 2021, Vol. 42
2021, Vol. 42文章信息
- 张佩雯, 张辉, 李明爽, 林艺丹, 孙静, 林孟波, 刘远立.
- Zhang Peiwen, Zhang Hui, Li Mingshuang, Lin Yidan, Sun Jing, Lin Mengbo, Liu Yuanli
- 基于医患双方的女性早期乳腺癌选择保乳手术的影响因素研究
- Factors associated with selection of breast-conserving surgery in early female patients with breast cancer
- 中华流行病学杂志, 2021, 42(11): 2044-2052
- Chinese Journal of Epidemiology, 2021, 42(11): 2044-2052
- http://dx.doi.org/10.3760/cma.j.cn112338-20210516-00402
-
文章历史
收稿日期: 2021-05-16




2. 福建省立医院肿瘤外科, 福州 350001;
3. 中国医学科学院北京协和医学院群医学与公共卫生学院, 北京 100710
2. Department of Oncology Surgery, Fujian Provincial Hospital, Fuzhou 350001, China;
3. School of Population Medicine and Public Health, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100710, China
2020年女性乳腺癌已超过肺癌成为全球癌症发病率的首要原因,也是癌症死亡的第五大原因[1]。我国女性乳腺癌年龄标化发生率为391例/万人[2],疾病负担呈逐年加重趋势。目前,常规乳腺癌手术方式包括乳房切除术(mastectomy)和保乳手术(breast-conserving surgery,BCS)[3]。乳房切除术中最常见的改良根治术除了切除整个乳房,有的还要清扫腋窝淋巴结。术后身体缺损和形体改变常使患者自信心下降,甚至发生焦虑和抑郁,影响生活质量[4]。保乳手术范围较小,可更好地保持女性形体[5-7]。国内外大量长期随访结果证明,早期乳腺癌女性患者保乳手术联合放疗的远期生存率及局部复发率不劣于乳房切除手术[8-12]。保乳手术已成为多数Ⅰ期和Ⅱ期乳腺癌女性患者的适宜治疗方法[13],在发达国家广泛应用。但我国保乳手术的临床实践还处于起步阶段[14-15],开展率较低。不仅有医疗技术水平的原因,还与卫生体系和医患双方的社会文化及经济发展等复杂因素有关。现有研究显示,患者的肿瘤大小、年龄、文化程度、收入[16-19]、个人的保乳意愿以及对治疗信息的掌握等因素[20-23]会影响乳腺癌患者的手术决策。术后放疗的便利性和由此带来的个人经济负担[24-25]也是影响患者手术决策的重要因素。医生在患者的手术决策中发挥重要作用[26],女医生、手术量大和肿瘤专科医生更倾向于选择保乳手术[27-28]。目前,欧美等发达国家开展对早期乳腺癌女性患者手术方式决策的研究较多,国内有限的研究大多集中于患者层面的分析,缺少对医生层面的分析及医患双方影响因素的综合考量。本研究基于一个省级医学中心的临床资料,结合医生调查和患者访谈,从医患双方全面地分析早期乳腺癌女性患者手术方式决策的影响因素,旨在为有效引导医患双方对早期乳腺癌女性患者的循证手术决策提供证据。
