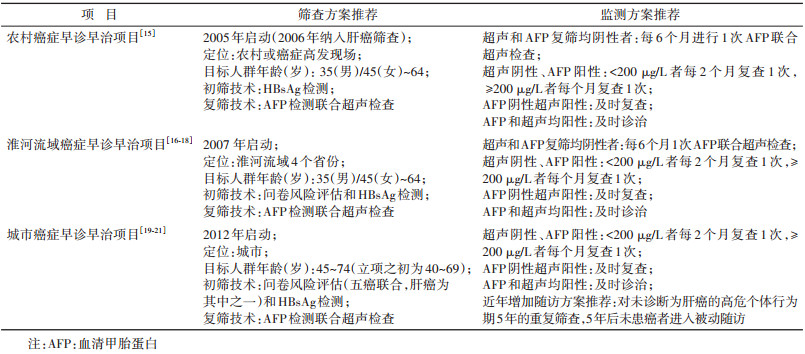
2. 相关政策及现行方案:我国目前中央财政支持的3项癌症筛查公共卫生服务项目,即农村癌症早诊早治项目(农癌项目)[15]、淮河流域癌症早诊早治项目(淮河流域项目)[16-18]和城市癌症早诊早治项目(城癌项目)[19-21],均在特定地区和年龄段的一般人群中进行肝癌筛查实践及相关评价,并且也针对筛查发现不同程度的高危人群有监测方案的推荐,基本以单独HBsAg检测或结合问卷风险评估为初筛,以血清甲胎蛋白(AFP)检测联合腹部超声检查作为复筛,具体各项目见表 1[15-21]。国家卫生健康委员会发布《原发性肝癌诊疗规范(2019年版)》的筛查诊断相关章节指出,借助肝脏超声检查和AFP进行肝癌早期筛查,建议高危人群至少每隔6个月进行1次检查[11]。也有部分地方性肝癌筛查项目、科研探索以及学术社团推荐的肝癌筛查和监测指南推荐。
3. 筛查覆盖率:主要指肝癌筛查(若为串联筛查方案,则指初筛)的人群覆盖率,需明确接受初筛的人数及对应年龄段人口数。①农癌项目:截至2019/2020年,已覆盖8个省份19个肝癌筛查项目现场,2019年新入队列初筛人数为1.8万[22]。需要补充说明的是,该数字要少于早期新入队列初筛人数(如,2012/2013年初筛人数为7.2万),因农癌项目各现场每年的总任务量包括两部分——新入队列人数和逐年累计需随访人数,而总任务量每年基本保持不变;此外,总项目早期在逐渐新增项目点,近年经费投入稳定未新增。②淮河流域项目:累计覆盖4个省份13个肝癌筛查项目现场,2010-2016年年均接受初筛人数为14.5万人[23],近年(包括2019年)每年初筛人数变化不大。③城癌项目:累计覆盖29个省份,累计风险评估人数445.2万,2019年约为45.7万人[24]。综上估算,我国三大公卫项目2019年肝癌筛查覆盖人数为62.0万,因而在全国35~74岁人群中(72 985万,2019年值[25])的覆盖率约为0.09%。针对肝癌的个体机会性筛查和单位组织体检等运行形式暂无信息支持。
4. 筛查参与率及影响因素:本研究所提筛查参与率特指实际参加复筛人数占初筛阳性人数的百分比,在部分研究报告中表示为依从率。三大公卫项目中的农癌项目,未明确报道整体HBsAg初筛阳性者的复筛率;通过系统文献检出的1项研究是农癌项目的肝癌筛查现场所在市(广东省中山市),报道2 822名HBsAg初筛阳性者进一步接受超声筛查参与率为62.3%[26]。三大公卫项目中的城癌项目,2013-2017年整体累计报道筛查参与率为37.5%[27];系统文献检索检出源自该国家级项目的散在省(市)级分析22篇[28-49],报道筛查参与率M(Q1,Q3)为42.5%(36.0%,52.1%),最小值和最大值分别为7.1%和71.1%。仅有的1篇影响因素报道提示,有相关肝病史和肝癌家族史者、女性、文化程度高、吸烟饮酒者等特征人群的筛查参与率更高[45]。三大公卫项目中的淮河项目,2010-2016年整体报道筛查参与率为57.9%(完成临床筛查人数为11.3万,问卷风险评估阳性人数为19.5万)[23];各省间筛查参与率存在差异,通过文献检出的2篇地方性报道分别为86.3%(江苏省,2013-2017年,2.1万人)[50]和60.6%(安徽省,2015-2018年,4.6万人)[51]。
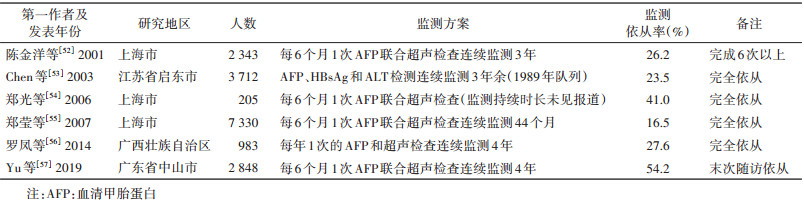
5. 监测依从率及影响因素:监测依从率一般指实际按推荐方案接受监测的高危个体人数占应监测人数的百分比。该指标系统综述共纳入6篇文献[52-57],依从率M(Q1,Q3)为26.9%(23.5%,41.0%),最小值和最大值分别为16.5%和54.2%。见表 2。上述三大公卫项目未见监测依从率及影响因素报道。上述6篇中仅1篇报道了影响因素,结果提示医务人员督促对监测依从率有显著影响(OR=17.8,95%CI:3.41~91.1)[54]。
6. 肝癌治疗率:为实际治疗例数占应治疗例数的百分比,三大项目中仅农癌项目常规分析报道肝癌治疗率,经过筛查监测发现并进一步诊断的肝癌患者治疗率在90%以上[22]。
7. 接受度:城癌项目癌症筛查可持续性评估报告提示,2012-2014年13个省份2 963名肝癌高危个体对AFP检测联合超声筛查技术的主观接受度为99.3%,其中完全可接受比例为92.1%[58-59]。系统综述检出肝癌筛查接受度且报道了具体率值的文献仅1篇,为上述城癌项目多中心分析的单点信息(北京市:88.5%)[60]。系统综述未检出肝癌监测接受度相关文献。更广义的接受度概念,如满意度、偏好等内容未检出。
8. 公平性:该概念应用到癌症防控领域,主要指无论个人特征如何,都可确保其获得癌症筛查及相关诊治[3],但通过系统综述未检出我国人群肝癌筛查及监测相关公平性研究,提示需得到更多关注。
讨论本研究探索性汇总量化了肝癌二级预防的筛查和监测服务在我国人群中的可及性,尤其是可获得性系列指标,整体而言证据仍然有限。通过对现有信息的整合分析提示,我国人群肝癌筛查和监测服务的整体可获得性的提升空间仍然较大,主要体现在当前覆盖率较低。其中筛查参与率和监测依从率存在项目和人群研究间差异,需更多影响因素探索;较高的主观接受度提示潜在的客观需求,治疗率较高但细化信息有限,提示需更多关注;未见公平性报道。
