 2022, Vol. 43
2022, Vol. 43文章信息
- 李若曈, 饶蓁蓁, 傅晏红, 徐婷玲, 刘江美, 于石成, 周脉耕, 董文兰, 胡国清.
- Li Ruotong, Rao Zhenzhen, Fu Yanhong, Xu Tingling, Liu Jiangmei, Yu Shicheng, Zhou Maigeng, Dong Wenlan, Hu Guoqing
- 2030年中国慢性阻塞性肺疾病的疾病负担预测与危险因素控制效果模拟
- Prediction on the burden of disease of chronic obstructive pulmonary disease and simulation of the effectiveness of controlling risk factors in China by 2030
- 中华流行病学杂志, 2022, 43(2): 201-206
- Chinese Journal of Epidemiology, 2022, 43(2): 201-206
- http://dx.doi.org/10.3760/cma.j.cn112338-20210803-00606
-
文章历史
收稿日期: 2021-08-03




2. 中国疾病预防控制中心慢性非传染性疾病预防控制中心, 北京 100050;
3. 中国疾病预防控制中心, 北京 102206;
4. 中南大学湘雅医院国家老年疾病临床医学研究中心, 长沙 410078
2. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
3. Chinese Center for Disease Control and Prevention, Beijing 102206, China;
4. National Clinical Research Center for Geriatric Disorders, Xiangya Hospital, Central South University, Changsha 410078, China
慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)是一种以持续气流受限为特征的可以预防和治疗的常见慢性呼吸系统疾病[1]。全球疾病负担研究(Global Burden of Disease Study,GBD)2019年估算数据显示[2],COPD在我国共造成104万人死亡,位居死因排行第三位。COPD的发病与导致持续气流受限的因素密切相关,研究证据显示,吸烟、职业暴露以及室内外空气污染均与COPD发病相关[3]。COPD患病率高,常反复发作,严重影响患者的生活质量,给患者及其家庭以及社会带来了沉重的经济负担[4]。《“健康中国2030”规划纲要》[5]、《中国防治慢性病中长期规划(2017-2025年)》[6]等行动计划均对慢性呼吸系统疾病提出了明确的防控目标。而COPD作为主要慢性呼吸系统疾病,预测2030年我国COPD的疾病负担,将有助于对上述行动计划的顺利实施提供参考;针对COPD相关的危险因素,基于暴露水平的人群死亡情况预测和调控,可进一步为有效防控策略的制定与实施提供指导,提升COPD防治能力和水平。目前针对我国COPD的疾病负担预测研究仅纳入吸烟这一相关危险因素[7],但证据显示环境颗粒物污染也与COPD死亡风险升高有关[8-10]。为此,本研究基于1990-2015年中国COPD所致总死亡数与危险因素暴露数据,在现有的防控策略和危险因素控制目标下,预测2030年COPD所致疾病负担,为主动防控COPD提供参考。
资料与方法1. 数据来源:选取GBD2015年中国分疾病负担研究中数据进行预测和分析[11],主要包括:①1990-2015年COPD死亡数(国际疾病分类第10版编码:J40~J44);②危险因素暴露数据[12]:吸烟率,室外空气动力学直径 < 2.5 μm的颗粒物(PM2.5)年平均浓度(μg/m³),在分析中纳入1990年与2015年数据;③COPD与吸烟、PM2.5污染的相对危险度(RR)主要基于文献综述与Meta分析确定。计算死亡率和过早死亡概率所需的人口数由项目牵头单位协调获取数据。本研究通过中南大学湘雅公共卫生学院伦理委员会审查(批准文号:XYGW- 2021-42)。
2. 数据分析:
(1)预测场景假设:基于WHO全球非传染性疾病预防控制综合监测框架(含指标)和自愿性目标[13]、国民经济和社会发展第十四个五年规划和2035年远景目标纲要[14]以及暴露数据的可及性,纳入与COPD相关的2种危险因素:吸烟和PM2.5污染,并根据相应控制目标,模拟2030年2种不同危险因素的暴露水平控制程度的4种场景(表 1)。

(2)人群归因分值(population attributable fraction,PAF)计算:基于比较风险评估(comparative risk assessment)理论框架[16-17],根据各危险因素暴露水平和RR值估计中国1990-2015年和2030年COPD总死亡数中有多少比例是由某种危险因素导致的,计算各种场景假设下归因于各类危险因素的PAF与联合PAF[17]。