对象与方法1. 研究对象:2015年1月1日至2019年12月31日在福建省立医院确诊并接受手术治疗、符合保乳手术指征的早期乳腺癌女性患者。根据《中国抗癌协会乳腺癌诊治指南与规范》[29]及临床经验确定研究对象的纳入标准:①术前病理确诊为浸润性乳腺癌;②根据美国癌症联合委员会第8版分期标准[30]符合临床分期Ⅰ或Ⅱ期的早期乳腺癌;③女性;④临床资料完整。排除标准:①复发或发生远处转移者;②患结缔组织疾病、严重精神疾病、其他恶性肿瘤或严重器质性疾病者;③既往接受过乳腺癌手术治疗的患者;④肿瘤较大(直径 > 5 cm)影响保乳手术后美观的患者;⑤乳腺癌家族史;⑥无法追溯调查主治医生的患者(根据患者的病案首页确定其主治医生作为调查对象,若该项未写明则选择该患者的手术医生作为调查对象)。研究观察期内,我国乳腺癌诊疗指南未有显著变化,研究医院也未出台任何与保乳手术选择相关的推进政策和开展其他干预项目,适宜保乳患者选择保乳手术的比例并未有显著改变。根据纳入排除标准确定研究对象共566例。
2. 研究方法:
(1)通过医院信息系统获得研究对象的病案信息,根据国内外文献确定需要提取的患者相关指标[16-25],包括患者年龄、居住地、医保类型及肿瘤大小、淋巴结转移、手术名称和编码等资料。
(2)采用电子问卷收集目标患者主治医生的相关资料。在医务管理部门的帮助下,发送电子问卷链接给目标医生,邀请其自填作答。电子问卷的设计参照文献[21, 27-28],内容包括目标医生的人口和社会学特征、乳腺癌临床诊疗经验及医生认为影响患者手术方式决策的因素等。
(3)由3名研究团队成员于2020年10月21-28日分别对肿瘤外科的15例早期乳腺癌术后女性患者进行知情同意后的半结构化访谈。通过住院患者访谈,了解早期乳腺癌女性患者手术方式决策中的主要考量。参考相关文献制订访谈提纲[21],了解患者手术方式决策的过程、主要原因以及医生推荐程度等。
3. 研究变量:
(1)患者的临床特征:包括肿瘤大小、淋巴结转移、月经状态以及手术名称及编码。根据国际疾病分类第九临床修订版(The International Classification of Diseases,Clinical Modification of,9th Revision)对与手术相关的患者进行识别和分类。若患者接受的手术名称为节段乳房切除术、肿块切除术、象限切除术、切除活检或部分乳房切除术中的任何一项,认定该患者为保乳手术患者;如果患者接受的手术中包含改良根治术、单纯/根治乳房切除术中的任何一项,将其归类为乳房切除术患者。根据文献[31],对先接受肿块切除手术,并在术后2个月内再次接受乳房切除手术的患者,认定为乳房切除术患者;间隔时间 > 2个月的,按首次手术认定为保乳手术患者,第二次手术不再纳入分析。
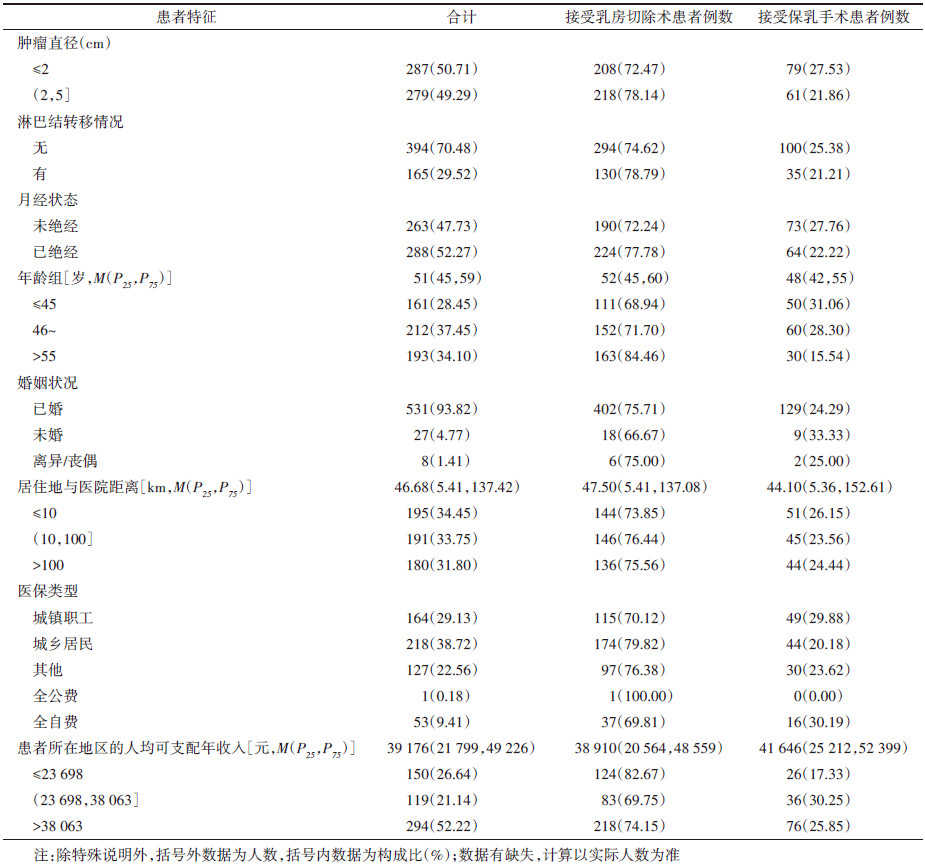
(2)患者的人口、社会和经济学特征:包括患者的出生日期、婚姻状况、医保类型及家庭住址。将患者确诊时的年龄分为3组(≤45、46~及 > 55岁)。根据患者的家庭住址确定其所在区(县),并根据患者所在地区的居民人均可支配年收入将患者划分为低、中、高3组{≤23 698、(23 698,38 063]、> 38 063元},以患者所在地区的居民人均可支配年收入作为患者经济水平的参考指标。计算患者家庭住址与调查医院之间高德地图软件显示的公路距离,并将患者分为3组{≤10、(10,100]、> 100 km},以患者家庭住址与调查医院间的距离作为患者就医便捷程度的参考指标。