肝癌作为我国人群癌谱中的重要癌种之一,一直备受关注[61]。因肝癌进展迅速,发现往往已是晚期,如何在极其有限的时间内筛查出早期肝癌以及时有效治疗目前仍是挑战。本次汇总分析也提示我国在十几年前就制定了肝癌筛查监测和早诊早治相关方案并在全国的重点农村地区开始探索,后来逐渐扩大目标人群和覆盖范围,相关实践为我国人群的肝癌二级预防积累了重要的现场经验。
相比筛查技术更成熟的癌种,如纳入两癌筛查和基本公共卫生服务的子宫颈癌和乳腺癌筛查,据全国第六次卫生服务统计调查报告显示,2018年对应人群覆盖率(20~64岁)分别是26.8%和28.3%[62]。本分析提示目前我国肝癌筛查项目的适龄人群年度覆盖率约为0.09%,可能与肝癌筛查技术一直处于探索行进而未大范围推广[63-64]以及在高危人群中开展更经济有效[65]等原因有关。当然,若将个体机会性筛查、单位组织体检等其他形式考虑在内,实际接受肝癌筛查服务的人群比例会更高。此外,实际人群当前较低的肝癌筛查覆盖率与较高的主观接受度并存的情况,提示着人群对筛查服务的需求。
本研究结果提示,筛查参与率存在项目人群间差异,可能与初筛方案及项目运作模式、项目开展时长对当地居民健康意识的影响、当地医疗经济水平等因素有关。城癌项目开展了相关影响因素研究,提示了可重点干预亚组人群以提高筛查参与率。针对高危人群的监测依从率数据整体更低也更稳定(约1/4),提示要按时完成监测,无论对高危个体还是监测工作人员都是难点,且普遍存在;相关影响因素方面,文献提示服务提供方的督促可有效提高监测依从率,但具体哪类革新技术、措施、管理模式可有效提高依从性,哪类服务接受方需要且可以重点干预,类似信息依然匮乏。
人群筛查效果与后续的监测早诊早治密不可分,个体的筛而不诊或诊而不治都将弱化人群筛查效力。与WHO消除子宫颈癌的疫苗-筛查-治疗三大环节有共通之处,通过筛查监测发现确诊的肝癌病例,其治疗率进一步决定干预的人群效果,而农村地区的实践报道了可喜的治疗率数据,一定程度反映了早期治疗服务较高的可获得性;当然,如有不同治疗方案(如仅采用中药治疗的姑息治疗等)的详尽信息,将会指引更具体的治疗服务利用分析;同时,未治疗的原因,除医疗资源的可获得性外,也可能是受到具体家庭个人的经济条件、观念、价值取向等影响。
可及性概念下的细化指标提示着不同的实践方向,覆盖率和公平性主要决定于服务提供方的资源配置,筛查参与率、监测依从率、治疗率、接受度等指标更多决定于服务提供方的筛查干预技术组织流程、服务接受方的知信行等。希望看到肝癌整个筛查监测干预链条上,针对各环节的更多报道和影响因素深入分析,切实指导优化从初筛-复筛-监测-诊治全链条过程中,组织机构项目管理角度的可操作性、人群对不同环节干预重要性的认知和参与等问题。
本次系统检索可能存在文献漏检。对监测的执行定义与部分报道可能存在区别,也希望该概念在肝癌二级预防领域中有更明确的公认的执行定义。本次探索性分析关注的细化指标选择,主要参照IARC系列癌症筛查手册(包括主观接受度);但在更广义的理论框架方面,卫生服务可及性的概念自半个世纪前被明确提出后,不断发展深化并延展到诸多领域,涵盖细化指标在不同模型和研究间既有共性也存在差别[66-69]。将来可考虑制定更全面且适合我国人群的癌症筛查可及性评价指标体系,就肝癌等常见癌种的筛查服务可及性进行全面量化,为癌症防控相关卫生决策提供参考。
利益冲突 所有作者声明无利益冲突
作者贡献声明 石菊芳:研究设计、论文撰写、经费支持;曹梦迪、严鑫鑫:文献检索、数据整理分析;曹毛毛、王宇婷、李燕婕、王鑫:信息核查;李纪宾、李霓、曲春枫:文稿审阅;陈万青:研究设计、论文审阅、经费支持
| [1] |
GBD 2016 Healthcare Access and Quality Collaborators. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: a systematic analysis from the Global Burden of Disease Study 2016[J]. Lancet, 2018, 391(10136): 2236-2271. DOI:10.1016/S0140-6736(18)30994-2 |
| [2] |
Sirohi B, Mathew A. Access to and affordability of cancer medicines: time to focus on the last mile[J]. Lancet Oncol, 2021, 22(10): 1342-1343. DOI:10.1016/S1470-2045(21)00518-0 |
| [3] |
IARC (2016). Breast cancer screening. IARC handbooks of cancer prevention[EB/OL]. [2021-10-06]. https://publications.iarc.fr/Book-And-Report-Series/Iarc-Handbooks-Of-Cancer-Prevention/Breast-Cancer-Screening-2016.
|
| [4] |
IARC (2019). Colorectal cancer screening. IARC handbooks of cancer prevention[EB/OL]. [2021-10-06]. https://publications.iarc.fr/Book-And-Report-Series/Iarc-Handbooks-Of-Cancer-Prevention/Colorectal-Cancer-Screening-2019.