(3)COPD死亡例数估算:在PAF的基础上,计算可归因死亡数(AM)与不可归因死亡数(UM),公式为:AM=M×PAF;UM=M-AM。其中,M为总死亡数;采用比例变化模型[15],根据1990-2015年分性别、年龄组各类疾病的UM估计出2030年的UM,再由此估算总死亡数,公式:
 (1)
(1)
s为性别,a为年龄组,d为疾病。2030年各种场景下各类疾病分性别、年龄组的死亡总数为:
 (2)
(2)
s为性别,a为年龄组,d为疾病,fj为第j个危险因素,n为疾病相关危险因素个数,sc为2030年设置的各种场景。
(4)死亡率、标化死亡率和过早死亡概率计算:在不同模拟场景下,利用所预测的2030年不同年龄、性别组疾病死亡数,结合中国人口与发展研究中心对我国2030年人口数的估计值,可计算分年龄、性别的各类COPD死亡率。采用2010年中国第六次人口普查结构对2015年和2030年的死亡率进行标化。过早死亡概率定义为30~70岁的人群死于COPD的概率。通过寿命表法,利用年龄别死亡率估算过早死亡概率。所有数据分析均在R 3.6.1软件中实现。
结果1. 自然趋势下2030年中国COPD疾病负担:
(1)死亡情况:按照1990-2015年危险因素的自然趋势估算,2030年中国COPD的死亡例数为105.54万例,相比2015年(91.13万例)上升15.81%,占慢性呼吸系统疾病总死亡例数的95.42%;预计2030年死亡率为73.85/10万,相比于2015年(66.71/10万)上升10.69%;预计2030年标化死亡率(33.81/10万)较2015年(55.32/10万)降低38.88%。
不同性别间的预测结果显示,2030年男性COPD死亡例数和死亡率均高于女性(死亡例数:61.65万例vs. 43.89万例,死亡率:84.35/10万vs. 62.86/10万),较2015年均呈上升趋势,但女性上升幅度高于男性;2030年男性慢性呼吸系统疾病标化死亡率高于女性(44.23/10万vs. 24.69/10万),且均呈下降趋势,男性下降幅度高于女性(表 2)。

(2)过早死亡情况:2030年中国30~70岁人群COPD过早死亡概率将由2015年的1.49%降至0.71%,降幅达52.73%(图 1)。

|
| 注:1990-2015年为GBD2015原始数据,2020-2030年为模型估算的数值 图 1 1990-2030年各场景下中国30~70岁人群慢性阻塞性肺疾病过早死亡概率变化趋势 |
其中,2030年女性COPD过早死亡概率为0.37%,低于男性的1.04%,且女性降低幅度高于男性(60.02% vs. 49.32%)(图 2,3)。

|
| 注:1990-2015年为GBD2015原始数据,2020-2030年为模型估算的数值 图 2 1990-2030年各场景下中国男性30~70岁人群慢性阻塞性肺疾病过早死亡概率变化趋势 |

|
| 注:1990-2015年为GBD2015原始数据,2020-2030年为模型估算的数值 图 3 1990-2030年各场景下中国女性30~70岁人群慢性阻塞性肺疾病过早死亡概率变化趋势 |
2. 危险因素控制场景假设下2030年中国COPD疾病负担:
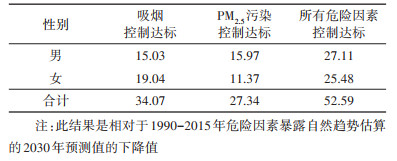
(1)死亡情况:若2030年各年龄段男女性吸烟率比2015年下降30%,COPD的死亡例数将较自然趋势减少34.07万例(男性15.03万例,女性19.04万例)。
若2030年24 h PM2.5平均浓度比2015年降低10%,将减少27.34万例COPD死亡(男性15.97万例,女性11.37万例)。
如果所有危险因素控制达标,2030年可避免52.59万例COPD死亡(男性27.11万例,女性25.48万例)(表 3)。
(2)过早死亡情况:吸烟控制达标将使2030年中国30~70岁人群COPD过早死亡概率由自然趋势的0.71%降至0.59%(图 1),男性降幅高于女性(19.43% vs. 8.69%)(图 2,3);PM2.5污染控制达标可使过早死亡概率降至0.52%;所有危险因素控制达标,到2030年可使过早死亡概率降至0.44%(图 1)。
讨论本研究结果显示,如吸烟率、PM2.5污染控制达标,相较于自然趋势,2030年可避免52.59万例COPD死亡,可将COPD过早死亡概率由自然趋势的0.71%降至0.44%,其中吸烟控制达标减少COPD死亡数高于PM2.5污染控制达标。
与既往研究预测结果相比[7, 18],未来COPD死亡趋势较为一致。《中国防治慢性病中长期规划(2017-2025年)》[6]提出的目标为到2025年30~70岁人群因慢性呼吸系统疾病导致的过早死亡概率较2015年降低20%的目标,《“健康中国2030”规划纲要》中提出的目标为到2030年重大慢性病过早死亡概率较2015年下降30%的目标[5]。研究结果表明,按照目前危险因素暴露水平和疾病负担趋势变化,基于COPD的上述防控目标将得以实现。
