 2022, Vol. 43
2022, Vol. 43文章信息
- 张静, 李秀惠, 李丽, 尚小飞.
- Zhang Jing, Li Xiuhui, Li Li, Shang Xiaofei
- 手足口病病原学和流行病学研究进展
- Etiology and epidemiology of hand, foot and mouth disease in China
- 中华流行病学杂志, 2022, 43(5): 771-783
- Chinese Journal of Epidemiology, 2022, 43(5): 771-783
- http://dx.doi.org/10.3760/cma.j.cn112338-20211012-00788
-
文章历史
收稿日期: 2021-10-12




2. 首都医科大学附属北京佑安医院中西医结合中心,北京 100069
2. Integrated Traditional Chinese and Western Medicine Center, Beijing Youan Hospital of Capital Medical University, Beijing 100069, China
手足口病是由肠道病毒(EV)引起的传染病,可引起手、足、口腔等部位的疱疹,少数患儿可引起无菌性脑膜脑炎、脑干脑炎、神经源性肺水肿、心肌炎等并发症[1]。个别重症患儿病情发展快,救治不及时易导致死亡。引起手足口病的EV主要传播途径为粪-口方式传播,也可通过接触口腔分泌物、水泡液被病毒污染的表面和污染物传播[2]。自1951年在南非首次分离到柯萨奇病毒A组16型(CV-A16)毒株[3]、1957年首次发现CV-A16引起的手足口病暴发[4],及1969年美国首次分离出EV-A71型毒株[5],EV-A71和CV-A16这两种毒株多年来一直是手足口病的主要病原体[6-8]。1997年以来,亚太地区多次暴发EV-A71感染的手足口病[9]。1998年国内首次报道EV-A71 C4亚型毒株,自此该毒株一直在我国流行[10]。1999年在我国深圳市分离到CV-A16 B1a进化分支毒株[3],2013年之前B1a分支一直占有绝对优势[3]。2007年我国山东省临沂市和2008年安徽省阜阳市先后暴发EV-A71(C4a)引起的手足口病[10-11],之后该型毒株在我国广泛传播[12]。2008年芬兰首次报道CV-A6是引起手足口病暴发疫情的新病原[13]。同时,其他EV在手足口病病例中的比例逐渐增多,并引起重症和死亡[14]。本研究综述2008年以来我国手足口病病原学和流行病学研究进展,为手足口病防控工作提供参考依据。
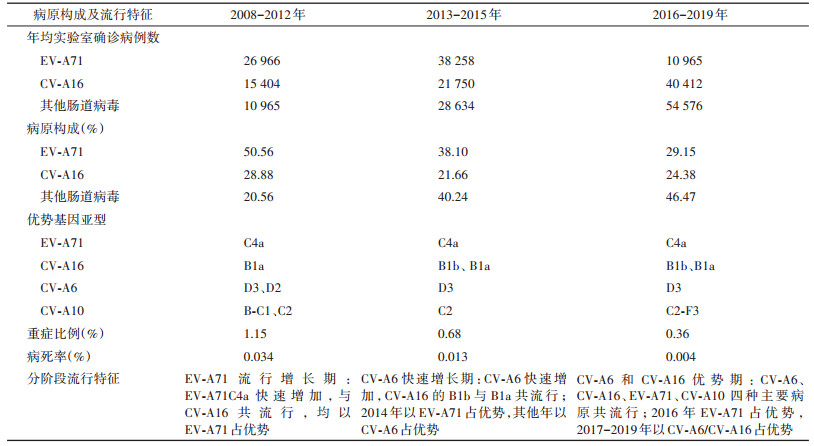
一、病原学1. 手足口病的病原谱:2008-2019年我国手足口病的病原构成发生明显变化。根据EV毒株型别构成的变化和EV-A71疫苗上市后对流行毒株的影响,可将我国手足口病的病原特征划分成三个阶段:2008-2012年EV-A71流行增长期、2013-2015年CV-A6快速增长期和2016-2019年CV-A6/CV-A16优势期(表 1)。2008-2012年手足口病主要是由EV-A71和CV-A16引起全国广泛流行[15-16],2013-2015年手足口病流行毒株构成发生转变,CV-A6、CV-A10、CV-A2等其他EV感染的手足口病散发、暴发逐年增多[17-18],2013年和2015年优势毒株转变为CV-A6。2016年,我国3种EV-A71灭活疫苗均获国家食品药品监督管理局批准上市使用,之后EV-A71感染所致手足口病病例数以及构成比进一步下降[18-19],其他EV的构成比年平均增加16.07%[19],不同地区EV-A71的构成优势也逐渐被CV-A6取代[20-32],CV-A6已成为一种导致手足口病的重要病原[33-34]。从全国手足口病优势病原来看,2008-2012、2014和2016年以EV-A71感染占优势,而在2013、2015、2017、2018和2019年则以其他EV感染占优势[18-19]。CV-A16的占比呈现高-下降-升高,但年均确诊病例数持续增加,从2017-2019年,CV-A16所致手足口病的病例数呈明显上升趋势(表 1),EV占比和确诊例数持续增加,表明有多价疫苗的需求。
手足口病病原谱具有地区和时间上的差异性。2013年广东省等地区出现严重的手足口病流行,优势病原由EV-A71转换为CV-A6,该CV-A6毒株与2011年的CV-A6毒株比对,在P2、P3及3'UTR序列差异较大,部分毒株存在明显基因差异[35-36]。2013-2016年湖南省农村地区手足口病病原检出率依次为CV-A16(29.0%)、CV-A6(28.0%)、EV-A71(17.0%)、CV-A10(4.0%)、CV-A4(2.0%)、CV-A8(1.0%)、CV-A2(1.0%)、CV-A5(0.2%)、EV-B(1.0%)、混合感染(2.0%)、未分型(4.0%)[37]。广州市1 220例实验室确诊手足口病的病原谱包括21种EV:CV-A6(29.8%)、CV-A10(25.0%)、CV-A16(32.5%)、CV-A4(3.2%)、EV-A71(2.1%)、埃可病毒11型(E-11)(1.5%)、CV-B5(1.0%)、CV-A9(0.9%)、CV-A5、CV-A2、PV-3、E-16、E-18、CV-A12、E-30、CV-A14、CV-B4、E-3、PV-1、CV-A21和E-7[38]。2018年广东省手足口病的病原阳性率居于前三位的分别是CV-A16(30.73%)、CV-A6(24.29%)和CV-A10(11.0%)[22]。2018年8月至2019年4月广东省茂名市、阳江市检测到的病原包括CV-A16(71.43%)、CV-A6(24.81%)、CV-A10(1.50%)、EV-A71(0.75%)、CV-A8(0.75%)和E11(0.75%);江苏省连云港市、盐城市和徐州市检测到的病原包括CV-A16(63.69%)、CV-A6(32.38%)、CV-A10(2.68%)、EV-A71(0.72%)、CV-B2(0.36%)和CV-B1(0.18%)[39]。
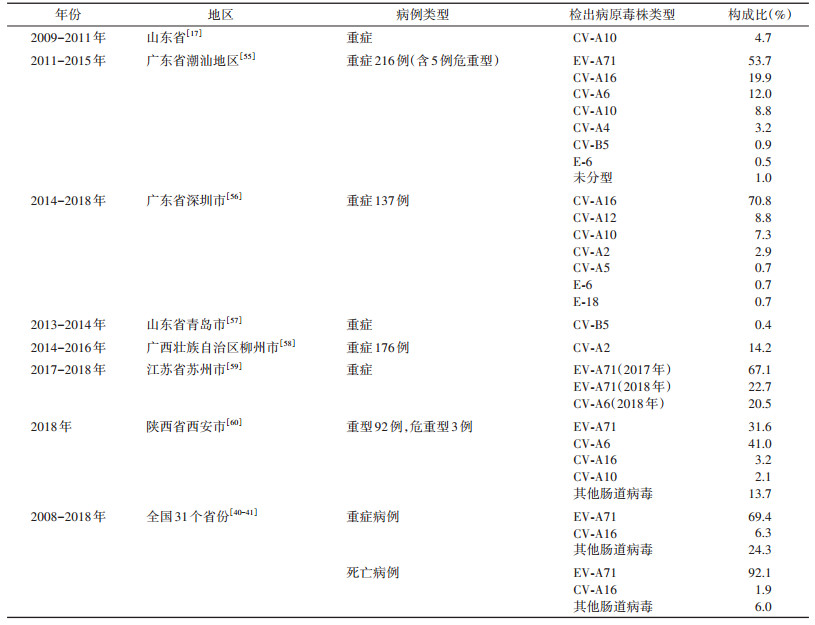
2. 重症和死亡病例病原谱:自2008年以来,我国手足口病重症病例的病原仍以EV-A71为主(69.39%),CV-A16占6.26%,其他EV占24.35%[40]。2016年EV-A71疫苗使用后,EV-A71所致重症比例明显下降,至2018年EV-A71重症病例所占比例仅为15.3%[20]。全国手足口病死亡病例中EV-A71感染占92%[41],2018年死亡病例中仍以EV-A71感染占优势(60%),但其构成比较2016年之前明显下降[20]。
EV-A71疫苗在2016年使用后,手足口病重症病原谱的变化受到进一步关注。除EV-A71以外,重症手足口病的其他EV还包括CV-A16、CV-A6、CV-A10、CV-A2、CV-A4、CV-A12、CV-B5、E-6等(表 2)。CV-A10感染引起手足口病具有重症病例相对较多的特点[42-43]。2009-2011年,山东省手足口病重症中CV-10感染占比为4.7%[17]。2015年厦门市从手足口病暴发病例中分离到CV-A10毒株;39%的重症病例为CV-A10阳性[44]。广东省2018年手足口病重症病例中EV⁃A71的重症率为9.6%(8/83),CV-A10重症率为2.2%(11/500),CV-A6所致的重症率为0.5%(7/1 374),CV-A16重症率为0.4%(7/1 738)。经统计学比较,CV-A10引起手足口病重症率低于EV-A71,但高于CV-A16和CV-A6[45]。
CV-A2也可引起重症手足口病和急性弛缓性麻痹。2012年北京市西城区从35例重症手足口病患儿的咽拭子样本中检测出1例CV-A2病毒株[46]。2012年中国香港地区从重症死亡婴幼儿的肠组织标本中检出CV-A2与EV-71和CV-A4的重组株[47]。2013年珠海市检出4例CV-A2感染重症手足口病病例,均出现神经系统受累表现[48]。2013年贵阳市手足口病病例CV-A2检出率为5.61%,不同程度出现重症的症状[49]。
3. 基因亚型和进化分支:
(1)EV-A71:分为A~F基因型,1998-2006年在我国EV-A71引起的手足口病以C4b基因亚型为流行优势株。2007年至今,全国31个省以EV-A71C4基因亚型C4a进化分支为绝对优势基因亚型[50],这一转变与2007年以来手足口病重症和死亡人数增多密切相关[45]。2016年首次从我国云南省发现了4株输入的EV-A71的B5基因亚型毒株,其在进化关系上与越南流行株同源关系较近[51],后续未见扩散。
(2)CV-A16:分为3种基因型(基因型A、B和D),基因型B包括两个基因亚型(B1、B2),B1又分3个进化分支(B1a~B1c)。2013年之前,我国CV-A16手足口病以B1a基因亚型占有绝对优势[3]。对我国22个省2016-2018年手足口病CV-A16毒株的271条全基因序列比对和进化树分析,我国有3种进化分支(B1a~B1c),CV-A16的传播仍以B1b为主,B1c分支仅在我国1个省发现,B1a毒株仅在6个省发现[52]。
(3)CV-A6:可分为A、B、C、D四种基因型,并可进一步细分为B1~B2、C1~C2和D1~D7基因亚型。对807株有代表性的CV-A6分离株进行基因型和基因亚型分析显示,D3是近年来在我国流行的主要亚型(734株),66株为D2,B1和C1各为1株,5株B2。D3亚型于2008年首次流行,2009年起成为主要的亚型,2013年达到峰值,而D2亚型在过去几年基本未检出,CV-A6在不同传播阶段以D3基因型具有更强的传播能力[53]。2013-2015年上海市部分CV-A6株在2C区与CV-A4发生了重组,聚集在D7簇,提示上海地区流行的CV-A6为新进化的流行株[54]。
(4)CV-A10:分为A~G基因型。F基因型包括F1~F3 3个亚型。2004-2009年活跃的基因型为B型,自2009年以来,C型进化为绝对优势基因型,并可进一步分为C1和C2基因亚型。2008-2012年以C1型为主,2010年以后以C2型为主。C1和C2基因亚型之间的核苷酸差异为5.8%。所有其他病毒都属于C2类,可分为C2-cluster1、C2-cluster2和C2-cluster3三个簇。组间平均距离为3.7%~6.2%。核苷酸序列比较分析,轻症、重症病例的氨基酸编码区无差异。2010年发现除1株宁夏毒株外,所有重症病例均位于C2,重症中有51.5%(17/33)的病毒位于cluster3,该病毒在2014-2016年持续传播[61]。2018-2019年,广东省和江苏省检出的CV-A10以F3亚型占优势[62]。