|
| [5] |
詹思延. 流行病学[M]. 8版. 北京: 人民卫生出版社, 2017. Zhan SY. Epidemiology[M]. 8th ed. Beijing: People's Medical Publishing House, 2017. |
| [6] |
Zhao CQ, Nguyen MH. Hepatocellular carcinoma screening and surveillance: practice guidelines and real-life practice[J]. J Clin Gastroenterol, 2016, 50(2): 120-133. DOI:10.1097/MCG.0000000000000446 |
| [7] |
Lei HK, Lei L, Shi JF, et al. No expenditure difference among patients with liver cancer at stage Ⅰ-Ⅳ: Findings from a multicenter cross-sectional study in China[J]. Chin J Cancer Res, 2020, 32: 516-529. DOI:10.21147/j.issn.1000-9604.2020.04.09 |
| [8] |
曹梦迪, 王红, 石菊芳, 等. 中国人群肝癌疾病负担: 多数据源证据更新整合分析[J]. 中华流行病学杂志, 2020, 41(11): 1848-1858. Cao MD, Wang H, Shi JF, et al. Disease burden of liver cancer in China: an updated and integrated analysis on multi-data source evidence[J]. Chin J Epidemiol, 2020, 41(11): 1848-1858. DOI:10.3760/cma.j.cn112338-20200306-00271 |
| [9] |
中华预防医学会肝胆胰疾病预防与控制专业委员会, 中国研究型医院学会肝病专业委员会, 中华医学会肝病学分会, 等. 原发性肝癌的分层筛查与监测指南(2020版)[J]. 中华肿瘤杂志, 2021, 43(1): 60-77. Hepatobiliary and Pancreatic Diseases Prevention and Control Professional Committee of Chinese Preventive Medical Association, Hepatology Professional Committee of Chinese Research Hospital Association, Hepatology Branch of Chinese Medical Association, et al. Guideline for stratified screening and surveillance of primary liver cancer (2020 edition)[J]. Chin J Oncol, 2021, 43(1): 60-77. DOI:10.3760/cma.j.cn112152-20201109-00970 |
| [10] |
中华医学会肝病学分会. 原发性肝癌二级预防共识(2021年版)[J]. 中华肝脏病杂志, 2021, 29(3): 216-226. Chinese Society of Hepatology. Consensus on secondary prevention of primary liver cancer (2021 version)[J]. Chin J Hepatol, 2021, 29(3): 216-226. DOI:10.3760/cma.j.cn501113-20210210-00082 |
| [11] |
中华人民共和国国家卫生健康委员会医政医管局. 原发性肝癌诊疗规范(2019年版)[J]. 中华消化外科杂志, 2020, 19(1): 1-20. National Health Commission of the People's Republic of China Medical Administration Hospital Authority. Standardization for diagnosis and treatment of hepatocellular carcinoma (2019 edition)[J]. Chin J Dig Surg, 2020, 19(1): 1-20. DOI:10.3760/cma.j.issn.1673-9752.2020.01.001 |
| [12] |
National Cancer Institute. About the surveillance research program[EB/OL]. [2021-10-13]. https://surveillance.cancer.gov/about/.