人口老龄化、预期寿命的延长和COPD诊疗水平的提高是导致自然趋势下2030年COPD的死亡数和死亡率升高但标化死亡率与过早死亡概率下降的重要原因。由于不同年龄段COPD发病风险与死亡风险有明显差别,COPD所导致死亡大多发生在老年人群中。因此,除了吸烟和PM2.5污染的影响,近年来不断加剧的人口老龄化趋势也是导致2030年COPD死亡数和死亡率较2015年上升的原因之一;而过早死亡概率仅涉及30~70岁人群,与标化死亡率均呈现下降趋势主要与预期寿命延长和COPD诊治水平提升密切相关。目前我国已步入老龄化社会,人口老龄化速度较快,老年人口数量和老年人口比例不断攀升,证据显示COPD患病率随年龄增大而升高[19],COPD是慢性呼吸系统疾病中的主要疾病,人口老龄化的加剧无疑对COPD防控提出了新的要求。进一步加强对重点人群的COPD早期筛查、实现分期分级规范治疗、完善对COPD患者的社区管理对减少老年人群中的COPD死亡人数至关重要[20]。
吸烟是COPD的主要危险因素。针对不同场景的预测结果提示,吸烟控制达标将显著降低2030年COPD导致的死亡与过早死亡。但目前我国控烟形势严峻,《2015中国成人烟草调查报告》显示[21],人群吸烟率与2010年基本持平,日均吸烟量增加1支。我国目前仍未出台国家层面的控烟法,烟草广告和促销现状非常普遍,烟草税收较其他国家依然处于较低水平[22]。如何基于证据实施强力控烟措施来降低人群吸烟率,是降低COPD负担的关键所在。空气污染也与COPD的发病密切相关。一项利用GBD2017估算数据的研究显示[23],40.0%的COPD所致的伤残调整生命年可归因于空气污染。2017年我国《大气污染防治行动计划》目标如期实现,大气污染状况得到了有效控制,将有助于减少COPD死亡人数。
受数据可及性与预测模型限制,本研究将死亡作为疾病负担指标,预测未来我国COPD标化死亡率与过早死亡概率将进一步降低。由于COPD病程较长,在过早死亡概率降低的情况下如何延缓COPD患者肺功能恶化,提高患者生活质量将成为未来降低COPD所致健康危害的关键。建议加强COPD的健康教育与促进,探索新的干预手段,提高COPD诊断治疗与规范化管理的水平,尽可能保障COPD患者获得质量较高的医疗服务[24-25]。
自GBD2015后,GBD课题组不再对外公布危险因素原始暴露水平的数据,故本研究只能基于既往1990-2015年的危险因素暴露变化趋势进行预测,预测所需危险因素暴露水平、COPD死亡数据及危险因素与疾病关联均来源于GBD2015中1990-2015年中国数据。采用比例变化模型进行预测,该方法对危险因素的未来趋势预测反映了1990-2015年危险因素暴露长期趋势下的变化[15]。考虑到近期危险因素暴露数据不可及与长期预测结果可能存在的很大不确定性,故本研究仅预测至2030年。本研究纳入与COPD相关的2个危险因素即吸烟与PM2.5污染,其中,GBD2015估计吸烟率数据采用来源于国际吸烟统计数据库(International Smoking Statistics Database)等有全国代表性的调查数据[12];GBD2015估计PM2.5浓度主要基于卫星观测大气中的气溶胶得到的PM2.5年浓度的估计,并构建框架将模拟浓度与地面监测结果结合起来以调整卫星建模方法中的偏差[12],尽管GBD估计值采用复杂模型来降低原始数据的缺失和低质量的影响,但仍可能存在一定的不确定性。此外,受目前数据资源的可及性影响,本研究未能纳入除吸烟与PM2.5污染外如医疗卫生服务状况等其他危险因素。如未来证实的相关危险因素暴露数据可获得,课题组将在本研究基础上纳入这些新报告的因素,进一步完善预测模型。
利益冲突 所有作者声明无利益冲突
作者贡献声明 李若曈:研究设计、数据整理、统计学分析、论文撰写;饶蓁蓁、傅晏红、徐婷玲、刘江美:数据整理、论文修改;于石成、周脉耕、董文兰、胡国清:研究指导、论文修改、经费支持
| [1] |
中华医学会, 中华医学会杂志社, 中华医学会全科医学分会, 等. 慢性阻塞性肺疾病基层诊疗指南(2018年)[J]. 中华全科医师杂志, 2018, 17(11): 856-870. Chinese Medical Association, Journal of the Chinese Medical Association, Chinese Society of General Practice, et al. Guideline for primary care of chronic obstructive pulmonary disease (2018)[J]. Chin J General Practit, 2018, 17(11): 856-870. DOI:10.3760/cma.j.issn.1671-7368.2018.11.002 |
| [2] |
Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease (GBD) data visualizations[EB/OL]. [2021-03-11]. http://www.healthmetricsandevaluation.org/gbd/visualizations/country.