二、流行病学1. 发病强度:自2008年5月手足口病被纳入法定报告传染病管理以来,我国31个省(自治区、直辖市)均有报告病例,年均报告发病人数187.22万例,报告死亡病例307例,发病率为134.59/10万,死亡率为0.03/10万,病死率为0.02%[18]。不同地区报告发病率差异较大,在25.79/10万~568.81/10万[63-75]。2010年以来手足口病报告病例数位居我国法定传染病首位[18],发病率呈增长趋势,年均增加15.92%;死亡率年均下降3.49%,病死率年均下降16.86%[19]。2010年后全国≤5岁儿童报告死亡率显著下降,2018和2019年较2010年(905例)分别减少了96.13%和97.90%[41]。2008-2018年全国报告手足口病重症病例157 065例,自2010年后出现下降趋势[19-40]。2018和2019年重症数较2010年(27 907例)分别减少了83.2%和91.6%[18]。表 1可见重症比例在第二和第三时间阶段分别较第一阶段下降41%和69%,病死率在第二和第三时间阶段分别较第一阶段下降62%和88%。
2008-2017年的年均发生暴发疫情600起,暴发病例数年均11 756例,暴发死亡数年均48例[19]。2012年的暴发疫情数量(1 405起)最多,2016年出现个小高峰,之后暴发数量有所下降[19],90%的暴发疫情发生在托幼机构,6.1%发生在小学,3.3%发生在村庄,1.1%发生在儿童照看中心,0.6%发生在初中[76-78]。
2. 周期性与季节性:自2010年以来,手足口病发病数/率呈隔年高发的特征,多数地区以偶数年高发,奇数年低发[19, 63-66, 73, 79-82]。全国报告发病数以2014年最高(227.91万例);报告死亡数以2010年最高(905例),之后显著下降[19]。各地区手足口病发病的周期性波动可能与不同毒株活跃的周期性频率不同有关[67, 83]。
手足口病发病有明显季节性,并呈现双高峰,春、夏季(4-7月)为主高峰,秋季(9-11月)为小高峰[19, 65]。受地理位置和气候的影响,南、北地区发病高峰时间略有不同,一般纬度越低,发病高峰出现的时间越早。南部和中南部地区每年第一个峰值出现在4-5月,第二个峰出现在10-11月[83]。北部地区发病高峰多呈单峰型(6-7月)[63-66, 68-71],个别年份出现双高峰[63-66],部分年份西北和西部地区在9月也出现秋季小高峰[66-67],可能与当年的气候条件有关。
3. 地区及城乡差异:2008-2017年我国手足口病年均报告发病率以广东省、广西壮族自治区、福建省(南部地区)最高(298.22/10万),其次是浙江省、上海市、江苏省(东部地区)(167.18/10万);新疆维吾尔自治区、甘肃省、宁夏回族自治区、青海省、西藏自治区(西北部地区)最低(40.79/10万)。南部地区报告发病率为西北部地区的7.33倍、为东部地区的4.10倍。河南省、湖北省、安徽省、江西省、湖南省(中部地区)、重庆市、四川省、云南省、贵州省(西南部地区)的重症比例较高[19]。县(区)级报告发病率以南部地区的较高[72]。城市和农村手足口病发病特征存在地区异质性,中等城市/城区的发病率低于城乡接合部及农村[67],大城市的城乡接合部发病率高于城区[73],小城市/县级市的发病率高于农村地区[74-75],农村地区病例的重症发生率高于城区[74]。
4. 年龄和性别分布:全国≤5岁儿童手足口病占手足口病总病例数的90%以上,其中,12~23月龄组儿童的发病率和死亡率最高,在2012年每1 000人中有38.2例病例,每10 000人中有1.5例死亡[16]。年龄组发病率居前三位的1~、2~和3~岁组分别为3 184.19/10万、2 547.47/10万和2 052.19/10万[19]。在2008-2018年手足口病死亡病例以≤5岁儿童为主,占死亡总人数的99.43%,儿童手足口病死亡病例中,男性多于女性(1.82∶1),以≤2岁儿童为主(87.71%)[41]。2008-2018年重症病例中男性高于女性(1.78∶1),以≤3岁婴幼儿为主(91.47%),EV-A71引起的重症手足口病中位年龄最高(1.99岁),且有逐年升高趋势;其他EV感染在≤1岁婴儿中构成较高(66.56%)[40]。
南部地区高发年龄段与全国总体分布基本一致[72, 78-84],但在北部地区高发年龄有所升高。北京市海淀区、沈阳市均以3岁发病率最高(2 573.16/10万、4 040.99/10万)[64, 71],新疆维吾尔自治区报告病例以 < 7岁儿童为主(占92.33%)[69],与全国总体年龄构成有一定差异性。
成年人感染比例有增加趋势,占全人群发病例数的构成比由2010年的0.33%上升到2.43%;最高发病年龄由2009年的38岁上升到66岁[42, 85]。托幼机构发病率较高,手足口病年均发病率为962.48/10万,且民办托幼机构幼儿发病率高于公办托幼机构[86]。
EV-A71和CV-A16感染年龄[M(Q1,Q3):24(12,36)月龄]较大,CV-A6、CV-A10和CV-A4感染年龄[M(Q1,Q3):12(12,24)月龄]均比EV-A71和CV-A16感染的年龄小[37]。
5. 感染谱:
(1)临床分型与并发症:手足口病病例以普通型(轻症)为主,重症占0.76%[40]。住院的手足口病患儿中,普通型/轻症病例占29.26%,重症病例70.74%(重型、危重型分别占40.75%、29.99%)。较小年龄是重症的危险因素,≤3岁儿童重症病例占比为88.02%[87]。
非典型手足口病病例数有明显增多趋势。引起非典型手足口病的最常见的病原体为CV-A6,占67.2%,其次为其他EV(26.6%)、EV-A71(4.7%)和CV-A16(1.5%)[88]。重庆市7.2%(64/887)为非典型手足口病患儿,其中15.6%(10/64)的患儿表现为神经系统受累,确诊重症和危重手足口病占7.8%(5/64)[88]。CV-A6导致脱甲症的比例为28.0%(95%CI:21.9%~34.3%)[89]。
对北京市、内蒙古自治区、吉林省、江苏省、浙江省、安徽省、河南省、湖南省、广东省、云南省和甘肃省1 217例手足口病住院病例随访调查显示,并发症主要有无菌性脑膜炎(56.78%)、非脑干脑炎(23.91%)、脑干脑炎(8.98%)、心肺功能衰竭(5.09%),脑脊髓炎、急性弛缓性麻痹、肺水肿和肺出血所占比例较小。642例EV-A71所致手足口病重症病例中,无菌性脑膜炎、非脑干脑炎、脑干脑炎、心肺功能衰竭的伴发率分别为55.30%、23.99%、20.56%、6.54%;261例其他EV感染手足口病病例中,无菌性脑膜炎、非脑干脑炎、脑干脑炎、心肺功能衰竭等主要并发症的伴发率分别为50.19%、25.67%、24.14%、3.45%[90]。死亡病例发病至诊断间隔时间M(Q1,Q3)为2(2,4)d,发病至死亡间隔时间M(Q1,Q3)为3(2,4)d[41]。
我国手足口病临床诊疗指南临床分期标准分为手足口病期(第1期)、神经系统受累期(第2期)、心肺功能衰竭前期(第3期)、心肺功能衰竭期(第4期)、恢复期或后遗症期(第5期)。全国随机抽样调查,重症病例临床严重程度达到第2期的占82.5%(95%CI:79.4%~85.3%),第3期占15.1%(95%CI:12.4%~18.0%),第4期占2.4%(95%CI:1.4%~3.9%)。病例后遗症发生率为1.7%(95%CI:0.9%~3.0%),主要以神经系统症状/体征为主(81.8%)[91]。
(2)重症早期识别及危险因素:重症手足口病组与普通病例组患儿相比,高热、EV-A71-IgM阳性、合并EB病毒感染、血糖 > 8.3 mmol/L、降钙素原(PCT) > 0.1 ng/ml、中性粒细胞/淋巴细胞比值(NLR) > 1.59均为识别手足口病重症的指标[92]。血清淀粉样蛋白A和人β-肌动蛋白水平在重症手足口病患者中显著升高,可作为临床诊断重症手足口病的潜在生物标志物[93]。年龄≤3岁是重症的危险因素,危重型手足口病早期均有高血压(100.00%)、心率快(94.84%)、呼吸增快(86.44%)、指(趾)端循环不良(69.76%)、肢体瘫痪(1.83%)和尿潴留(0.41%)。危重型手足口病的病原以EV-A71感染为主[92]。EV-A71感染、发病诊断时间间隔较长和居住地为农村是手足口病死亡的危险因素[41]。
(3)重复感染率:手足口病疫情报告病例的重复感染发生率2.72%。两次感染时间间隔平均为16个月,重症、轻症病例重复感染率分别为5.56%和2.71%,EV-A71、CV-A16、其他EV感染者的重复感染发生率分别为6.56%、2.73%、3.77%[94]。一项采用血清特异性中和抗体检测结合疾病监测的队列研究发现,EV-A71、CV-A6、CV-A10、CV-A16、CV-B3和CV-B5的重复感染率分别为17.7%、13.3%、27.8%、12.2%、2.2%和4.5%,相同血清型重复感染是指在前一个时间点血清中和抗体滴度检测结果为阳性(GMT≥8)的受试者,在后一个时间点中和抗体出现4倍及以上增高,同种血清型重复感染者全部无临床症状[95]。
(4)显性和隐性感染比例:一项人群队列研究发现,手足口病总体显性感染占比为5.6%,隐性感染比例为94.4%,显性与隐性感染比为1∶17。EV-A71、CV-A6、CV-A10、CV-A16、CV-B3、CV-B5的显性感染比例分别为18.9%、1.1%、0.7%、16.9%、3.7%、1.5%,提示6种病原显性与隐性感染比分别为1∶4、1∶90、1∶142、1∶5、1∶26和1∶66,其中CV-A10、CV-A6和CV-B5发生隐性感染的比例相对较高[95]。
6. 流行因素:
(1)传染源:手足口病病例和隐性感染者/无症状感染者为主要传染源。EV-A71引起的手足口病普通型患儿第1~6周粪便排毒率为100.0%、88.4%、59.4%、22.3%、22.3%、0.0%,持续排毒时间最长为6周;EV-A71重症患儿第1~10周粪便排毒率为100.0%、97.0%、79.5%、60.6%、35.3%、25.2%、16.8%、8.4%、0.0%,持续排毒时间最长为10周[96]。健康人群中,EV-A71、CV-A16、其他EV隐性感染率分别为3.3%(95%CI:2.2%~4.4%),1.7%(95%CI:1.0%~2.5%)和15.1%(95%CI:11.1%~17.1%)[97]。0~3岁、4~6岁、7~12岁儿童的EV隐性感染率分别为48.00%、20.27%、4.37%[98]。
(2)传播途径:共用玩具、与手足口病患者接触、流动人口是感染手足口病的危险因素[99]。家庭成员中有儿童患手足口病是引起家庭内传播的危险因素,托幼儿童中EV携带者或近期有手足口病相关潜伏期病例,可能是托幼机构内传播的危险因素[100]。与EV-A71阳性手足口病患儿有密切接触的家庭成员中粪便EV-A71核酸阳性率为28.70%,与CV-A16阳性手足口病患儿有密切接触的家庭成员中粪便CV-A16核酸阳性率为32.14%,与EV通用型阳性患儿有密切接触的家庭成员中粪便EV通用型核酸阳性率为25.93%,同期检测的无手足口病接触史的健康成年人,粪便EV核酸均阴性;400例托幼机构正常幼托儿童的粪便样本仅检出1份EV阳性[101]。
护理人员的不卫生行为也是儿童传播手足口病的重要途径(OR=9.22,95%CI:1.16~73.23)。照顾者的行为,如用嘴吹儿童的食物(OR=1.85,95%CI:1.11~3.08)和使用自己的餐具喂养儿童(OR=2.19,95%CI:1.07~4.45),显著增加了儿童传播手足口病的风险,相反,在给孩子喂食前洗手可以降低发病风险,家庭经常消毒玩具,父母便后洗手习惯是预防CV-A6感染的保护因素[102-103]。