|
| [13] |
EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma[J]. J Hepatol, 2018, 69(1): 182-236. DOI: 10.1016/j.jhep.2018.03.019.
|
| [14] |
Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma[J]. Hepatology, 2018, 67(1): 358-380. DOI:10.1002/hep.29086 |
| [15] |
卫生部疾病预防控制局, 癌症早诊早治项目专家委员会. 癌症早诊早治项目技术方案(2011年版)[M]. 北京: 人民卫生出版社, 2011. Bureau of Disease Control and Prevention of the Ministry of Health, Expert Committee of Cancer Early Diagnosis and Early Treatment Project. Technical protocol of early diagnosis and early treatment of cancer program (2011 edition)[M]. Beijing: People's Medical Publishing House, 2011. |
| [16] |
Li J, Li H, Zeng HM, et al. A study protocol of population-based cancer screening cohort study on esophageal, stomach and liver cancer in rural China[J]. Chin J Cancer Res, 2020, 32(4): 540-546. DOI:10.21147/j.issn.1000-9604.2020.04.11 |
| [17] |
Cao MM, Li H, Sun DQ, et al. Cancer screening in China: The current status, challenges, and suggestions[J]. Cancer Lett, 2021, 506: 120-127. DOI:10.1016/j.canlet.2021.02.017 |
| [18] |
国家癌症中心, 中国医学科学院肿瘤医院. 淮河流域癌症早诊早治项目技术方案(2020年修订版). 北京, 2020. National Cancer Center, Cancer Hospital, Chinese Academy of Medical Sciences. Technical protocol for cancer screening program in Huaihe River (2020 revised edition). Beijing, 2020. |
| [19] |
代敏, 石菊芳, 李霓. 中国城市癌症早诊早治项目设计及预期目标[J]. 中华预防医学杂志, 2013, 47(2): 179-182. Dai M, Shi JF, Li N. Design and expected target of early diagnosis and treatment project of urban cancer in China[J]. Chin J Prev Med, 2013, 47(2): 179-182. DOI:10.3760/cma.j.issn.0253-9624.2013.02.018 |
| [20] |
国家癌症中心, 中国医学科学院肿瘤医院. 城市癌症早诊早治项目技术方案(2020年版)[M]. 北京: 国家癌症中心, 2020. National Cancer Center, Cancer Hospital, Chinese Academy of Medical Sciences. Technical protocol for cancer screening program in Urban China (2020 edition)[M]. Beijing: National Cancer Center, 2020. |
| [21] |
赫捷. 中国人群癌症筛查工作指导手册[M]. 北京: 人民卫生出版社, 2021.