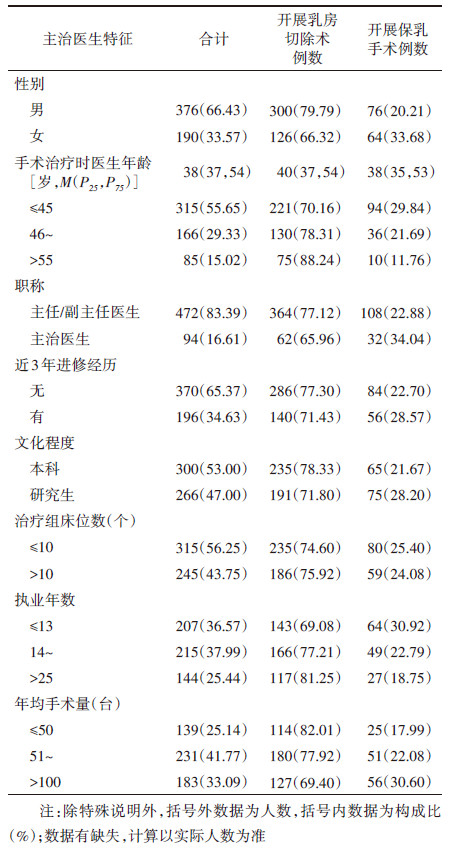
(3)主治医生特征:包含医生性别、年龄、职称、近3年进修经历、文化程度、所在治疗组床位数、执业年数及乳腺癌手术年均手术量。将连续变量进行分类转换,对患者手术治疗当年的医生年龄(≤45、46~、> 55岁)、医生执业年数(≤13、14~、> 25年)及年均手术量(≤50、51~、> 100例)按照数据分布分别分为3组。
4. 统计学分析:目标患者是同一家医院连续5年收治的所有符合研究要求的早期乳腺癌患者,其临床特征及社会人口学特征在5年间的分布差异无统计学意义。该医院持续开展乳腺癌手术的医生无显著变化。在研究时间内乳腺癌诊疗指南未发生变化和研究医院未开展影响保乳手术干预项目的条件下,将5年样本合并分析。首先对收集的数据进行正态性检验,连续变量使用x±s和M(P25,P75)报告,分类变量采用频率计数和百分比(%)报告。连续变量的单因素分析采用Mann-Whitney U检验,分类变量的单因素分析采用χ2检验。影响因素分析采用二分类logistic多元回归模型。将患者的手术方式(保乳手术=1,乳房切除术=0)作为因变量,自变量选择单因素分析手术方式在不同特征患者中的分布差异有统计学意义的变量(检验水准α放宽至0.15)和根据专业判断需纳入的变量。考虑到未观测的因素可能造成的样本异质性,在多因素logistic回归模型中引入时间控制变量。由于保乳手术决策的复杂性及医患关系的特殊性,患者相关变量对其手术方式选择的作用很有可能受到某些医生变量的影响,产生交互效应。探索发现的医患双方的年龄是两个较强的影响因素,将患者年龄与主治医生年龄两个连续变量去中心化处理后,引入医患年龄交互项,进一步分析在对方不同年龄条件下,医患年龄对患者选择保乳手术概率影响的边际影响效应。通过计算平均边际效应(average marginal effects)对交互项的影响效应进一步解释[32-33]。由于非线性模型中交互项的回归系数并不能全面反应交互项的影响效应,为更准确地计算logit模型中交互项的影响效应,采用“inteff”命令计算所有样本的医患年龄交互作用对预测保乳手术概率的影响效应估计值、sx和Z统计量的平均值、最大效应、最小效应和标准差[34-36]。为更好地控制sx估计偏倚,各模型的sx均使用稳健估计。所有统计分析使用Stata 16.1软件,统计学检验显著水平设置为α=0.05。
结果1. 患者特征:纳入研究的早期乳腺癌女性患者共566例,最小年龄23岁,最大年龄91岁,平均年龄52岁。其中观察期内接受保乳手术的目标患者共140例,适宜保乳率(接受保乳手术患者占所有适宜开展保乳手术患者的比例)为24.73%。患者临床特征及社会人口学特征见表 1,分布的差异无统计学意义。
2. 主治医生特征:目标患者对应的主治医生共15名,来自肿瘤外科(9名)、基本外科(5名)以及胸外科(1名);研究开展时医生年龄最小为35岁,最大62岁,平均年龄45岁,男性(12名)医生占大多数。被调查医生均为5年内在研究医院连续开展乳腺癌诊疗的医生,医生特征在观察期内的分布差异无统计学意义。目标患者对应的主治医生特征见表 2。
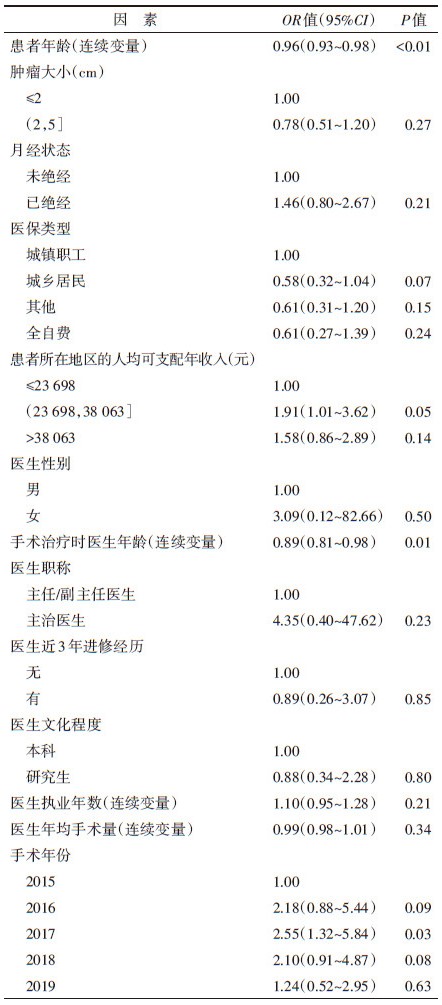