儿童聚集性场所存在手足口病病原污染,室外儿童游乐场所阳性率(32.26%)高于室内(4.83%),农村游乐场所阳性率(21.25%)高于城乡接合部(3.03%)及城市。污染最严重的物品为室外电动摇摇车,托幼机构中以课室检出核酸阳性率最高(0.46%)[103]。
(3)人群易感性:EV特异性抗体水平、基因易感性等是感染手足口病或发生重症的影响因素。在0~6月龄EV-A71血清抗体阳性率随年龄的增加而逐渐下降,7~11月龄均保持低水平(5.0%~10.0%),1~4岁年龄组升高(22.5%~87.5%)。CV-A16抗体阳性率在0~6月龄极低(0.0%~13.0%),在7月龄至4岁逐渐升高(15.0%~70.0%),在5~15岁稳定在54.0%(108/200)[104],抗体水平较低者具有感染风险。与健康对照的基因易感性比较,EV-A71手足口病男性患儿中TLR7基因rs3853839 C等位基因的易感性(OR=2.343,95%CI:1.516~3.621)与重症化(OR=1.939,95%CI:1.064~3.521)风险升高有关。男性患儿TLR7基因rs179010-T等位基因的易感性(OR=1.701,95%CI:1.142~2.535)与重症化(OR=1.852,95%CI:1.038~3.305)风险升高有关。女性患儿TLR7基因rs3853839、rs179010等位基因分布在病例组与对照组间差异不明显[105]。携带OAS1 rs2660 AG基因型的儿童在EV-A71感染后更容易累及中枢神经系统[106]。CV-A6患者中携带单核苷酸多态性(SNP)rs10879355基因与严重CV-A6型手足口病相关,CC基因型相比TT+TC基因型有更高的患重症的风险(OR=2.48,95%CI:1.34~4.56)。SNP rs4290270在我国汉族儿童中与rs10879355完全同源,与CV-A6重症相关[107]。
(4)传染率:又称有效接触率(β),β值等于研究人群的接触率与该病在易感者每次接触感染的概率(β0)之积,可反映感染者的活动能力、环境条件以及病原体的毒力。春运期间手足口病传染率快速增加(2月),2-3月均处于较高水平;各省传染率季节性多与春运有关;在暑假期间,大部分地区的传染率也有小幅度增加[108]。
(5)基本再生数(R0):衡量病原体传播能力的指标,也是区分疾病是否流行的阈值。当R0 < 1时,意味着流行将逐渐停止,R0 > 1时,意味着疾病将会持续传播和流行,R0越大,病原体传播力越强。有效再生数(Rt)指随机选择的病例在完全易感人群感染期间所能产生的平均继发感染数,基于泊松回归嵌套易感-感染-恢复统计(SIR)模型,对2008-2009年我国不同时间和地域的手足口病Rt和传播风险进行估计,总体R值(经过协变量调整)在春季为1.4(Q1,Q3:1.4,1.6),其他季节均 < 1.2[109]。基于更新的数学方程的2种方法,陕西省部分地区利用2010年、2011年和2018年的每日新增手足口病病例数估计CV-A16、EV-A71、CV-A6的R0值分别为1.33~1.46、1.20~1.29和1.38~1.59,CV-A6在3种病原体中传播能力最强,而EV-A71传播能力最差;估计手足口病日Rt在6月前和7月后均有显著波动,但在6-7月变化较小(0.5,2)[110]。基于TSIR模型对广东省2009-2012年EV-A71、CV-A16手足口病的R0估计值分别为4.621(Q1,Q3:3.907,5.823)、3.023(Q1,Q3:2.289,4.292)和7.767(Q1,Q3:6.903~10.353)[111]。基于潜伏期的R0计算方程,对2011-2018年我国手足口病暴发疫情R0进行计算,假设平均潜伏期5 d,估计EV-A71、CV-A16和CV-A6这3种病原体的R0值的M(Q1,Q3)分别为5.06(2.81,10.20)、4.84(3.00,9.00)、5.94(3.27,10.00)[77]。
(6)气象影响因素:一项对51项研究的Meta分析发现,气象参数在手足口病的流行中起着重要作用。只有平均气压与手足口病发病率呈负相关,而其他5个气象参数(平均气温、相对湿度、降雨量、日照和平均风速)与手足口病发病率呈正相关[112]。
基于交叉相关分析和回归树(classification and regression trees,CART)模型,对广州市2010-2017年手足口病流行与暴发的气象因素进行分析时发现,其月平均气温和相对湿度与手足口病月发病数有相关性;当月平均气温≥22.3 ℃,且前一个月平均相对湿度≥82.37%时,手足口病发病风险增高(RR=2.06,95%CI:1.99~2.13);当月平均气温≥24.6 ℃,且上一个月平均相对湿度≥83.92%时,手足口病暴发风险显著升高(RR=3.54,95%CI:3.03~4.03)[113]。
珠江三角洲地区手足口病发病可由约1周前的气象因素所解释,温度对手足口病流行的贡献最大(28.99%~71.93%),其次是降水量(6.52%~6.11%)、湿度(3.92%~17.66%)、风速(3.84%~11.37%)和日照(6.21%~10.36%)。温度在10 ℃~25 ℃,湿度在70%~90%,对手足口病的流行有促进作用。日照时间 > 9 h和风速 < 2.5 m/s也增加了手足口病的发病风险。日降水量 > 25 mm时,手足口病与降水量呈负相关关系。年龄较小的儿童对天气变化更敏感[114]。平均气温、相对湿度和风速可能是深圳市儿童手足口病发病的危险因素,前6 d日平均温度每增加1 ℃,发病超额相对风险为2.75%(95%CI:1.98%~3.53%);前3 d风速每增加1 m/s的发病超额风险为3.93%(95%CI:2.16%~5.73%)。相对湿度具有非线性效应(低阈值为45%,高阈值为85%),在阈值范围内存在正效应,前5 d相对湿度增加1%的超额相对风险为1.06%(95%CI:0.85%~1.27%)。降水量和日照时间的影响不显著[115]。
安徽省蚌埠市手足口病发病率与气候因素研究发现,当气温为16 ℃~25 ℃时发病数趋于发病高峰,气温高于26 ℃时,发病率下降;风速与发病率呈正相关,线性回归方程为手足口病月发病率=-11.244+0.704×月平均气温+8.184×月平均风速[116]。安徽省合肥市相对湿度超过84%时,对儿童手足口病发病的影响增加,相对湿度每增加1%,儿童手足口病发病率增加0.34%(95%CI:0.23%~0.45%)。在城市儿童、男性儿童和0~4岁儿童因相对湿度增加而出现手足口病发病增加更为明显[117]。
我国地域辽阔、环境多样,纬度并不是影响手足口病传播的唯一因素[118-121]。手足口病流行热点主要分布在省会城市周边的区县和城乡接合部。这可能与人口密度、经济条件和人口间交叉感染有关。手足口病疫情在沿海城市较为常见,发病率较高[122]。
(7)EV-A71疫苗接种的效果:2016年,我国有3个EV-A71单价灭活疫苗先后注册上市。疫苗Ⅲ期临床试验显示,对所有EV-A71导致的手足口病的保护效力均 > 90%,对重症手足口病的保护效力达100%[123-125]。截至2018年北京市对5岁儿童疫苗覆盖率已达30%,对EV-A71感染起到保护作用[126]。
通过在全时间序列中拟合一个变点模型评估接种EV-A71型手足口病疫苗接种后的趋势发现,成都市2017-2018年EV-A71手足口病的平均发病率比未接种疫苗时的预测低60%(95%CI:41%~72%),估计2年内避免了6 911(95%CI:3 246~11 542)例EV-A71病例。重症手足口病病例比预测减少52%(95%CI:42%~60%)。疫苗接种后4个月EV-A71型手足口病的趋势显著下降。而非CV-A16型和非EV-A71型手足口病的发病率在2018年有所上升。表明接种EV-A71疫苗对儿童手足口病有效,提供了真实世界的证据[127]。
采用时间序列方法对广州市2016年1月至2018年12月EV-A71疫苗接种效果进行分析结果显示,该疫苗接种在3岁儿童中对手足口病有保护性关联,接种率增加1%,手足口病病例减少0.9%,EV-A71组病例减少1.4%和其他EV减少1.3%,但对CV-A16病例没有影响[128]。如采用同时考虑疫苗接种、污染环境和检疫的新的数学模型,从2016年接种疫苗可使2016年和2017年的手足口病总患病人数分别减少了17%和22%[129]。
2016年9月至2017年12月,广东省共报告接种EV-A71灭活疫苗2 304 456剂次,2016、2017年平均估算接种率分别为3.82%和10.07%。深圳市估算接种率最高,2016、2017年分别为6.05%和19.76%。2017年广东省EV-A71型手足口病发病率比2016年下降39.97%,EV-A71型手足口病重症及死亡数下降53.33%[130]。2017-2019年广东省江门市接种EV-A71疫苗3年估算接种率分别为17.96%、29.33%和30.75%,同时估算发病率分别为21.21/10万、3.02/10万和0,呈逐年下降趋势;手足口病报告发病率2018年比2017年下降42.17%,2019年比2018年上升54.45%。表明接种EV-A71灭活疫苗能有效降低EV-A71感染所致的手足口病发病率,重症数明显减少[131]。
三、总结我国自2008年以来手足口病持续流行,病原构成和优势病原发生一定变化。手足口病的广泛流行与传染率和传播力较高,易感人群存在,传播途径多样,以及气候、人口等因素的影响有关。疾病监测数据显示,EV-A71疫苗的应用有效减少了EV-A71引起的手足口病发病、重症和死亡,但手足口病发病率尚未明显下降,引起手足口病的其他EV的流行逐渐增多,2017-2019年CV-A16流行也有所增强,表明开发多价疫苗的必要性。临床疾病谱呈多样化,重症病例的早期识别极为重要。手足口病的隐性感染率占较高比例,家庭/托幼机构/学校内的密切接触及不卫生行为的暴露是疾病传播的危险因素,需采取有效的干预措施防控手足口病。
利益冲突 所有作者声明无利益冲突
| [1] |
Wu Y, Yeo A, Phoon MC, et al. The largest outbreak of hand, foot and mouth disease in Singapore in 2008:the role of enterovirus 71 and coxsackievirus A strains[J]. Int J Infect Dis, 2010, 14(12): e1076-1081. DOI:10.1016/j.ijid.2010.07.006 |
| [2] |
Pallansch MA, Roos R. Enteroviruses: polioviruses, coxsackieviruses, echoviruses, and newer enteroviruses[M]//Fields virology (Volume 1). Philadelphia: Lippincott, Williams & Wilkins, 2007: 839-894.