|
| [22] |
国家卫生健康委员会疾病预防控制局, 中国癌症基金会, 农村癌症早诊早治项目专家委员会. 癌症早诊早治项目(农村)工作报告2019/2020[R]. 北京, 2020. Bureau of Disease Control and Prevention of the National Health Commission, China Cancer Foundation, Expert Committee of Cancer Screening Program in Rural China. Annual report of the cancer screening program in Rural China, 2019-2020[R]. Beijing, 2020. |
| [23] |
Li J, Li H, Zeng HM, et al. Trends in high-risk rates and screening rates for the population-based cancer screening program on esophageal, stomach and liver cancer in China, 2010-2016[J]. J Natl Cancer Center, 2021, 1(3): 101-107. DOI:10.1016/j.jncc.2021.05.001 |
| [24] |
国家癌症中心, 中国医学科学院肿瘤医院. 城市癌症早诊早治项目工作报告(2020版)[R]. 北京, 2020. National Cancer Center, Cancer Hospital, Chinese Academy of Medical Sciences. Annual Report of the Cancer Screening Program in Urban China (2020 edition)[R]. Beijing, 2020. |
| [25] |
国家统计局. 中国统计年鉴[EB/OL]. [2021-10-03]. http://www.stats.gov.cn/tjsj/ndsj/. The National Bureau of Statistics. China statistical yearbook[EB/OL]. [2021-10-03]. http://www.stats.gov.cn/tjsj/ndsj/. |
| [26] |
俞霞, 程伟民, 吴标华, 等. 中山市小榄镇肝癌高危人群筛查依从性及筛查效果分析[J]. 中国肿瘤临床, 2020, 47(7): 350-353. Yu X, Cheng WM, Wu BH, et al. Compliance and effectiveness of screening in population with high risk for liver cancer in Xiaolan town, Zhongshan city[J]. Chin J Clin Oncol, 2020, 47(7): 350-353. DOI:10.3969/j.issn.1000-8179.2020.07.111 |
| [27] |
陈万青, 李霓, 曹毛毛, 等. 2013-2017年中国城市癌症早诊早治项目基线结果分析[J]. 中国肿瘤, 2020, 29(1): 1-6. Chen WQ, Li N, Cao MM, et al. Preliminary analysis of cancer screening program in urban China from 2013 to 2017[J]. China Cancer, 2020, 29(1): 1-6. DOI:10.11735/j.issn.1004-0242.2020.01.A001 |
| [28] |
李辉章, 杜灵彬, 孙校华, 等. 浙江省城市居民癌症早诊早治项目筛查结果报告[J]. 浙江预防医学, 2015, 27(12): 1189-1193. Li HZ, Du LB, Sun XH, et al. An analysis on the result of early detection and treatment of cancer in Zhejiang urban population[J]. Zhejiang Prev Med, 2015, 27(12): 1189-1193. DOI:10.19485/j.cnki.issn1007-0931.2015.12.001 |
| [29] |
汪雯, 李辉章, 朱陈, 等. 浙江省2014-2015年度居民癌症风险评估及筛查结果分析[J]. 浙江医学, 2016, 38(22): 1795-1798, 1814. Wang W, Li HZ, Zhu C, et al. 2014-2015 cancer risk assessment and screening in urban population of Zhejiang province[J]. Zhejiang Med J, 2016, 38(22): 1795-1798, 1814. |
| [30] |
朱俊宇, 顾秀瑛, 宋述铭, 等. 乌鲁木齐市2015~2016年度城市居民癌症高风险人群筛查分析[J]. 实用肿瘤杂志, 2017, 32(4): 367-370. Zhu JY, Gu XY, Song SM, et al. Analysis of 2015-2016 population screen of high cancer risk urban residents in Urumqi city[J]. J Pract Oncol, 2017, 32(4): 367-370. DOI:10.13267/j.cnki.syzlzz.2017.04.019 |
| [31] |
Xu H, Wang Q. Assessment on cancer risk and analysis on screening results of urban residents in Nantong from 2015 to 2016[J]. Mod Prev Med, 2017, 44(20): 3724-3726, 3752. DOI: 1003-8507(2017)20-3724-04. 徐红, 王秦. 2015-2016年度南通市城市居民癌症风险评估和筛查结果分析[J]. 现代预防医学, 2017, 44(20): 3724-3726, 3752. DOI: 1003-8507(2017)20-3724-04. |
| [32] |
李辉, 龚清海, 孙校华, 等. 宁波市城市居民恶性肿瘤风险评估及临床筛查结果分析[J]. 预防医学, 2017, 29(10): 1024-1026. Li H, Gong QH, Sun XH, et al. Risk assessment and clinical screening results of malignant tumor in Ningbo city[J]. Prev Med, 2017, 29(10): 1024-1026. DOI:10.19485/j.cnki.issn1007-0931.2017.10.013 |
| [33] |
孙高峰, 赵娥, 谢惠芳, 等. 乌鲁木齐市2014年城市癌症早诊早治筛查效果分析[J]. 中国初级卫生保健, 2018, 32(3): 57-60. Sun GF, Zhao E, Xie HF, et al. Analysis on the result of early detection and treatment of cancer in 2014 Urumqi[J]. Chin Primary Health Care, 2018, 32(3): 57-60. DOI:10.3969/j.issn.1001-568X.2018.03.0021 |