3. 适宜保乳女性乳腺癌术式决策影响因素的多元logistic回归分析:将单因素分析有统计学意义的因素纳入logistic回归分析,结果显示,患者年龄越大,选择保乳手术的可能性越小(OR=0.96,95%CI:0.93~0.98,P < 0.01)。中等收入地区的患者选择保乳手术的概率是低收入地区患者的1.91倍(OR=1.91,95%CI:1.01~3.62,P=0.05)。患者接受手术治疗时主治医生的年龄越大,其选择保乳手术的可能性越低(OR=0.89,95%CI:0.81~0.98,P=0.01)。见表 3。
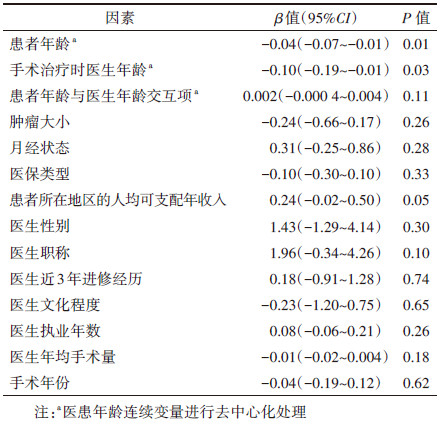
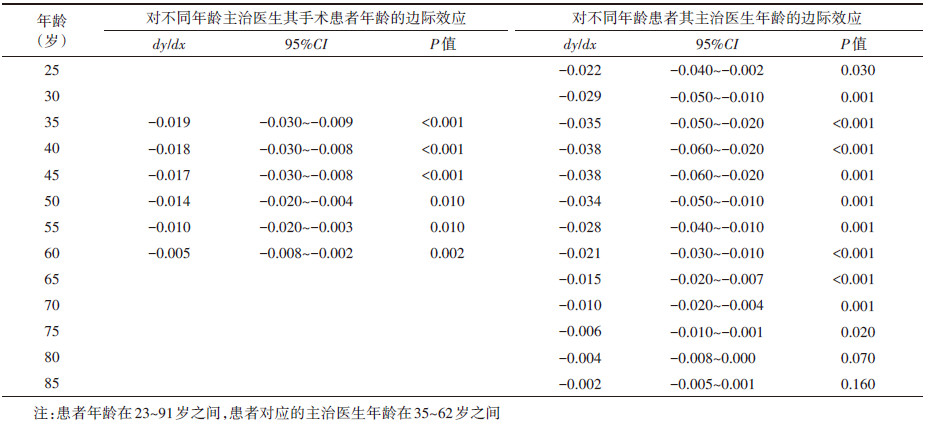
将医、患年龄进行去中心化处理,引入医患年龄的交互项,拟合结果显示,医患双方的年龄变量仍然是患者选择保乳手术的重要影响因素,当保持其他变量取值不变,患者的主治医生处于平均年龄(45岁)时,患者年龄每增加1岁,选择保乳手术预测概率降低4%(95%CI:-0.07~-0.01,P=0.01);患者处于平均年龄(52岁)时,其主治医生年龄每增长1岁,选择保乳手术的预测概率降低10%(95%CI:-0.19~-0.01,P=0.03)。见表 4。
当保持其他变量取值不变,主治医生年龄为35岁时,患者年龄影响其选择保乳手术概率的负边际效应最大,患者年龄每增长1岁,其选择保乳手术的概率下降1.90%(95%CI:-0.030~-0.009,P < 0.001);主治医生年龄达到35岁以后,患者年龄影响其选择保乳手术概率的负边际效应递减。当保持其他变量取值不变,患者年龄 < 40岁时,主治医生年龄影响其主诊的患者选择保乳手术概率的边际效应递增;患者年龄增长到40或45岁时,主治医生年龄影响其主诊的患者选择保乳手术概率的边际效应最大,主治医生年龄每增长1岁,其主诊的患者选择保乳手术的概率下降3.80%(95%CI:-0.060~-0.020,P < 0.001或P=0.001);患者年龄 > 45岁以后,主治医生年龄影响其主诊的患者选择保乳手术概率的边际效应递减;患者年龄达到80岁后,主治医生年龄对其主诊的患者选择保乳手术概率的影响效应已无统计学意义。由此进一步证实,非线性模型中交互项的回归系数并不能全面地解释交互项的影响效应。见表 5。
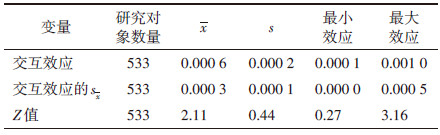
采用“inteff”命令精确估计logit模型中两个连续的年龄变量的交互影响效应,结果显示,所有研究对象的医患年龄交互项对其选择保乳手术概率的影响效应均为正向,平均效应为0.06%(Z=2.11,sx =0.000 3,P < 0.05),最小效应无统计学意义,最大效应为0.1%(Z=3.16,sx =0.000 5,P < 0.05)。见表 6。
按照线性模型交互项的参数估计logit模型交互项的影响效应,低估了医患年龄交互作用对绝大多数研究对象选择保乳手术概率的影响效应。医患年龄交互作用对部分研究对象的影响效应有统计学意义(Z > 1.96,P < 0.05)。见图 1。

|
| 图 1 患者/主治医生年龄交互作用对保乳手术预测概率影响效应的估计和Z统计量 |
我国乳腺癌保乳手术起步晚,医生及患者普遍对保乳手术的认知有限,选择意愿较弱。样本医院2015-2019年平均适宜保乳率为24.73%,与欧美地区60%~80%的水平相差很多[37-38]。我国保乳手术开展率较低的原因包括癌症早期比例低[39]、乳房体积小、乳房组织致密[40]等客观因素,也包括医患的社会心理因素[41]、医疗资源因素和患者经济负担因素[42]。本研究只纳入适宜接受保乳手术的患者,在一定程度上排除了疾病本身特征及客观条件对患者手术方式选择的影响,重点关注医患双方保乳意愿及相互影响对手术决策的影响。