|
| [3] |
Zhang Y, Wang DY, Yan DM, et al. Molecular evidence of persistent epidemic and evolution of subgenotype B1 coxsackievirus A16-associated hand, foot, and mouth disease in China[J]. J Clin Microbiol, 2010, 48(2): 619-622. DOI:10.1128/JCM.02338-09 |
| [4] |
Robinson CR, Doane FW, Rhodes AJ. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957;isolation of group A coxsackie virus[J]. Can Med Assoc J, 1958, 79(8): 615-621. |
| [5] |
Ho M, Chen ER, Hsu KH, et al. An epidemic of enterovirus 71 infection in Taiwan[J]. N Engl J Med, 1999, 341(13): 929-935. DOI:10.1056/NEJM199909233411301 |
| [6] |
Zhao YY, Jin H, Zhang XF, et al. Case-fatality of hand, foot and mouth disease associated with EV71:a systematic review and meta-analysis[J]. Epidemiol Infect, 2015, 143(14): 3094-3102. DOI:10.1017/S095026881500028X |
| [7] |
Liu WY, Wu SM, Xiong Y, et al. Co-circulation and genomic recombination of coxsackievirus A16 and enterovirus 71 during a large outbreak of hand, foot, and mouth disease in Central China[J]. PLoS One, 2014, 9(4): e96051. DOI:10.1371/journal.pone.0096051 |
| [8] |
Fang YR, Wang SP, Zhang LJ, et al. Risk factors of severe hand, foot and mouth disease: a meta-analysis[J]. Scand J Infect Dis, 2014, 46(7): 515-522. DOI:10.3109/00365548.2014.907929 |
| [9] |
Koh WM, Bogich T, Siegel K, et al. The epidemiology of hand, foot and mouth disease in Asia: A systematic review and analysis[J]. Pediatr Infect Dis J, 2016, 35(10): e285-300. DOI:10.1097/INF.0000000000001242 |
| [10] |
Zhang Y, Tan XJ, Wang HY, et al. An outbreak of hand, foot, and mouth disease associated with subgenotype C4 of humanenterovirus 71 in Shandong, China[J]. J Clin Virol, 2009, 44(4): 262-267. DOI:10.1016/j.jcv.2009.02.002 |
| [11] |
Zhang Y, Zhu Z, Yang WZ, et al. An emerging recombinant human enterovirus 71 responsible for the 2008 outbreak of hand foot and mouth disease in Fuyang city of China[J]. Virol J, 2010, 7: 94. DOI:10.1186/1743-422X-7-94 |
| [12] |
Zhang Y, Wang JT, Guo WS, et al. Emergence and transmission pathways of rapidly evolving evolutionary branch C4a strains of human enterovirus 71 in the Central Plain of China[J]. PLoS One, 2011, 6(11): e27895. DOI:10.1371/journal.pone.0027895 |
| [13] |
Österback R, Vuorinen T, Linna M, 等. Coxsackievirus A6 and hand, foot, and mouth disease, Finland[J]. Emerg Infect Dis, 2009, 15(9): 1485-1488. DOI:10.3201/eid1509.090438 |
| [14] |
Ji TJ, Han TL, Tan XJ, et al. Surveillance, epidemiology, and pathogen spectrum of hand, foot, and mouth disease in mainland of China from 2008 to 2017[J]. Biosaf Health, 2019, 1(1): 32-40. DOI:10.1016/j.bsheal.2019.02.005 |
| [15] |
Zhang J, Sun JL, Chang ZR, et al. Characterization of hand, foot, and mouth disease in China between 2008 and 2009[J]. Biomed Environ Sci, 2011, 24(3): 214-221. DOI:10.3967/0895-3988.2011.03.002 |
| [16] |
Xing WJ, Liao QH, Viboud C, et al. Hand, foot, and mouth disease in China, 2008-12:an epidemiological study[J]. Lancet Infect Dis, 2014, 14(4): 308-318. DOI:10.1016/S1473-3099(13)70342-6 |
| [17] |
Lu QB, Zhang XA, Wo Y, et al. Circulation of coxsackievirus A10 and A6 in hand-foot-mouth disease in China, 2009-2011[J]. PLoS One, 2012, 7(12): e52073. DOI:10.1371/journal.pone.0052073 |
| [18] |
中国疾病预防控制中心. 中国重点传染病监测年度报告[R]. 北京: 中国疾病预防控制中心, 2020. Chinese Center for Disease Control and Prevention. Annual report on surveillance of key infectious diseases in China[R]. Beijing: Chinese Center for Disease Control and Prevention, 2020. |
| [19] |
张静. 2008-2017年中国手足口病流行趋势和病原变化动态数列分析[J]. 中华流行病学杂志, 2019, 40(2): 147-154. Zhang J. Trend of epidemics and variation of pathogens of hand, foot and mouth disease in China: a dynamic series analysis, 2008-2017[J]. Chin J Epidemiol, 2019, 40(2): 147-154. DOI:10.3760/cma.j.issn.0254-6450.2019.02.005 |
| [20] |
Liu FF, Ren MR, Chen SM, et al. Pathogen spectrum of hand, foot, and mouth disease based on laboratory surveillance-China, 2018[J]. China CDC Wkly, 2020, 2(11): 167-171. DOI:10.46234/ccdcw2020.044 |
| [21] |
谢中勇, 卢远达, 杨坤祥, 宋足琼. 惠州市2016-2018年手足口病流行病学及病原学变化分析[J]. 广东医学, 2020, 41(3): 234-237. DOI: 10.13820/j.cnki.gdyx.20191521. Xie ZY, Lu YD, Yang KX, et al. Analysis of the epidemiological and etiological changes of hand, foot and mouth disease in Huizhou from 2016 to 2018[J]. Guangdong Med J, 2020, 41(3): 234-237. DOI: 10.13820/j.cnki.gdyx.20191521. |
| [22] |
曾汉日, 陆靖, 郑焕英, 等. 中国广东省18株柯萨奇病毒A6型分离株全基因组特征分析[J]. 病毒学报, 2016, 32(5): 566-573. Zeng HR, Lu J, Zheng HY, et al. The complete sequence analysis of 18 strains of coxsackievirus A6 in Guangdong province of China[J]. Chin J Virol, 2016, 32(5): 566-573. DOI:10.13242/j.cnki.bingduxuebao.003022 |
| [23] |
许少坚, 任燕, 郝夏琼, 等. 深圳市龙华区2018年手足口病病原学特征[J]. 中国热带医学, 2019, 19(10): 972-976. Xu SJ, Ren Y, Hao XQ, et al. Characteristics of the pathogen for hand-foot-and-mouth disease in Longhua District, Shenzhen in 2018[J]. China Trop Med, 2019, 19(10): 972-976. DOI:10.13604/j.cnki.46-1064/r.2019.10.14 |
| [24] |
吴志强, 熊焰, 刘  , 等. 2016-2018年武汉地区手足口病病原学和流行病学调查[J]. 武汉大学学报: 医学版, 2019, 40(3): 429-434. , 等. 2016-2018年武汉地区手足口病病原学和流行病学调查[J]. 武汉大学学报: 医学版, 2019, 40(3): 429-434.Wu ZQ, Xiong Y, Liu T, et al. An epidemiologic survey of hand, foot and mouth disease (HFMD) in Wuhan area from 2016 to 2018[J]. Med J Wuhan Univ, 2019, 40(3): 429-434. DOI:10.14188/j.1671-8852.2018.0912 |
| [25] |
徐长征, 文丹宁, 周金戈, 等. 2018年武汉地区手足口病肠道病毒分子流行病学分析[J]. 中国生物制品学杂志, 2020, 33(11): 1262-1269. Xu CZ, Wen DN, Zhou JG, et al. Molecular epidemiological analysis of enteroviruses associated with hand, foot and mouth disease in Wuhan in 2018[J]. Chin J Biologicals, 2020, 33(11): 1262-1269. DOI:10.13200/j.cnki.cjb.003196 |
| [26] |
文艳, 杨小蓉, 陈果, 等. 四川省绵阳市2015-2018年手足口病流行特征[J]. 中国热带医学, 2020, 20(5): 462-465. Wen Y, Yang XR, Chen G, et al. Epidemic characteristics of hand-foot-mouth disease in Mianyang, Sichuan, 2015-2018[J]. China Trop Med, 2020, 20(5): 462-465. DOI:10.13604/j.cnki.46-1064/r.2020.05.14 |
| [27] |
沈来红, 李琴, 吕沛骏, 等. 攀枝花市2018年手足口病病原学特征分析[J]. 医学动物防制, 2020, 36(9): 827-830. Shen LH, Li Q, Lv PJ, et al. Pathogenic characteristics of hand-foot-mouth disease in Panzhihua, 2018[J]. J Med Pest Control, 2020, 36(9): 827-830. DOI:10.7629/yxdwfz202009003 |
| [28] |
韦欢欢, 刘宁, 陈飞, 等. 2015-2019年北京佑安医院手足口病特征分析[J]. 中国病毒病杂志, 2020, 10(6): 426-429. Wei HH, Liu N, Chen F, et al. Characteristics of hand, foot and mouth disease identified in Beijing You'an Hospital from 2015 to 2019[J]. Chin J Viral Dis, 2020, 10(6): 426-429. DOI:10.16505/j.2095-0136.2020.0063 |
| [29] |
张文俊, 刘莹莹, 于秋丽, 等. 2013-2017年河北省其他肠道病毒手足口病流行及病原构成特征分析[J]. 中国病原生物学杂志, 2018, 13(10): 1126-1130. Zhang WJ, Liu YY, Yu QL, et al. Epidemiological characteristics and pathogenic monitoring of hand, foot, and mouth disease due to an enterovirus other than enterovirus 71 or Coxsackievirus A16 in Hebei from 2013-2017[J]. J Pathogen Biol, 2018, 13(10): 1126-1130. DOI:10.13350/j.cjpb.181014 |
| [30] |
于伟, 杜晓兰, 张倩, 等. 2013-2018年辽宁省手足口病病原学监测及其分子特征分析[J]. 病毒学报, 2020, 36(1): 26-34. Yu W, Du XL, Zhang Q, et al. Pathogenic surveillance of HFMD in Liaoning province, China, from 2013 to 2018[J]. Chin J Virol, 2020, 36(1): 26-34. DOI:10.13242/j.cnki.bingduxuebao.003634 |