|
| [3] |
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease 2020 report[EB/OL]. [2021-03-11]. https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf.
|
| [4] |
中华医学会呼吸病学分会慢性阻塞性肺疾病学组, 中国医师协会呼吸医师分会慢性阻塞性肺疾病工作委员会. 慢性阻塞性肺疾病诊治指南(2021年修订版)[J]. 中华结核和呼吸杂志, 2021, 44(3): 170-205. Group on Chronic Obstructive Pulmonary Disease, Chinese Thoracic Society, Committee on Chronic Obstructive Pulmonary Disease, Chinese Association of Chest Physicians. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021)[J]. Chin J Tubercul Respirat Dis, 2021, 44(3): 170-205. DOI:10.3760/cma.j.cn112147-20210109-00031 |
| [5] |
新华社. 中共中央国务院印发《"健康中国2030"规划纲要》[EB/OL]. (2016-10-25) [2021-03-11]. http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm.
|
| [6] |
国务院办公厅. 国务院办公厅关于印发中国防治慢性病中长期规划(2017-2025年)的通知[EB/OL]. (2017-02-14) [2020-03-11]. http://www.gov.cn/zhengce/content/2017-02/14/content_5167886.htm.
|
| [7] |
曾新颖, 李镒冲, 刘江美, 等. 危险因素控制对2030年中国慢性病死亡、期望寿命和劳动力损失的影响估计[J]. 中华预防医学杂志, 2017, 51(12): 1079-1085. Zeng XY, Li YC, Liu JM, et al. Estimation of the impact of risk factors control on non-communicable diseases mortality, life expectancy and the labor force lost in China in 2030[J]. Chin J Prev Med, 2017, 51(12): 1079-1085. DOI:10.3760/cma.j.issn.0253-9624.2017.12.006 |
| [8] |
Faustini A, Stafoggia M, Cappai G, et al. Short-term effects of air pollution in a cohort of patients with chronic obstructive pulmonary disease[J]. Epidemiology, 2012, 23(6): 861-879. DOI:10.1097/EDE.0b013e31826767c2 |
| [9] |
Li MH, Fan LC, Mao B, et al. Short-term exposure to ambient fine particulate matter increases hospitalizations and mortality in COPD: a systematic review and meta-analysis[J]. Chest, 2016, 149(2): 447-458. DOI:10.1378/chest.15-0513 |
| [10] |
Li GX, Huang J, Xu GZ, et al. The short term burden of ambient fine particulate matter on chronic obstructive pulmonary disease in Ningbo, China[J]. Environ Health, 2017, 16(1): 54. DOI:10.1186/s12940-017-0253-1 |
| [11] |
Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease (GBD) GBD results tool[EB/OL]. [2020-03-11]. http://ghdx.healthdata.org/gbd-results-tool.