患者年龄是早期乳腺癌患者选择保乳手术的影响因素,选择保留乳房手术患者年龄偏低,与现有研究发现一致[16, 28, 43-44]。本研究通过患者访谈发现,多位年长女性乳腺癌患者认为自己没有必要保留乳房,且切除后能一劳永逸,故而选择了乳房切除术。目前临床上老年乳腺癌患者的手术治疗主要采用改良根治手术,但有研究显示对于合并有高血压、心脏病和糖尿病的高龄早期乳腺癌患者而言,选择保乳手术可减少术后并发症,降低围手术期风险[45-46]。对具有保乳手术指征的老年乳腺癌患者,保乳手术仍可作为推荐术式。
患者支付能力是另一影响因素。原则上,保乳手术后均需行放疗以降低局部复发率。常规放疗周期为5周,共计25次放射治疗,还需更多的影像及病理评估[29],费用较高。居住在中等收入地区的患者比低收入地区的患者更可能接受保乳手术,一定程度上反映了患者的经济水平对手术方式选择的影响[16, 47-48]。与城镇职工医保参保患者相比,城乡居民医保参保患者选择保乳手术的可能性大幅降低,提示医疗保障待遇较好的城镇职工医保参保患者较医保待遇较差的城乡居民医保参保患者更有机会接受保乳手术治疗,与国内外现有研究结果相似,享有高水平医疗保障的患者能选择更好的治疗方案和医疗服务[49-51]。由于保乳治疗费用较高,支付能力较强的患者更有机会接受保乳治疗。进一步提高城乡居民医保待遇水平,特别加强对经济困难家庭的保障,有助于低收入家庭患者群体接受保乳手术治疗。
主治医生年龄是影响乳腺癌患者手术方式决策的重要因素,这与国外现有研究的发现一致[31, 52-53]。医生对早期乳腺癌患者术式选择的倾向和推荐可能随年龄增长偏于保守。年龄较大的医生可能对乳腺癌前沿治疗技术掌握和运用不足。适宜乳腺癌保乳手术的决策涉及多方因素,且这些因素相互作用、相互影响。要推广适宜乳腺癌保乳手术,医患双方须共同努力。应加强对相关科室医生的专业培训与技能进修,使医生充分理解保乳手术的循证证据及优势,提升医生的诊疗水平。临床医生应重视不同年龄段患者的心理需求,对患者进行个性化的术前教育及心理干预,树立患者对保乳手术安全性、有效性、术后并发症等的客观认知水平[18],将最佳治疗方案与患者的需求和愿望协调。
本研究是基于省级医学中心的单中心回顾性调查研究,样本量较小,一些社会人口学指标(如患者的文化程度、职业等)难以收集获得,可能无法全面地观测医患双方特征及其交互作用对患者术式选择的影响。另外,由于主治医生制度未完全落实到位,病案首页中存在一定的信息缺失。对于未写明主治医生的患者,以该患者的手术医生代替调查,可能造成医生因素分析偏倚。因此,在未来的研究中需要扩大研究区域及样本,进行前瞻性研究验证以上发现。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. DOI:10.3322/caac.21660 |
| [2] |
International Agency for Research on Cancer. Estimated number of new cases in 2020, China, females, all ages[EB/OL]. [2021-02-28]. https://iarc.who.int/.