| [31] |
王笑笑, 蔡剑, 韩桃利, 等. 2009-2017年浙江省手足口病流行病学特征及病原学监测分析[J]. 中华实验和临床病毒学杂志, 2019, 33(1): 1-5. Wang Xiaoxiao, Cai Jian, Han Taoli, et al. Epidemiologic characteristics and pathogen surveillance of hand, foot and mouth disease in Zhejiang province, 2009-2017[J]. Chinese Journal of Experimental and Clinical Virology, 2019, 33(1): 1-5. DOI:10.3760/cma.j.issn.1003-9279.2019.01.001 |
| [32] |
樊旭成, 房师松, 陈薇, 等. 2018年乌鲁木齐市手足口病病原学检测结果分析[J]. 热带医学杂志, 2020, 20(3): 410-413. Fan XC, Fang SS, Chen W, et al. Etiology analysis for hand, foot and mouth disease in Urumuqi in 2018[J]. J Trop Med, 2020, 20(3): 410-413. DOI:10.3969/j.issn.1672-3619.2020.03.033 |
| [33] |
吴倩, 徐勤, 周信, 等. 2015至2019年扬州市手足口病病原学特征分析[J]. 中华预防医学杂志, 2021, 55(3): 394-398. Wu Q, Xu Q, Zhou X, et al. Etiological characteristics of hand, foot and mouth disease in Yangzhou from 2015 to 2019[J]. Chin J Prevent Med, 2021, 55(3): 394-398. DOI:10.3760/cma.j.cn112150-20200512-00721 |
| [34] |
Blomqvist S, Klemola P, Kaijalainen S, et al. Co-circulation of coxsackieviruses A6 and A10 in hand, foot and mouth disease outbreak in Finland[J]. J Clin Virol, 2010, 48(1): 49-54. DOI:10.1016/j.jcv.2010.02.002 |
| [35] |
Tian HF, Zhang Y, Sun Q, et al. Prevalence of multiple enteroviruses associated with hand, foot, and mouth disease in Shijiazhuang city, Hebei province, China: outbreaks of coxsackieviruses A10 and B3[J]. PLoS One, 2014, 9(1): e84233. DOI:10.1371/journal.pone.0084233 |
| [36] |
钟家禹, 李柏生, 朱冰, 等. 2016年至2017年广州市手足口病流行病学及非肠道病毒A组71型非柯萨奇病毒A组16型肠道病毒型别分析[J]. 中华传染病杂志, 2018, 36(12): 747-751. Zhong JY, Li BS, Zhu B, et al. Hand, foot, and mouth disease in Guangzhou, 2016-2017:an epidemiological study and genotype analysis of non-enterovirus group A71 non-coxsackievirus group A16 enterovirus[J]. Chin J Infect Dis, 2018, 36(12): 747-751. DOI:10.3760/cma.j.issn.1000-6680.2018.12.006 |
| [37] |
Gao LD, Zou G, Liao QH, et al. Spectrum of enterovirus serotypes causing uncomplicated hand, foot, and mouth disease and enteroviral diagnostic yield of different clinical samples[J]. Clin Infect Dis, 2018, 67(11): 1729-1735. DOI:10.1093/cid/ciy341 |
| [38] |
Xie J, Yang XH, Hu SQ, et al. Co-circulation of coxsackieviruses A-6, A-10, and A-16 causes hand, foot, and mouth disease in Guangzhou city, China[J]. BMC Infect Dis, 2020, 20: 271. DOI:10.1186/s12879-020-04992-x |
| [39] |
刘思远, 霍雅倩, 顾美蓉, 等. 2018-2019年广东省和江苏省手足口病病原分子流行特征分析[J]. 中国生物制品学杂志, 2021, 34(2): 186-191. Liu SY, Huo YQ, Gu MR, et al. Molecular epidemic characteristics of pathogen of hand, foot and mouth disease in Guangdong and Jiangsu provinces, China from 2018 to 2019[J]. Chin J Biol, 2021, 34(2): 186-191. DOI:10.13200/j.cnki.cjb.003270 |
| [40] |
任敏睿, 崔金朝, 聂陶然, 等. 2008-2018年中国手足口病重症病例流行病学特征分析[J]. 中华流行病学杂志, 2020, 41(11): 1802-1807. Ren MR, Cui JZ, Nie TR, et al. Epidemiological characteristics of severe cases of hand, foot, and mouth disease in China, 2008-2018[J]. Chin J Epidemiol, 2020, 41(11): 1802-1807. DOI:10.3760/cma.j.cn112338-20200201-00063 |
| [41] |
崔金朝, 聂陶然, 任敏睿, 等. 2008-2018年中国5岁及以下儿童手足口病死亡病例流行病学特征[J]. 中华流行病学杂志, 2020, 41(7): 1041-1046. Cui JZ, Nie TR, Ren MR, et al. Epidemiological characteristics of fatal cases of hand, foot, and mouth disease in children under 5 years old in China, 2008-2018[J]. Chin J Epidemiol, 2020, 41(7): 1041-1046. DOI:10.3760/cma.j.cn112338-20200114-00031 |
| [42] |
He YQ, Chen L, Xu WB, et al. Emergence, circulation, and spatiotemporal phylogenetic analysis of coxsackievirus A6- and coxsackievirus A10-associated hand, foot, and mouth disease infections from 2008 to 2012 in Shenzhen, China[J]. J Clin Microbiol, 2013, 51(11): 3560-3566. DOI:10.1128/JCM.01231-13 |
| [43] |
于秋丽, 刘莹莹, 赵文娜, 等. 河北省2013-2017年其他肠道病毒手足口病重症和死亡病例流行病学和病原特征分析[J]. 中华流行病学杂志, 2020, 41(7): 1054-1057. Yu QL, Liu YY, Zhao WN, et al. Epidemiological and pathogenic characteristics of cases with severe and fatal hand, foot, and mouth disease caused by other enterovirus in Hebei province, 2013-2017[J]. Chin J Epidemiol, 2020, 41(7): 1054-1057. DOI:10.3760/cma.j.cn112338-20190802-00575 |
| [44] |
Chen MY, He SZ, Yan Q, et al. Severe hand, foot and mouth disease associated with Coxsackievirus A10 infections in Xiamen, China in 2015[J]. J Clin Virol, 2017, 93: 20-24. DOI:10.1016/j.jcv.2017.05.011 |
| [45] |
曾汉日, 郑焕英, 刘冷, 等. 广东省2018年手足口病病原谱及柯萨奇病毒A10型基因特征分析[J]. 病毒学报, 2020, 36(6): 1028-1036. Zeng HR, Zheng HY, Liu L, et al. Etiological spectrum of HFMD and genetic characteristics of coxsackievirus A10 in Guangdong province, China, in 2018[J]. Chin J Virol, 2020, 36(6): 1028-1036. DOI:10.13242/j.cnki.bingduxuebao.003756 |
| [46] |
吉彦莉, 王永全. 手足口病重症病例特征分析及其病原型别分子鉴定[J]. 现代预防医学, 2012, 39(11): 2817-2819. Ji YL, Wang YQ. Analysis on the characteristics of severe hand foot and mouth disease cases and molecular typing of the causative agent[J]. Mod Prev Med, 2012, 39(11): 2817-2819. |
| [47] |
Yip CCY, Lau SKP, Woo PCY, et al. Recombinant coxsackievirus A2 and deaths of children, Hong Kong, 2012[J]. Emerg Infect Dis, 2013, 19(8): 1285-1288. DOI:10.3201/eid1908.121498 |
| [48] |
周兰兰, 魏泉德, 张丽荣, 等. 珠海市2013年手足口病患儿柯萨奇病毒A2型分离株基因特征分析[J]. 中国病毒病杂志, 2015, 5(2): 109-113. Zhou LL, Wei QD, Zhang LR, et al. Genetic characteristics of coxsackievirus A2 isolated from children with hand-foot-mouth disease in Zhuhai city of China in 2013[J]. Chin J Viral Dis, 2015, 5(2): 109-113. DOI:10.16505/j.2095-0136.2015.02.001 |
| [49] |
杨兴林, 梁跃东, 洪章萍, 等. 贵阳地区2013年手足口病非EV71、非CVA16型肠道病毒的检测分析[J]. 重庆医学, 2016, 45(17): 2343-2345. Yang XL, Liang YD, Hong ZP, et al. Etiology study of hand, foot and mouth disease related non-EV71, non-CoxA16 enteroviruses in Guiyang area during 2013[J]. Chongqing Med, 2016, 45(17): 2343-2345. DOI:10.3969/j.issn.1671-8348.2016.17.012 |
| [50] |
Zhang Y, Tan XJ, Cui AL, et al. Complete genome analysis of the C4 subgenotype strains of enterovirus 71:predominant recombination C4 viruses persistently circulating in China for 14 years[J]. PLoS One, 2013, 8(2): e56341. DOI:10.1371/journal.pone.0056341 |
| [51] |
黄克强, 寸建萍, 韩振志, 等. 云南省2016年输入性B5基因亚型EV-A71的鉴定和基因特征分析[J]. 病毒学报, 2018, 34(3): 328-333. Huang KQ, Cun JP, Han ZZ, et al. Genetic analysis and identification of imported EV-A71 in Yunnan province, China in 2016[J]. Chin J Virol, 2018, 34(3): 328-333. DOI:10.13242/j.cnki.bingduxuebao.003372 |
| [52] |
Han ZZ, Song Y, Xiao JB, et al. Genomic epidemiology of coxsackievirus A16 in mainland of China, 2000-18[J]. Virus Evol, 2020, 6(2): veaa084. DOI:10.1093/ve/veaa084 |
| [53] |
Song Y, Zhang Y, Ji TJ, et al. Persistent circulation of Coxsackievirus A6 of genotype D3 in mainland of China between 2008 and 2015[J]. Sci Rep, 2017, 7: 5491. DOI:10.1038/s41598-017-05618-0 |
| [54] |
张晓玲, 俞慧菊, 宋志刚, 等. 上海市柯萨奇病毒A6型流行株基因进化与选择压力分析[J]. 国际病毒学杂志, 2017, 24(6): 365-369. Zhang XL, Yu HJ, Song ZG, et al. Genetic evolution and selection pressure analysis on the epidemic strains of coxsackievirus A6 in Shanghai area[J]. Int J Virol, 2017, 24(6): 365-370. DOI:10.3760/cma.j.issn.1673-4092.2017.06.002 |
| [55] |
蔡晓莹, 杨林芝, 林广裕, 等. 潮汕地区2011至2015年重症手足口病病原学变化趋势分析[J]. 中国小儿急救医学, 2018, 25(1): 27-31. Cai XY, Yang LZ, Lin GY, et al. Change trends of pathogen of severe hand, foot and mouth disease in Chaoshan area during 2011 to 2015[J]. Chin Pediatr Emerg Med, 2018, 25(1): 27-31. DOI:10.3760/cma.j.issn.1673-4912.2018.01.008 |