| [34] |
张强, 黄云超, 沈丽达, 等. 云南省127 960名城市居民癌症风险评估及筛查结果分析[J]. 中国肿瘤, 2018, 27(9): 641-646. Zhang Q, Huang YC, Shen LD, et al. Analysis of cancer risk assessment and screening results among urban residents in Kunming City[J]. China Cancer, 2018, 27(9): 641-646. DOI:10.11735/j.issn.1004-0242.2018.09.A001 |
| [35] |
龚静, 元国平, 林寅君, 等. 宁波市江北区2013-2017年度居民癌症高风险评估及临床筛查结果分析[J]. 中国公共卫生, 2019, 35(11): 1572-1574. Gong J, Yuan GP, Lin YJ, et al. Outcomes of high risk assessment and clinical screening on cancer among community residents in Jiangbei district of Ningbo city: 2013-2017[J]. Chin J Public Health, 2019, 35(11): 1572-1574. DOI:10.11847/zgggws1119564 |
| [36] |
刘运泳, 左婷婷, 于连政, 等. 沈阳市城市居民癌症风险评估及筛查结果分析[J]. 中国公共卫生, 2020, 36(1): 1-4. Liu YY, Zuo TT, Yu LZ, et al. Analysis of the results on cancer risk assessment and screening of urban residents in Shenyang[J]. Chin J Public Health, 2020, 36(1): 1-4. DOI:10.11847/zgggws1127286 |
| [37] |
于慧会, 任英, 张亮, 等. 2014-2018年辽宁省城市居民肝癌筛查结果分析[J]. 现代预防医学, 2020, 47(5): 913-916. Yu HH, Ren Y, Zhang L, et al. Hepatocellular carcinoma screening among residents, Liaoning province, 2014-2018[J]. Mod Prev Med, 2020, 47(5): 913-916. |
| [38] |
朱战慧, 曹骥, 余家华, 等. 2014-2017年广西城市癌症早诊早治项目癌症风险评估及筛查结果分析[J]. 中国癌症防治杂志, 2020, 12(6): 681-685. Zhu ZH, Cao J, Yu JH, et al. Assessment of cancer risk and analysis of screening results of cancer screening program in urban Guangxi from 2014 to 2017[J]. Chin J Cancer Prev Treat, 2020, 12(6): 681-685. DOI:10.3969/j.issn.1674-5671.2020.06.15 |
| [39] |
容敏华, 葛莲英, 余家华, 等. 2014-2019年广西城市癌症早诊早治项目肝癌筛查和随访结果分析[J]. 中国肿瘤, 2021, 30(5): 328-333. Rong MH, Ge LY, Yu JH, et al. Analysis of liver cancer screening results in Guangxi urban cancer early detection and treatment project, 2014-2019[J]. China Cancer, 2021, 30(5): 328-333. DOI:10.11735/j.issn.1004-0242.2021.05.A002 |
| [40] |
庹吉妤, 张霞, 何晓梅, 等. 湖北省2018-2019年城市癌症早诊早治项目筛查结果分析[J]. 实用肿瘤学杂志, 2021, 35(4): 297-301. Tuo JY, Zhang X, He XM, et al. Analysis of the screening results of the urban cancer early diagnosis and treatment project in Hubei province from 2018 to 2019[J]. J Pract Oncol, 2021, 35(4): 297-301. DOI:10.11904/j.issn.1002-3070.2021.04.002 |
| [41] |
王悠清, 李辉章, 王乐, 等. 2013-2018年浙江省城市癌症早诊早治项目人群肝癌筛查结果及相关因素分析[J]. 中华预防医学杂志, 2021, 55(3): 346-352. Wang YQ, Li HZ, Wang L, et al. Analysis of liver cancer screening results and influencing factors of urban residents in Zhejiang Province from 2013 to 2018[J]. Chin J Prev Med, 2021, 55(3): 346-352. DOI:10.3760/cma.j.cn112150-20200818-01132 |
| [42] |
熊小玲, 魏清风, 任剑, 等. 2018-2019年南昌市城区居民癌症风险评估和筛查结果分析[J]. 实用癌症杂志, 2021, 36(7): 1211-1214. Xiong XL, Wei QF, Ren J, et al. Analysis of cancer risk assessment and screening results of urban residents in Nanchang from 2018 to 2019[J]. Pract J Cancer, 2021, 36(7): 1211-1214. DOI:10.3969/j.issn.1001-5930.20201.07.042 |
| [43] |
于慧会, 左婷婷, 吴颖, 等. 2016-2018年沈阳市城市居民肝癌高危风险评估及筛查效果分析[J]. 中国肿瘤, 2021, 30(4): 286-291. Yu HH, Zuo TT, Wu Y, et al. High-risk assessment and screening of hepatocellular carcinoma in Shenyang, 2016-2018[J]. China Cancer, 2021, 30(4): 286-291. DOI:10.11735/j.issn.1004-0242.2021.04.A007 |
| [44] |