|
| [3] |
张彦收, 刘运江. 乳腺癌手术治疗回顾和进展[J]. 现代肿瘤医学, 2015, 23(5): 719-722. Zhang YS, Liu YJ. A review for the surgical management of breast cancer and the latest developments[J]. J Mod Oncol, 2015, 23(5): 719-722. DOI:10.3969/j.issn.1672-4992.2015.05.42 |
| [4] |
田乃元. 乳腺癌患者乳房再造意向及影响因素的多中心研究[D]. 北京: 北京协和医学院, 2018. Tian NY. A Multi-institutional survey of breast cancer patients' intention of breast reconstruction and the factors influencing their choices[D]. Beijing: Peking Union Medical College, 2018. |
| [5] |
Härtl K, Janni W, Kästner R, et al. Impact of medical and demographic factors on long-term quality of life and body image of breast cancer patients[J]. Ann Oncol, 2003, 14(7): 1064-1071. DOI:10.1093/annonc/mdg289 |
| [6] |
Kwait RM, Pesek S, Onstad M, et al. Influential forces in breast cancer surgical decision making and the impact on body image and sexual function[J]. Ann Surg Oncol, 2016, 23(10): 3403-3411. DOI:10.1245/s10434-016-5365-2 |
| [7] |
Al-Ghazal SK, Fallowfield L, Blamey RW. Comparison of psychological aspects and patient satisfaction following breast conserving surgery, simple mastectomy and breast reconstruction[J]. Eur J Cancer, 2000, 36(15): 1938-1943. DOI:10.1016/s0959-8049(0)00197-0 |
| [8] |
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer[J]. N Engl J Med, 2002, 347(16): 1233-1241. DOI:10.1056/NEJMoa022152 |
| [9] |
Agarwal S, Pappas L, Neumayer L, et al. Effect of breast conservation therapy vs mastectomy on disease-specific survival for early-stage breast cancer[J]. JAMA Surg, 2014, 149(3): 267-274. DOI:10.1001/jamasurg.2013.3049 |
| [10] |
van Maaren MC, de Munck L, de Bock GH, et al. 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: a population-based study[J]. Lancet Oncol, 2016, 17(8): 1158-1170. DOI:10.1016/s1470-2045(16)30067-5 |
| [11] |
张保宁, 邵志敏, 乔新民, 等. 中国乳腺癌保乳治疗的前瞻性多中心研究[J]. 中华肿瘤杂志, 2005, 27(11): 44-48. Zhang BN, Shao ZM, Qiao XM, et al. A prospective multicenter clinical trial of breast conserving therapy for early breast cancer in China[J]. Chin J Oncol, 2005, 27(11): 44-48. DOI:10.3760/j.issn:0253-3766.2005.11.011 |
| [12] |
Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer[J]. N Engl J Med, 2002, 347(16): 1227-1232. DOI:10.1056/NEJMoa020989 |
| [13] |
Consensus conference. Treatment of early stage breast cancer. National Institutes of Health[J]. Conn Med, 1991, 55(2): 101-107. |
| [14] |
Jonczyk MM, Jean J, Graham R, et al. Surgical trends in breast cancer: a rise in novel operative treatment options over a 12 year analysis[J]. Breast Cancer Res Treat, 2019, 173(2): 267-274. DOI:10.1007/s10549-018-5018-1 |
| [15] |
赵乙壑. 中国早期乳腺癌保乳手术开展现状多中心调查研究[D]. 济南: 山东大学, 2020. DOI: 10.27272/d.cnki.gshdu.2020.004696. Zhao YH. A multicenter study on the status of breast-conserving surgery in early-stage breast cancer in China[D]. Ji'nan: Shandong University, 2020. DOI: 10.27272/d.cnki.gshdu.2020.004696. |
| [16] |
傅建琴. 乳腺癌患者选择手术方式的影响因素调查分析[J]. 基层医学论坛, 2016, 20(34): 4892-4894. Fu JQ. Investigation and analysis of factors influencing breast cancer patients' choice of surgical procedures[J]. Med Forum, 2016, 20(34): 4892-4894. DOI:10.3969/j.issn.1672-1721.2016.34.089 |
| [17] |
张景涵. 乳腺癌女性患者乳腺癌根治术和保乳手术选择意愿调查及影响因素分析[J]. 中国妇幼保健, 2020, 35(20): 3868-3871. Zhang JH. Investigation of breast cancer radical mastectomy and breast conserving surgery in women with breast cancer and influencing factors[J]. Mate Child Health Care China, 2020, 35(20): 3868-3871. DOI:10.19829/j.zgfybj.issn.1001-4411.2020.20.050 |
| [18] |
张静. 适合保乳手术的乳腺癌患者手术方式选择的影响因素[D]. 石家庄: 河北医科大学, 2019. Zhang J. The factors influencing choice of surgical treatments of the patients suitable for breast-conserving surgery[D]. Shijiazhuang: Hebei Medical University, 2019. |
| [19] |
张培, 李霞, 李国媛. 早期乳腺癌患者影响保乳手术选择的因素分析[J]. 天津护理, 2013, 21(6): 479-481. Zhang P, Li X, Li GY. The factors influencing choice of conserving surgery of the patients with early stage breast cancer[J]. Tianjin J Nurs, 2013, 21(6): 479-481. DOI:10.3969/j.issn.1006-9143.2013.06.004 |