| [56] |
Chen L, Xu SJ, Yao XJ, et al. Molecular epidemiology of enteroviruses associated with severe hand, foot and mouth disease in Shenzhen, China, 2014-2018[J]. Arch Virol, 2020, 165(10): 2213-2227. DOI:10.1007/s00705-020-04734-z |
| [57] |
梁荣香, 史晓燕, 张艳辉, 等. 2013-2014年青岛市柯萨奇病毒B5型手足口病病原学及重症病例临床特征[J]. 中华预防医学杂志, 2018, 52(11): 1168-1172. Liang RX, Shi XY, Zhang YH, et al. Etiology and clinical analysis of central nervous system infection caused by Coxsackievirus B5 in severe hand, foot and mouth disease in Qingdao city, 2013-2014[J]. Chin J Prev Med, 2018, 52(11): 1168-1172. DOI:10.3760/cma.j.issn.0253-9624.2018.11.014 |
| [58] |
黄萍, 陈柳军, 余钧池. 2014-2016年柳州市重症手足口病柯萨奇病毒A2型病毒株基因特征分析[J]. 中国病毒病杂志, 2017, 7(2): 120-123. Huang P, Chen LJ, Yu JC. Genetic characteristics of coxsackievirus A2 isolated from severe hand, foot and mouth disease from 2014 to 2016 in Liuzhou city of China[J]. Chin J Viral Dis, 2017, 7(2): 120-123. DOI:10.16505/j.2095-0136.2017.02.007 |
| [59] |
夏瑜, 徐俊, 董泽丰, 等. 2017-2018年江苏省苏州市手足口病病原学及重症监测分析[J]. 医学动物防制, 2020, 36(7): 652-654. Xia Y, Xu J, Dong ZF, et al. Etiological and intensive surveillance of hand-foot-mouth disease in Suzhou of Jiangsu province from 2017 to 2018[J]. J Med Pest Control, 2020, 36(7): 652-654. DOI:10.7629/yxdwfz202007012 |
| [60] |
邓慧玲, 张玉凤, 薛泽润, 等. 2018年西安地区重症手足口病病原学及临床特点[J]. 中华实用儿科临床杂志, 2019, 34(22): 1715-1719. Deng HL, Zhang YF, Xue ZR, et al. Etiological and clinical characteristics of severe hand, foot and mouth disease in Xi'an in 2018[J]. Chin J Appl Clin Pediatr, 2019, 34(22): 1715-1719. DOI:10.3760/cma.j.issn.2095-428X.2019.22.009 |
| [61] |
Ji TJ, Guo Y, Huang W, et al. The emerging sub-genotype C2 of Coxsackievirus A10 Associated with Hand, Foot and Mouth Disease extensively circulating in mainland of China[J]. Sci Rep, 2018, 8: 13357. DOI:10.1038/s41598-018-31616-x |
| [62] |
卞莲莲, 毛群颖, 高帆, 等. 我国大陆地区柯萨奇病毒A组10型流行株基因特征分析[J]. 中国病毒病杂志, 2018, 8(6): 509-514. DOI: CNKI:SUN:ZRYX.0.2018-06-015. Bian LL, Mao QY, Gao F, et al. Genotype analysis of coxsackievirus A10 strains circulating in Mainland China[J]. Chin J Viral Dis. 2018, 8(6): 509-514. DOI: CNKI:SUN:ZRYX.0.2018-06-015. |
| [63] |
宋丹, 潘雍. 2009-2017年天津市河北区手足口病流行特征分析[J]. 社区医学杂志, 2019, 17(5): 247-250. Song D, Pan Y. Analysis on the epidemiologic characteristics of hand foot and mouth disease in Hebei District of Tianjin in 2009-2017[J]. J Community Med, 2019, 17(5): 247-250. |
| [64] |
华伟玉, 刘锋. 2009-2017年北京市海淀区手足口病流行病学及病原学特征分析[J]. 预防医学情报杂志, 2019, 35(7): 687-691. Hua WY, Liu F. Epidemiological and etiological characteristics analysis of hand-foot-mouth disease in haidian district of Beijing from 2009 to 2017[J]. J Prev Med Inf, 2019, 35(7): 687-691. |
| [65] |
陈飒, 赵斌, 刘艳, 等. 陕西省2009-2018年手足口病流行特征及动态变化分析[J]. 中华流行病学杂志, 2019, 40(9): 1120-1124. Chen S, Zhao B, Liu Y, et al. Dynamics and epidemiological characteristics of hand, foot and mouth disease in Shaanxi province, 2009-2018[J]. Chin J Epidemiol, 2019, 40(9): 1120-1124. DOI:10.3760/cma.j.issn.0254-6450.2019.09.019 |
| [66] |
常源兴, 袁伟鹏, 银万栋, 等. 2009-2018年张掖市手足口病流行特征分析[J]. 疾病预防控制通报, 2019, 34(5): 68-70, 76. Chang YX, Yuan WP, Yin WD, et al. Epidemiological characteristics of hand, foot and mouth disease in Zhangye city from 2009 to 2018[J]. Bull Dis Control Prev (China), 2019, 34(5): 68-70, 76. DOI:10.13215/j.cnki.jbyfkztb.1909011 |
| [67] |
段丽华, 鲜洪, 杨九洲, 等. 2009-2018年绵竹市手足口病流行病学特征分析[J]. 职业卫生与病伤, 2019, 34(4): 214-219. Duan LH, Xian H, Yang JZ, et al. Analysis of epidemiological characteristics of hand-foot-mouth disease from 2009 to 2018 in Mianzhu city[J]. Occup Health Damage, 2019, 34(4): 214-219. |
| [68] |
丁惠萍, 徐玉凤. 吴忠市2009-2018年手足口病流行病学特征及病原学监测分析[J]. 宁夏医科大学学报, 2019, 41(7): 720-723. Ding HP, Xu YF. Epidemiological characteristics and pathogenic detection of hand-foot-and-mouth disease in Wuzhong city from 2009 to 2018[J]. J Ningxia Med Univ, 2019, 41(7): 720-723. DOI:10.16050/j.cnki.issn1674-6309.2019.07.017 |
| [69] |
刘万里, 黄永迪, 马会来, 等. 2011-2015年新疆手足口病流行病学特征分析[J]. 新疆医科大学学报, 2018, 41(3): 357-361, 365. Liu WL, Huang YD, Ma HL, et al. Epidemiological characteristics of hand foot and mouth disease in Xinjiang over 2011-2015 years[J]. J Xinjiang Med Univ, 2018, 41(3): 357-361, 365. DOI:10.3969/j.issn.1009-5551.2018.03.024 |
| [70] |
栾博, 赵庆龙, 沈博, 等. 吉林省2008-2018年手足口病流行特征分析[J]. 实用预防医学, 2020, 27(1): 65-68. Luan B, Zhao QL, Shen B, et al. Epidemic characteristics of hand-foot-mouth disease in Jilin province, 2008-2018[J]. Pract Prev Med, 2020, 27(1): 65-68. |
| [71] |
白杉. 2008-2017年沈阳市手足口病流行病学特征[J]. 职业与健康, 2018, 34(22): 3095-3098, 3102. Bai S. Epidemiological characteristics of hand-foot-mouth disease in Shenyang city from 2008-2017[J]. Occup Health, 2018, 34(22): 3095-3098, 3102. DOI:10.13329/j.cnki.zyyjk.2018.0866 |
| [72] |
罗亮, 王玲, 邵际晓, 等. 深圳市坪山区2011-2018年手足口病流行特征分析[J]. 国际病毒学杂志, 2020, 27(6): 508-511. Luo L, Wang L, Shao JX, et al. Epidemiological analysis of hand, foot, and mouth disease in Pingshan district of Shenzhen city, 2011-2018[J]. Int J Virol, 2020, 27(6): 508-511. DOI:10.3760/cma.j.issn.1673-4092.2020.06.017 |
| [73] |
魏崇崇, 施超, 葛桂芝. 无锡市手足口病流行特征和病原学分析[J]. 预防医学, 2019, 31(11): 1156-1158. Wei CC, Shi C, Ge GZ. The epidemiological characteristics and pathogenologic analysis of hand-foot-mouth disease of Wuxi city[J]. Prev Med, 2019, 31(11): 1156-1158. DOI:10.19485/j.cnki.issn2096-5087.2019.11.020 |
| [74] |
赵球平, 李旭东, 王悦, 等. 仙桃市2008-2016年手足口病流行病学特征[J]. 海峡预防医学杂志, 2018, 24(2): 38-40. Zhao QP, Li XD, Wang Y, et al. Epidemiology characteristics of foot and mouth disease in Xiantao city, Hubei, 2008-2016[J]. Strait J Prev Med, 2018, 24(2): 38-40. |
| [75] |
禹长兰, 李方友, 王大鹏, 等. 2009-2018年安丘市手足口病流行特征分析[J]. 预防医学论坛, 2019, 25(10): 779-781, 784. Yu CL, Li FY, Wang DP, et al. Analysis on epidemiological characteristics of hand, foot and mouth disease, Anqiu city, 2009-2018[J]. Prev Med Trib, 2019, 25(10): 779-781, 784. DOI:10.16406/j.pmt.issn.1672-9153.2019.10.018 |
| [76] |
陈婷, 汤洪洋, 潘利花, 等. 2008-2019年南宁市手足口病暴发疫情流行特征分析[J]. 现代预防医学, 2021, 48(2): 206-209. Chen T, Tang HY, Pan LH, et al. Analysis of the epidemiological characteristics of hand-foot-and-mouth disease outbreaks in Nanning, 2008-2019[J]. Mod Prev Med, 2021, 48(2): 206-209. |
| [77] |
Zhang Z, Liu Y, Liu FF, et al. Basic reproduction number of enterovirus 71 and coxsackievirus A16 and A6:Evidence from outbreaks of hand, foot, and mouth disease in China between 2011 and 2018[J]. Clin Infect Dis, 2021, 73(9): e2552-2559. DOI:10.1093/CID/CIAA1853 |
| [78] |
苏杏冰, 梁文靖, 陈纯. 2015-2018年广州市番禺区手足口病流行特征[J]. 热带医学杂志, 2020, 20(4): 567-569. Su XB, Liang WJ, Chen C. Epidemiological feature of hand-foot-and-mouth disease in Panyu district of Guangzhou city from 2015 to 2018[J]. J Trop Med, 2020, 20(4): 567-569. DOI:10.3969/j.issn.1672-3619.2020.04.034 |
| [79] |
何绍青, 李继军, 陈辉, 等. 2008-2017年昆明市手足口病流行特征分析[J]. 中国卫生产业, 2019, 16(19): 162-164, 168. He SC, Li JJ, Chen H, et al. Epidemiological characteristics of hand-foot-mouth disease in Kunming city from 2008 to 2017[J]. China Health Ind, 2019, 16(19): 162-164, 168. DOI:10.16659/j.cnki.1672-5654.2019.19.162 |