张永贞, 高秋生, 崔王飞, 等. 2014-2018年山西省城市癌症早诊早治项目筛查结果分析[J]. 中国肿瘤, 2021, 30(2): 131-136. Zhang YZ, Gao QS, Cui WF, et al. Analysis of cancer screening program in Shanxi urban area from 2014 to 2018[J]. China Cancer, 2021, 30(2): 131-136. DOI:10.11735/j.issn.1004-0242.2021.02.A005 |
| [45] |
郭兰伟, 张韶凯, 刘曙正, 等. 河南省城市地区肝癌筛查依从性及其影响因素分析[J]. 中华肿瘤杂志, 2021, 43(2): 233-237. Guo LW, Zhang SK, Liu SZ, et al. Compliance rate and impact factor analysis of liver cancer screening in urban areas of Henan province[J]. Chin J Oncol, 2021, 43(2): 233-237. DOI:10.3760/cma.j.cn112152-20200331-00286 |
| [46] |
刘亚洲, 孔蕴馨, 罗小虎, 等. 2014-2016年徐州市城市癌症早诊早治筛查分析[J]. 江苏预防医学, 2018, 29(4): 382-385, 388. Liu YZ, Kong YX, Luo XH, et al. Analysis of early diagnosis and treatment of cancer in urban populations of Xuzhou city from 2014 to 2016[J]. Jiangsu J Prev Med, 2018, 29(4): 382-385, 388. DOI:10.13668/j.issn.1006-9070.2018.04.006 |
| [47] |
赵仁成, 林子棠, 余卫军, 等. 2017-2019年深圳市宝安区40~74岁常住居民五癌风险流行状况分析[J]. 实用肿瘤学杂志, 2020, 34(4): 315-320. Zhao RC, Lin ZT, Yu WJ, et al. Analysis of the prevalence of five cancer risks among permanent residents aged 40-74 years old in Baoan District, Shenzhen, 2017-2019[J]. J Pract Oncol, 2020, 34(4): 315-320. DOI:10.11904/j.issn.1002-3070.2020.04.005 |
| [48] |
肖海帆, 颜仕鹏, 许可葵, 等. 湖南省2012-2018年城市癌症早诊早治项目临床筛查结果初步分析[J]. 中国肿瘤, 2019, 28(11): 807-815. Xiao HF, Yan SP, Xu KK, et al. Analysis of cancer screening program in Changsha urban area from 2012 to 2018[J]. China Cancer, 2019, 28(11): 807-815. DOI:10.11735/j.issn.1004-0242.2019.11.A001 |
| [49] |
梁岭, 雷林, 蔡伟聪, 等. 2017-2019年广东省深圳市城市居民肝癌风险评估及筛查结果分析[J]. 中国肿瘤, 2021, 30(5): 334-339. Liang L, Lei L, Cai WC, et al. Analysis of liver cancer risk assessment and screening results among urban residents in Shenzhen, 2017-2019[J]. China Cancer, 2021, 30(5): 334-339. DOI:10.11735/j.issn.1004-0242.2021.05.A003 |
| [50] |
缪伟刚, 周金意, 韩仁强, 等. 2013-2017年江苏省淮河流域地区早诊早治项目肝癌筛查分析[J]. 中国肿瘤, 2021, 30(7): 511-515. Miao WG, Zhou JY, Han RQ, et al. Analysis of liver cancer screening program in Huai River areas of Jiangsu province from 2013 to 2017[J]. China Cancer, 2021, 30(7): 511-515. DOI:10.11735/j.issn.1004-0242.2021.07.A005 |
| [51] |
查震球, 贾尚春, 陈叶纪, 等. 2015-2018年安徽省癌症早诊早治项目农村地区肝癌筛查分析[J]. 中国肿瘤, 2019, 28(10): 743-748. Zha ZQ, Jia SC, Chen YJ, et al. Results of liver cancer screening in rural areas of Anhui Province from 2015 to 2018[J]. China Cancer, 2019, 28(10): 743-748. DOI:10.11735/j.issn.1004-0242.2019.10.A005 |
| [52] |
陈金洋, 杨秉辉, 周杏元, 等. 社区肝癌高危人群筛查间隔时间的探索[J]. 中国肿瘤, 2001, 10(4): 201-202. Chen JY, Yang BH, Zhou XY, et al. The screening interval of early detection for liver cancer in high risk population in community[J]. China Cancer, 2001, 10(4): 201-202. DOI:10.3969/j.issn.1004-0242.2001.04.006 |
| [53] |
Chen JG, Parkin DM, Chen QG, et al. Screening for liver cancer: results of a randomised controlled trial in Qidong, China[J]. J Med Screen, 2003, 10(4): 204-209. DOI:10.1258/096914103771773320 |
| [54] |
郑光, 张红叶, 倪红伟, 等. 肝癌高危人群二级预防依从性影响因素分析[J]. 中国公共卫生, 2006, 22(12): 1439-1440. Zheng G, Zhang HY, Ni HW, et al. Ananlysis influence factors on of second prevention in patients with liver cancer high risk[J]. Chin J Public Health, 2006, 22(12): 1439-1440. DOI:10.3321/j.issn:1001-0580.2006.12.017 |
| [55] |
郑莹, 朱美英, 程月华, 等. 上海市社区肝癌高危人群早发现干预效果的研究[J]. 肿瘤, 2007, 27(1): 73-77. Zheng Y, Zhu MY, Cheng YH, et al. Effect of early detection intervention on high-risk population of liver cancer in Shanghai[J]. Tumor, 2007, 27(1): 73-77. DOI:10.3781/j.issn.1000-7431.2007.01.019 |