| [20] |
Fagerlin A, Lakhani I, Lantz PM, et al. An informed decision? Breast cancer patients and their knowledge about treatment[J]. Patient Educ Couns, 2006, 64(1/3): 303-312. DOI:10.1016/j.pec.2006.03.010 |
| [21] |
Gu J, Delisle M, Engler-Stringer R, et al. Mastectomy versus breast-conservation therapy: an examination of how individual, clinicopathologic, and physician factors influence decision-making[J]. Curr Oncol, 2019, 26(4): e522-534. DOI:10.3747/co.26.5079 |
| [22] |
Schou I, Ekeberg Ø, Ruland CM, et al. Do women newly diagnosed with breast cancer and consulting surgeon assess decision-making equally?[J]. Breast, 2002, 11(5): 434-441. DOI:10.1054/brst.2002.0454 |
| [23] |
林燕苹, 陈述政, 殷文瑾, 等. 乳腺癌患者保乳治疗选择的社会心理因素分析[J]. 复旦学报: 医学版, 2008, 35(5): 641-645. Lin YP, Chen SZ, Yin WJ, et al. Factors that influencing patients' decision making for breast conserving surgery[J]. Fudan Univ J Med Sci, 2008, 35(5): 641-645. DOI:10.3969/j.issn.1672-8467.2008.05.002 |
| [24] |
Polsky D, Mandelblatt JS, Weeks JC, et al. Economic evaluation of breast cancer treatment: considering the value of patient choice[J]. J Clin Oncol, 2003, 21(6): 1139-1146. DOI:10.1200/jco.2003.03.126 |
| [25] |
Barlow WE, Taplin SH, Yoshida CK, et al. Cost comparison of mastectomy versus breast-conserving therapy for early-stage breast cancer[J]. J Natl Cancer Inst, 2001, 93(6): 447-455. DOI:10.1093/jnci/93.6.447 |
| [26] |
Reitsamer R, Menzel C, Glueck S, et al. Predictors of mastectomy in a certified breast center-the surgeon is an independent risk factor[J]. Breast J, 2008, 14(4): 324-329. DOI:10.1111/j.1524-4741.2008.00592.x |
| [27] |
Opatt D, Morrow M, Hawley S, et al. Conflicts in decision-making for breast cancer surgery[J]. Ann Surg Oncol, 2007, 14(9): 2463-2469. DOI:10.1245/s10434-007-9431-7 |
| [28] |
Molenaar S, Oort F, Sprangers M, et al. Predictors of patients' choices for breast-conserving therapy or mastectomy: a prospective study[J]. Br J Cancer, 2004, 90(11): 2123-2130. DOI:10.1038/sj.bjc.6601835 |
| [29] |
中国抗癌协会乳腺癌专业委员会. 中国抗癌协会乳腺癌诊治指南与规范(2019年版)[J]. 中国癌症杂志, 2019, 29(8): 609-679. China Cancer Association Breast Cancer Specialized Committee. Guidelines and guidelines for breast cancer diagnosis and treatment of China Cancer Association (2019 Edition)[J]. China Oncol, 2019, 29(8): 609-679. DOI:10.19401/j.cnki.1007-3639.2019.08.009 |
| [30] |
American Joint Committee on Cancer. AJCC Cancer Staging Manual, 8th Edition[EB/OL]. (2016). [2021-02-28]. https://cancerstaging.org/references-tools/deskreferences/Pages/default.aspx.
|
| [31] |
Hershman DL, Buono D, Jacobson JS, et al. Surgeon characteristics and use of breast conservation surgery in women with early stage breast cancer[J]. Ann Surg, 2009, 249(5): 828-833. DOI:10.1097/SLA.0b013e3181a38f6f |
| [32] |
Williams RA. Using the margins command to estimate and interpret adjusted predictions and marginal effects[J]. Stata J, 2012, 12(2): 308-331. DOI:10.1177/1536867X1201200209 |
| [33] |
Karaca-Mandic P, Norton EC, Dowd B. Interaction terms in nonlinear models[J]. Health Serv Res, 2012, 47(1 Pt 1): 255-274. DOI:10.1111/j.1475-6773.2011.01314.x |
| [34] |
Norton EC, Wang H, Ai CR. Computing interaction effects and standard errors in logit and probit models[J]. Stata J, 2004, 4(2): 154-167. DOI:10.1177/1536867x0400400206 |
| [35] |
Ai CR, Norton EC. Interaction terms in Logit and probit models[J]. Econom Lett, 2003, 80(1): 123-129. DOI:10.1016/S0165-1765(3)00032-6 |
| [36] |
詹姆斯·杰卡德. Logistic回归中的交互效应[M]. 缪佳, 译. 上海: 格致出版社, 2014. Jaccard J. Interaction effect in logistic regression[M]. Miao J, trans. Shanghai: Truth & Wisdom Press, 2014. |
| [37] |
Garcia-Etienne CA, Tomatis M, Heil J, et al. Mastectomy trends for early-stage breast cancer: a report from the EUSOMA multi-institutional European database[J]. Eur J Cancer, 2012, 48(13): 1947-1956. DOI:10.1016/j.ejca.2012.03.008 |