| [80] |
胡艳红, 颜慧敏. 长沙市岳麓区2014-2018年手足口病流行病学特征和病原学监测结果分析[J]. 中国社区医师, 2019, 35(28): 175-177. Hu YH, Yan HM. Epidemiological characteristics and pathogenic monitoring results of hand-foot-mouth disease in Yuelu district of Changsha city from 2014 to 2018[J]. Chin Community Doct, 2019, 35(28): 175-177. DOI:10.3969/j.issn.1007-614x.2019.28.119 |
| [81] |
苏杏冰, 梁文靖, 陈纯. 2015-2018年广州市番禺区手足口病流行特征[J]. 热带医学杂志, 2020, 20(4): 567-569. Su YB, Liang WJ, Chen C. Epidemiological feature of hand-foot-and-mouth disease in Panyu district of Guangzhou city from 2015 to 2018[J]. J Trop Med, 2020, 20(4): 567-569. DOI:10.3969/j.issn.1672-3619.2020.04.034 |
| [82] |
杨克江, 许玲玉, 李婷婷, 等. 2014-2018年昆明市官渡区手足口病流行特征分析[J]. 职业与健康, 2020, 36(12): 1650-1654. Yang KJ, Xu LY, Li TT, et al. Analysis on epidemic characteristics of hand-foot-mouth disease in Guandu district of Kunming city from 2014 to 2018[J]. Occup Health, 2020, 36(12): 1650-1654. DOI:10.13329/j.cnki.zyyjk.2020.0441 |
| [83] |
熊田甜, 李苑, 陈亿雄, 等. 2013-2016年深圳市宝安区手足口病流行病学特征分析[J]. 河南预防医学杂志, 2018, 29(4): 306-308. Xiong TT, Li Y, Chen YX, et al. Epidemiological analysis on hand-foot-mouth disease in Baoan district of Shenzhen, 2013-2016[J]. Henan J Prev Med, 2018, 29(4): 306-308. DOI:10.13515/j.cnki.hnjpm.1006-8414.2018.04.021 |
| [84] |
杨吉星, 忻郦菁, 李童, 等. 2009-2018年虹口区手足口病流行病学及病原学特征分析[J]. 热带医学杂志, 2020, 20(10): 1359-1362. Yang JX, Qi LJ, Li T, et al. Epidemiological and etiological characteristics of hand-foot-mouth disease in Hongkou district, 2009-2018[J]. J Trop Med, 2020, 20(10): 1359-1362. DOI:10.3969/j.issn.1672-3619.2020.10.026 |
| [85] |
潘蓓, 韩雅琳, 董礼艳, 等. 2009-2013年青岛市成人手足口病流行特征分析[J]. 预防医学论坛, 2018, 24(2): 127-129. Pan B, Han YL, Dong LY, et al. Analysis on epidemiological characteristics of hand-foot-mouth disease among adults Qingdao city, 2009-2013[J]. Prev Med Trib, 2018, 24(2): 127-129. DOI:10.16406/j.pmt.issn.1672-9153.2018.02.015 |
| [86] |
王海健, 陈虹, 何苗苗, 等. 上海市宝山区托幼机构2015-2017年手足口病流行特征分析[J]. 中国学校卫生, 2019, 40(8): 1251-1253. Wang HJ, Chen H, He MM, et al. The epidemiological characteristics of hand, foot, and mouth disease of Kindergarten in Baoshan district of Shanghai city from 2015 to 2017[J]. Chin J School Heal, 2019, 40(8): 1251-1253. DOI:10.16835/j.cnki.1000-9817.2019.08.037 |
| [87] |
王美芬, 符甜甜, 罗云娇, 等. 2008-2017年昆明地区住院手足口病患儿的临床特征研究[J]. 中国全科医学, 2021, 24(11): 1410-1417. Wang MF, Fu TT, Luo YJ, et al. Clinical characteristics of hospitalized children with hand-foot-mouth disease in Kunming from 2008 to 2017[J]. Chin General Pract, 2021, 24(11): 1410-1417. DOI:10.12114/j.issn.1007-9572.2020.00.475 |
| [88] |
Yan X, Zhang ZZ, Yang ZH, et al. Clinical and etiological characteristics of atypical hand-foot-and-mouth disease in children from Chongqing, China: A retrospective study[J]. BioMed Res Int, 2015, 2015: 802046. DOI:10.1155/2015/802046 |
| [89] |
Zhao TS, Du J, Sun DP, et al. A review and meta-analysis of the epidemiology and clinical presentation of coxsackievirus A6 causing hand-foot-mouth disease in China and global implications[J]. Rev Med Virol, 2020, 30(2): e2087. DOI:10.1002/rmv.2087 |
| [90] |
张钟, 郑亚明, 姜黎黎, 等. 我国2015-2016年哨点监测手足口病病原学和并发症分析[J]. 中华流行病学杂志, 2019, 40(6): 627-632. Zhang Z, Zheng YM, Jiang LL, et al. Review on the etiology and complications of hand, foot and mouth disease, using data from the national sentinel surveillance program, in China, 2015-2016[J]. Chin J Epidemiol, 2019, 40(6): 627-632. DOI:10.3760/cma.j.issn.0254-6450.2019.06.005 |
| [91] |
张静, 靳妍, 孙军玲, 等. 手足口病重症病例临床分期与结局分析[J]. 中华流行病学杂志, 2017, 38(5): 651-655. Zhang J, Jin Y, Sun JL, et al. Clinical stages and outcomes of severe cases on hand, foot and mouth disease[J]. Chin J Epidemiol, 2017, 38(5): 651-655. DOI:10.3760/cma.j.issn.0254-6450.2017.05.019 |
| [92] |
李亚萍, 翟嵩, 李梅, 等. 中性粒细胞/淋巴细胞比值与手足口病患儿重症化的相关性[J]. 中华实验和临床感染病杂志: 电子版, 2018, 12(6): 559-564. Li YP, Zhai S, Li M, et al. Neutrophil-lymphocyte ratio as a prognostic factor in severe hand, foot and mouth disease[J]. Chin J Exp Clin Infect Dis: Elect Vers, 2018, 12(6): 559-564. DOI:10.3877/cma.j.issn.1674-1358.2018.06.008 |
| [93] |
Zhou FY, Chen XQ, Chen GX, et al. Identification of SAA and ACTB as potential biomarker of patients with severe HFMD using iTRAQ quantitative proteomics[J]. Clin Biochem, 2019, 67: 1-6. DOI:10.1016/j.clinbiochem.2019.02.011 |
| [94] |
胡青坡, 孙乔, 何纳, 等. 上海市浦东新区手足口病单次与重复感染病例流行病学特征分析[J]. 中华疾病控制杂志, 2014, 18(4): 363-365. Hu QP, Sun Q, He N, et al. Epidemiological analysis of single and repeated infections with hand-foot-mouth disease in Pudong New Area of Shanghai city[J]. Chin J Dis Control Prev, 2014, 18(4): 363-365. |
| [95] |
高帆, 胡亚林, 孙世洋, 等. 我国婴幼儿人群中6种肠道病毒血清流行病学研究[J]. 中国病毒病杂志, 2018, 8(6): 501-508. Gao F, Hu YL, Sun SY, et al. Seroepidemiology of six enteroviruses among infants and children in China[J]. Chin J Viral Dis, 2018, 8(6): 501-508. DOI:10.16505/j.2095-0136.2018.0106 |
| [96] |
赵仕勇, 林先耀, 滕淑, 等. 肠道病毒71型感染手足口病患儿的肠道排毒时间及传播机制的初步探讨[J]. 疾病监测, 2015, 30(1): 23-26. Zhao SY, Lin XY, Teng S, et al. Survey of virus shedding and spread mechanism in children infected with EV71[J]. Dis Surveill, 2015, 30(1): 23-26. DOI:10.3784/j.issn.1003-9961.2015.01.007 |
| [97] |
Zhou YJ, Niu XD, Ding YQ, et al. Prevalence of recessive infection of pathogens of hand, foot, and mouth disease in healthy people in China[J]. Medicine, 2021, 100(7): e24855. DOI:10.1097/MD.0000000000024855 |
| [98] |
谢燕, 夏利, 袁娟. 陕西省西安地区手足口病隐性感染状况调查研究[J]. 实用临床医药杂志, 2019, 23(15): 45-47, 52. Xie Y, Xia L, Yuan J. Investigation on inapparent infection status of hand-foot-mouth disease in Xi'an city of Shaanxi province[J]. J Clin Med Pract, 2019, 23(15): 45-47, 52. DOI:10.7619/jcmp.201915012 |
| [99] |
孙昼, 谢立, 邓晶, 等. 杭州市儿童手足口病危险因素研究[J]. 疾病监测, 2010, 25(8): 606-608. Sun Z, Xie L, Deng J, et al. Risk factors of hand, foot and mouth disease among children in Hangzhou city[J]. Dis Surveill, 2010, 25(8): 606-608. DOI:10.3784/j.issn.1003-9961.2010.08.005 |
| [100] |
林先耀, 赵仕勇, 祁正红, 等. 不同类型肠道病毒感染所致手足口病流行病学调查[J]. 中国预防医学杂志, 2019, 20(7): 584-587. Lin XY, Zhao SY, Qi ZH, et al. Epidemiological characteristics of hand-foot-mouth disease caused by different types of enterovirus[J]. Chin Prevent Med, 2019, 20(7): 584-587. DOI:10.16506/j.1009-6639.2019.07.006 |
| [101] |
Liu JD, Chen Y, Hu PP, et al. Caregivers: the potential infection resources for the sustaining epidemic of hand, foot, and mouth disease/herpangina in Guangdong, China?[J]. Arch Public Health, 2021, 79: 54. DOI:10.1186/s13690-021-00574-8 |
| [102] |
Wang ZC, Liu T, Li JM, et al. Risk factors for hand, foot, and mouth disease caused by Coxsackievirus A6 in children under 6 years of age in Tianjin, China: a case-control study[J]. Jpn J Infect Dis, 2021, 74(5): 437-442. DOI:10.7883/yoken.JJID.2020.983 |
| [103] |
龙遗芳, 谭小华, 曾汉日, 等. 儿童聚集性场所肠道病毒污染现况调查[J]. 中国公共卫生, 2020, 36(7): 1080-1082. Long YF, Tang XH, Zeng HR, et al. Prevalence of enterovirus contamination in children's playgrounds, kindergartens and nurseries[J]. Chin J Public Health, 2020, 36(7): 1080-1082. DOI:10.11847/zgggws1121316 |
| [104] |