| [56] |
罗凤, 崔英, 岳惠芬, 等. 2011-2013年广西社区肝癌和鼻咽癌联合筛查及追踪分析[J]. 中国当代医药, 2014, 21(15): 171-174. Luo F, Cui Y, Yue HF, et al. The joint screening and tracing analysis of hepatic carcinoma and nasopharyngeal carcinoma in Guangxi communities from 2011 to 2013[J]. China Mod Med, 2014, 21(15): 171-174. |
| [57] |
Yu X, Ji MF, Cheng WM, et al. A retrospective cohort study of nasopharyngeal carcinoma screening and hepatocellular carcinoma screening in Zhongshan city[J]. J Cancer, 2019, 10(8): 1909-1914. DOI:10.7150/jca.27676 |
| [58] |
国家癌症中心, 中国医学科学院肿瘤医院. 城市癌症早诊早治项目卫生经济学评价系列报告之中国城市人群中开展癌症筛查的可持续性评估[R]. 北京, 2017. National Cancer Center, Cancer Hospital, Chinese Academy of Medical Sciences. CanSPUC health economic evaluation report: the sustainability of cancer screening in urban populations in China: a report from the CanSPUC Program[R]. Beijing, 2017. |
| [59] |
雷海科, 董佩, 周琦, 等. 我国城市地区人群癌症筛查需求调查分析[J]. 中华流行病学杂志, 2018, 39(3): 289-294. Lei HK, Dong P, Zhou Q, et al. Potential demand on cancer screening service in urban populations in China: a cross-sectional survey[J]. Chin J Epidemiol, 2018, 39(3): 289-294. DOI:10.3760/cma.j.issn.0254-6450.2018.03.008 |
| [60] |
严晓玲, 毛阿燕, 胡广宇, 等. 北京城市居民癌症筛查接受度分析[J]. 中国公共卫生, 2015, 31(8): 1012-1015. Yan XL, Mao AY, Hu GY, et al. Acceptability of cancer screening among urban residents in Beijing[J]. Chin J Public Health, 2015, 31(8): 1012-1015. DOI:10.11847/zgggws2015-31-08-10 |
| [61] |
Shi JF, Cao MM, Wang YT, et al. Is it possible to halve the incidence of liver cancer in China by 2050?[J]. Int J Cancer, 2021, 148(5): 1051-1065. DOI:10.1002/ijc.33313 |
| [62] |
国家卫生健康委统计信息中心. 2018年全国第六次卫生服务统计调查报告[M]. 北京: 人民卫生出版社, 2021. National Health Commission Statistical Information Center. The sixth national health service statistical survey in 2018[M]. Beijing: People's Medical Publishing House, 2021. |
| [63] |
Yeh YP, Hu TH, Cho PY, et al. Evaluation of abdominal ultrasonography mass screening for hepatocellular carcinoma in Taiwan[J]. Hepatology, 2014, 59(5): 1840-1849. DOI:10.1002/hep.26703 |
| [64] |
Ji MF, Liu ZW, Chang ET, et al. Mass screening for liver cancer: results from a demonstration screening project in Zhongshan City, China[J]. Sci Rep, 2018, 8(1): 12787. DOI:10.1038/s41598-018-31119-9 |
| [65] |
白方舟, 王乐, 王宇婷, 等. 中国肝癌筛查卫生经济学研究的系统评价[J]. 中国循证医学杂志, 2018, 18(5): 442-449. Bai FZ, Wang L, Wang YT, et al. Economic evaluation of liver cancer screening in China: a systematic review[J]. Chin J Evid Based Med, 2018, 18(5): 442-449. DOI:10.7507/1672-2531.201802028 |
| [66] |
Andersen RM. A behavioral model of families' use of health services, Research series No. 25. Chicago: Center for Health Administration Studies, University of Chicago, 1968.
|
| [67] |
Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction[J]. Med Care, 1981, 19(2): 127-140. DOI:10.1097/00005650-198102000-00001 |
| [68] |
Thiede M, Akweongo P, McIntyre D. Exploring the dimensions of access. The economics of health equity[M]. New York: Cambridge University Press, 2007.
|
| [69] |
Fundytus A, Sengar M, Lombe D, et al. Access to cancer medicines deemed essential by oncologists in 82 countries: an international, cross-sectional survey[J]. Lancet Oncol, 2021, 22(10): 1367-1377. DOI:10.1016/S1470-2045(21)00463-0 |