| [38] |
Kummerow KL, Du LP, Penson DF, et al. Nationwide trends in mastectomy for early-stage breast cancer[J]. JAMA Surg, 2015, 150(1): 9-16. DOI:10.1001/jamasurg.2014.2895 |
| [39] |
闫宇, 周灿. 中美两国女性乳腺癌临床病理特征及治疗的对比研究[J]. 现代肿瘤医学, 2019, 27(8): 1344-1351. Yan Y, Zhou C. A comparative study of clinic-pathological features and treatment of female breast cancer in China and USA[J]. J Mod Oncol, 2019, 27(8): 1344-1351. DOI:10.3969/j.issn.1672-4992.2019.08.014 |
| [40] |
邵志敏. 乳腺癌保乳手术的进展与评述[J]. 肿瘤防治研究, 2018, 45(5): 269-273. Shao ZM. Progress and comment of breast conserving therapy[J]. Cancer Res Prev Treat, 2018, 45(5): 269-273. DOI:10.3971/j.issn.1000-8578.2018.18.0268 |
| [41] |
Killoran M, Moyer A. Surgical treatment preferences in Chinese-American women with early-stage breast cancer[J]. Psycho-Oncol, 2006, 15(11): 969-984. DOI:10.1002/pon.1032 |
| [42] |
Greenup RA, Rushing C, Fish L, et al. Financial costs and burden related to decisions for breast cancer surgery[J]. J Oncol Pract, 2019, 15(8): e666-676. DOI:10.1200/jop.18.00796 |
| [43] |
Chagpar AB, Studts JL, Scoggins CR, et al. Factors associated with surgical options for breast carcinoma[J]. Cancer, 2006, 106(7): 1462-1466. DOI:10.1002/cncr.21728 |
| [44] |
Locker GY, Sainsbury JR, Cuzick J. Breast surgery in the 'Arimidex, Tamoxifen Alone or in Combination' (ATAC) trial: American women are more likely than women from the United Kingdom to undergo mastectomy[J]. Cancer, 2004, 101(4): 735-740. DOI:10.1002/cncr.20435 |
| [45] |
张珊, 曾繁余, 唐巍, 等. 保乳联合前哨淋巴结活检对老年乳腺癌患者的疗效及对术后生活质量及美容效果的影响[J]. 实用癌症杂志, 2016, 31(1): 124-127. Zhang S, Zeng FY, Tang W, et al. Breast-conserving united with sentinel lymph node biopsy for elderly patients with breast cancer and the impact on quality of life after surgery and cosmetic results[J]. Pract J Cancer, 2016, 31(1): 124-127. DOI:10.3969/j.issn.1001-5930.2016.01.037 |
| [46] |
朱林超, 谷元廷, 赵松. 保乳联合前哨淋巴结活检在老年乳腺癌治疗中的临床价值[J]. 中国老年学杂志, 2012, 32(12): 2504-2506. Zhu LC, Gu YT, Zhao S. Clinical value of breast conserving combined with sentinel lymph node biopsy in elderly patients with breast cancer[J]. Chin J Gerontol, 2012, 32(12): 2504-2506. DOI:10.3969/j.issn.1005-9202.2012.12.028 |
| [47] |
Benedict S, Cole DJ, Baron L, et al. Factors influencing choice between mastectomy and lumpectomy for women in the Carolinas[J]. J Surg Oncol, 2001, 76(1): 6-12. DOI:10.1002/1096-9098(200101)76:1<6:aid-jso1002>3.0.co;2-f |
| [48] |
Sauerzapf VA, Jones AP, Haynes R, et al. Travel time to radiotherapy and uptake of breast-conserving surgery for early stage cancer in Northern England[J]. Health Place, 2008, 14(3): 424-433. DOI:10.1016/j.healthplace.2007.09.002 |
| [49] |
Wang ZH, Li XJ, Chen MS, et al. Social health insurance, healthcare utilization, and costs in middle-aged and elderly community-dwelling adults in China[J]. Int J Equity Health, 2018, 17(1): 17. DOI:10.1186/s12939-018-0733-0 |
| [50] |
Han JQ, Meng YY. Institutional differences and geographical disparity: the impact of medical insurance on the equity of health services utilization by the floating elderly population-evidence from China[J]. Int J Equity Health, 2019, 18(1): 91. DOI:10.1186/s12939-019-0998-y |
| [51] |
Li Z, Hung P, He RB, et al. Disparities in end-of-life care, expenditures, and place of death by health insurance among cancer patients in China: a population-based, retrospective study[J]. BMC Public Health, 2020, 20(1): 1354. DOI:10.1186/s12889-020-09463-1 |
| [52] |
Roder D, Zorbas H, Kollias J, et al. Factors predictive of treatment by Australian breast surgeons of invasive female breast cancer by mastectomy rather than breast conserving surgery[J]. Asian Pac J Cancer Prev, 2013, 14(1): 539-545. DOI:10.7314/apjcp.2013.14.1.539 |
| [53] |
Cyran EM, Crane LA, Palmer L. Physician sex and other factors associated with type of breast cancer surgery in older women[J]. Arch Surg, 2001, 136(2): 185-191. DOI:10.1001/archsurg.136.2.185 |