|
| [12] |
GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015:a systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet, 2016, 388(10053): 1659-1724. DOI:10.1016/S0140-6736(16)31679-8 |
| [13] |
世界卫生组织. 全球非传染性疾病预防控制综合监测框架(含指标)和自愿性目标[EB/OL]. (2012-07-25) [2021-03-11]. http://www.who.int/nmh/events/2012/Discussion_paper3_CH.pdf?ua=1.
|
| [14] |
新华社. 中华人民共和国国民经济和社会发展第十四个五年规划和2035年远景目标纲要[EB/OL]. (2021-03-13) [2021-03-20]. http://www.gov.cn/xinwen/2021-03/13/content_5592681.htm.
|
| [15] |
Roth GA, Nguyen G, Forouzanfar MH, et al. Estimates of global and regional premature cardiovascular mortality in 2025[J]. Circulation, 2015, 132(13): 1270-1282. DOI:10.1161/CIRCULATIONAHA.115.016021 |
| [16] |
Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet, 2012, 380(9859): 2224-2260. DOI:10.1016/S0140-6736(12)61766-8 |
| [17] |
Murray CJL, Ezzati M, Lopez AD, et al. Comparative quantification of health risks: Conceptual framework and methodological issues[J]. Popul Health Metr, 2003, 1(1): 1. DOI:10.1186/1478-7954-1-1 |
| [18] |
Li YC, Zeng XY, Liu JM, et al. Can China achieve a one-third reduction in premature mortality from non-communicable diseases by 2030?[J]. BMC Med, 2017, 15(1): 132. DOI:10.1186/s12916-017-0894-5 |
| [19] |
包鹤龄, 方利文, 王临虹. 1990-2014年中国40岁及以上人群慢性阻塞性肺疾病患病率Meta分析[J]. 中华流行病学杂志, 2016, 37(1): 119-124. Bao HL, Fang LW, Wang LH. Prevalence of chronic obstructive pulmonary disease among community population aged ≥40 in China: a Meta-analysis on studies published between 1990 and 2014[J]. Chin J Epidemiol, 2016, 37(1): 119-124. DOI:10.3760/cma.j.issn.0254-6450.2016.01.026 |
| [20] |
康健, 文富强. 从医保数据分析中国慢性阻塞性肺疾病管理的不足[J]. 中华结核和呼吸杂志, 2017, 40(12): 884-886. Kang J, Wen FQ. Analysis of COPD management in China based on health insurance data[J]. Chin J Tuberc Respir Dis, 2017, 40(12): 884-886. DOI:10.3760/cma.j.issn.1001-0939.2017.12.002 |
| [21] |
杨焱, 南奕, 屠梦吴, 等. 《2015中国成人烟草调查报告》概要[J]. 中华健康管理学杂志, 2016, 10(2): 85-87. Yang Y, Nan Y, Tu MW, et al. Major finding of 2015 China adults tobacco survery[J]. Chin J Health Manag, 2016, 10(2): 85-87. DOI:10.3760/cma.j.issn.1674-0815.2016.02.002 |
| [22] |
邹小农, 贾漫漫, 王鑫, 等. 中国肺癌和烟草流行及控烟现状[J]. 中国肺癌杂志, 2017, 20(8): 505-510. Zou XN, Jia MM, Wang X, et al. Changing epidemic of lung cancer & tobacco and situation of tobacco control in China[J]. Chin J Lung Cancer, 2017, 20(8): 505-510. DOI:10.3779/j.issn.1009-3419.2017.08.01 |
| [23] |
Yin P, Brauer M, Cohen AJ, et al. The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990-2017:an analysis for the Global Burden of Disease Study 2017[J]. Lancet Planet Health, 2020, 4(9): e386-398. DOI:10.1016/S2542-5196(20)30161-3 |
| [24] |
王辰. 中国18个地市慢性阻塞性肺疾病诊疗报告[M]. 北京: 人民卫生出版社, 2020. Wang C. Diagnosis and treatment report of chronic obstructive pulmonary disease in 18 cities in China[M]. Beijing: People's Medical Publishing House, 2020. |
| [25] |
方晓聪, 王向东, 白春学. 慢性阻塞性肺疾病在中国的诊治现状[J]. 国际呼吸杂志, 2011, 31(7): 493-497. Fang XC, Wang XD, Bai CX. Burden and importance of proper management about chronic obstructive pulmonary disease in China[J]. Int J Respir, 2011, 31(7): 493-497. DOI:10.3760/cma.j.issn.1673-436X.2011.007.004 |