Ji H, Li L, Liu YM, et al. Seroepidemiology of human enterovirus71 and coxsackievirus A16 in Jiangsu province, China[J]. Virol J, 2012, 9: 248. DOI:10.1186/1743-422X-9-248 |
| [105] |
李亚萍, 翟嵩, 李梅, 等. TLR7基因rs3853839、rs179010多态性与EV71手足口病男性患儿易感性及病情严重程度相关[J]. 细胞与分子免疫学杂志, 2017, 33(7): 953-958. Li YP, Zhai S, Li M, et al. Polymorphisms of TLR7 rs3853839 and rs179010 are associated with susceptibility to and severity of hand, foot and mouth disease caused by enterovirus 71 in male children[J]. Chin J Cell Mol Immunol, 2017, 33(7): 953-958. DOI:10.13423/j.cnki.cjcmi.008197 |
| [106] |
李亚萍, 翟嵩, 王文俊, 等. OAS1基因多态性与儿童肠道病毒71型感染合并中枢神经系统受累相关[J]. 南方医科大学学报, 2019, 39(4): 381-386. Li YP, Zhai S, Wang WJ, et al. OAS1 gene polymorphism is associated with central nervous system involvement in children with enterovirus 71 infection[J]. J Southern Med Univ, 2019, 39(4): 381-386. DOI:10.12122/j.issn.1673-4254.2019.04.01 |
| [107] |
Meng Y, Xiong TT, Zhao RX, et al. Genome-wide association study identifies TPH2 variant as a novel locus for severe CV-A6-associated hand, foot, and mouth disease in Han Chinese[J]. Int J Infect Dis, 2020, 98: 268-274. DOI:10.1016/j.ijid.2020.06.104 |
| [108] |
王燕芬, 王旭峰, 赵继军. 中国部分省份手足口病传染率分析[J]. 中华疾病控制杂志, 2019, 23(5): 540-544. Wang YF, Wang XF, Zhao JJ. Analysis of transmission rate of hand-foot-mouth disease in different provinces in China[J]. Chin J Dis Control Prev, 2019, 23(5): 540-544. DOI:10.16462/j.cnki.zhjbkz.2019.05.010 |
| [109] |
Wang Y, Feng ZJ, Yang Y, et al. Hand, foot, and mouth disease in China: Patterns of spread and transmissibility[J]. Epidemiology, 2011, 22(6): 781-792. DOI:10.1097/EDE.0b013e318231d67a |
| [110] |
Xia F, Deng F, Tian H, et al. Estimation of the reproduction number and identification of periodicity for HFMD infections in northwest China[J]. J Theoret Biol, 2020, 484: 110027. DOI:10.1016/j.jtbi.2019.110027 |
| [111] |
Du ZC, Zhang WJ, Zhang DM, et al. Estimating the basic reproduction rate of HFMD using the time series SIR model in Guangdong, China[J]. PLoS One, 2017, 12(7): e179623. DOI:10.1371/journal.pone.0179623 |
| [112] |
Jiang Y, Xu J, Lai H, et al. Association between meteorological parameters and hand, foot and mouth disease in mainland China: A systematic review and meta-analysis[J]. Iran J Public Health, 2021, 50(9): 1757-1765. DOI:10.18502/ijph.v50i9.7046 |
| [113] |
景钦隆, 吴琦琳, 鲁影, 等. 手足口病流行与暴发的气象因素预警界值研究[J]. 中国预防医学杂志, 2019, 20(7): 579-583. Jing QL, Wu QL, Lu Y, et al. Studies on early warning threshold of meteorological parameters related to the epidemic and outbreak of hand-foot-mouth disease[J]. China Prev Med, 2019, 20(7): 579-583. DOI:10.16506/j.1009-6639.2019.07.005 |
| [114] |
Zhang WJ, Du ZC, Zhang DM, et al. Boosted regression tree model-based assessment of the impacts of meteorological drivers of hand, foot and mouth disease in Guangdong, China[J]. Sci Total Environ, 2016, 553: 366-371. DOI:10.1016/j.scitotenv.2016.02.023 |
| [115] |
Zhang Z, Xie X, Chen XL, et al. Short-term effects of meteorological factors on hand, foot and mouth disease among children in Shenzhen, China: Non-linearity, threshold and interaction[J]. Sci Total Environ, 2016, 539: 576-582. DOI:10.1016/j.scitotenv.2015.09.027 |
| [116] |
李媛丽, 程孝连, 梁寅生, 等. 蚌埠市2009-2018年手足口病流行特征及气象影响因素分析[J]. 安徽预防医学杂志, 2019, 25(6): 435-438. Li YL, Cheng XL, Liang YS, et al. Epidemiological characteristics and meteorological factors of hand, foot and mouth disease in Bengbu city from 2009 to 2018[J]. Anhui J Prev Med, 2019, 25(6): 435-438. |
| [117] |
Yang H, Wu J, Cheng J, et al. Is high relative humidity associated with childhood hand, foot, and mouth disease in rural and urban areas?[J]. Public Health, 2017, 142: 201-207. DOI:10.1016/j.puhe.2015.03.018 |
| [118] |
Wang C, Cao K, Zhang YJ, et al. Different effects of meteorological factors on hand, foot and mouth disease in various climates: a spatial panel data model analysis[J]. BMC Infect Dis, 2016, 16: 233. DOI:10.1186/s12879-016-1560-9 |
| [119] |
Liu WD, Ji H, Shan J, et al. Spatiotemporal dynamics of hand-foot-mouth disease and its relationship with meteorological factors in Jiangsu province, China[J]. PLoS One, 2015, 10(6): e0131311. DOI:10.1371/journal.pone.0131311 |
| [120] |
Liao JQ, Yu SC, Yang F, et al. Short-term effects of climatic variables on hand, foot, and mouth disease in mainland China, 2008-2013:A multilevel spatial poisson regression model accounting for overdispersion[J]. PLoS One, 2016, 11(1): e0147054. DOI:10.1371/journal.pone.0147054 |
| [121] |
Gui JJ, Liu ZF, Zhang TF, et al. Epidemiological characteristics and spatial-temporal clusters of hand, foot, and mouth disease in Zhejiang province, China, 2008-2012[J]. PLoS One, 2015, 10(9): e0139109. DOI:10.1371/journal.pone.0139109 |
| [122] |
Rui J, Luo KW, Chen QP, et al. Early warning of hand, foot, and mouth disease transmission: A modeling study in mainland, China[J]. PLoS Negl Trop Dis, 2021, 15(3): e0009233. DOI:10.1371/journal.pntd.0009233 |
| [123] |
Zhu FC, Meng FY, Li JX, et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial[J]. Lancet, 2013, 381(9882): 2024-2032. DOI:10.1016/S0140-6736(13)61049-1 |
| [124] |
Zhu FC, Xu WB, Xia JL, et al. Efficacy, safety, and immunogenicity of an enterovirus 71 vaccine in China[J]. N Engl J Med, 2014, 370(9): 818-828. DOI:10.1056/NEJMoa1304923 |
| [125] |
Li RC, Liu LD, Mo ZJ, et al. An inactivated enterovirus 71 vaccine in healthy children[J]. N Engl J Med, 2014, 370(9): 829-837. DOI:10.1056/NEJMoa1303224 |
| [126] |
王晓莉. 北京市手足口病疾病负担及其EV-A71疫苗接种效果的评价研究[D]. 北京: 中国疾病预防控制中心, 2019. Wang XL. Study on the burden of hand, foot, mouth disease and the effectiveness evaluation of the EV-A71 vaccination program in Beijing[D]. Beijing: Chinese Center for Disease Control and Prevention, 2019. |
| [127] |
Head JR, Collender PA, Lewnard JA, et al. Early evidence of inactivated enterovirus 71 vaccine impact against hand, foot, and mouth disease in a major center of ongoing transmission in China, 2011-2018:a longitudinal surveillance study[J]. Clin Infect Dis, 2020, 71(12): 3088-3095. DOI:10.1093/cid/ciz1188 |
| [128] |
Du ZC, Huang Y, Bloom MS, et al. Assessing the vaccine effectiveness for hand, foot, and mouth disease in Guangzhou, China: a time-series analysis[J]. Hum Vaccin Immunother, 2021, 17(1): 217-223. DOI:10.1080/21645515.2020.1763076 |
| [129] |
Shi L, Zhao HY, Wu DY, et al. Modelling and analysis of HFMD with the effects of vaccination, contaminated environments and quarantine in mainland China[J]. Math Biosci Eng, 2019, 16(1): 474-500. DOI:10.3934/mbe.2019022 |
| [130] |
杨芬, 梁文佳, 孙立梅, 等. 广东省EV71疫苗接种水平与手足口病流行分析[J]. 中国公共卫生, 2020, 36(3): 351-354. Yang F, Liang WJ, Sun LM, et al. Innoculation of enterorirus 71 vaccine and incidence of hand-foot-mouth disease in Guangdong province[J]. Chin J Public Health, 2020, 36(3): 351-354. DOI:10.11847/zgggws1119741 |
| [131] |
陈成连, 陈阿群, 李昕韵, 等. 2017-2019年江门市肠道病毒71型灭活疫苗接种水平与手足口病流行病学分析[J]. 华南预防医学, 2020, 46(4): 424-426. Chen CL, Chen AQ, Li XY, et al. Epidemiological analysis of hand, foot, and mouth disease and vaccination level of inactivated enterovirus 71 vaccine in Jiangmen, 2017-2019[J]. South China J Prev Med, 2020, 46(4): 424-426. DOI:10.12183/j.scjpm.2020.0424 |