 2021, Vol. 42
2021, Vol. 42文章信息
- 杨晓帆, 刘珍珍, 贾存显.
- Yang Xiaofan, Liu Zhenzhen, Jia Cunxian
- 家庭矛盾与青少年自杀行为关系的队列研究
- A longitudinal study of relationship between family conflict and suicidal behavior in adolescents
- 中华流行病学杂志, 2021, 42(11): 1976-1982
- Chinese Journal of Epidemiology, 2021, 42(11): 1976-1982
- http://dx.doi.org/10.3760/cma.j.cn112338-20210317-00215
-
文章历史
收稿日期: 2021-03-17




自杀是世界上重要的公共卫生和社会问题之一,每年超过80万人死于自杀,同时是青少年的第二大死亡原因,仅次于交通意外造成的生命损失[1]。近年来中国自杀率有所下降[2],但疾病负担仍较重[3],仍然是青壮年死亡的重要原因,且自杀行为在青少年阶段增加[4]。自杀行为包括自杀意念、自杀计划、自杀未遂、自杀死亡等[5],而自杀意念、自杀计划和自杀未遂是青少年自杀死亡的重要预测因素。早期筛查和识别青少年自杀行为的相关因素对预防青少年自杀死亡的发生具有重要意义。青少年正处于身心快速发展的新阶段,面对变化的周围环境,压力越来越大,更容易出现心理问题。家庭是青少年生存发展的重要环境之一,是青少年身心发展的关键因素,良好的家庭关系是青少年不良行为的保护因素[6]。家庭矛盾是指家庭成员相互间的矛盾和冲突,包括父母和亲子冲突等,其可能导致青少年自杀行为的发生[7-9]。研究表明父母冲突[10]和亲子冲突[4]对青少年自杀行为有一定的影响。本研究通过山东省青少年队列探讨青少年家庭矛盾和自杀行为的关系,为从家庭角度预防和控制青少年自杀提供科学依据。
对象与方法1.研究对象:来自山东省青少年行为与健康队列。综合考虑样本的代表性、前期合作、经费等问题,选取山东省邹城市、阳谷县和利津县为调查地点,5所初中和3所高中为调查学校,采用方便整群抽样的方式于2015年11-12月对8所中学7~11年级在校且自愿参加调查的中学生进行问卷调查,2016年对7、8和10年级中学生进行随访。本研究选取同时参与基线和随访的学生作为研究样本。本研究通过山东大学公共卫生学院伦理委员会审查(批准文号:20161102)。
2.调查方法和内容:问卷自填。获得学生和老师同意后,由调查员指导填写。具体的设计、实施和调查方案见相关文献[11-12]。青少年健康和行为问卷[13]由课题组自行设计,调查内容:①基线人口学信息:性别、年龄、吸烟、饮酒、身体健康状况、家庭经济状况、父母婚姻状况和父母职业等。②自杀行为:通过条目“过去12个月,你是否曾认真地考虑过自杀”“过去12个月,你是否曾计划过自杀” “过去12个月,你是否采取过自杀行为(不是口头说说)”评价青少年过去一年的自杀意念、自杀计划和自杀未遂。研究对象对上述问题回答“是/否”,若某条目回答“是”,则认为其具有相应的自杀行为;如果研究对象报告有自杀意念、自杀计划或自杀未遂,则认为其具有自杀行为。基线和随访的自杀行为测量方式相同。③家庭矛盾:测量基线家庭矛盾得分。采取家庭环境量表中文版(Family Environment Scale-Chinese Version,FES-CV)矛盾分量表测量家庭成员间的矛盾特征[14]。该分量表共9个条目,每个条目答案为“是/否”,“是”计为1分,“否”计为2分,根据公式求和,总分范围0~9,得分越高家庭矛盾越大。FES-CV具有良好的信效度[14],该分量表在本研究人群的克朗巴赫系数为0.68。④抑郁:使用流调中心抑郁水平评定量表(Center for Epidemiologic Studies Depression Scale,CES-D)[15]调查研究对象最近一周的抑郁状况。该量表共20个条目,每个条目0~3分,总分0~60分,分值越高抑郁程度越严重。该量表在本研究人群中的克朗巴赫系数为0.86。⑤失眠:通过Liu等[16]编制的青少年失眠自评量表(Youth Self⁃Rating Insomnia Scale,YSIS)评价研究对象最近一个月的失眠情况。共8个条目,每个条目为1~5分,总分8~40分,得分越高失眠程度越严重。该量表在本研究人群的克朗巴赫系数为0.79。⑥特质愤怒:通过特质愤怒量表测量个体感知愤怒激发情境及愤怒表现反应的一般倾向[17]。共10个条目,每个条目为1~4分,总分10~40分,得分越高表明越容易愤怒。该量表在本研究人群中的克朗巴赫系数为0.88。
3.统计学分析:采用Stata15.0软件进行统计学分析。采用χ2检验或两独立样本t检验或Wilcoxon秩和检验对随访研究对象的基线人口学特征进行比较。采用logistic回归模型对全样本进行分析,探讨基线家庭矛盾得分和随访时过去一年自杀行为间的关系。采用敏感性分析的方法对基线时无自杀行为者进行研究,验证该队列中家庭矛盾得分和随访时过去一年自杀行为的关系。所有检验均为双侧检验,检验水准α=0.05。
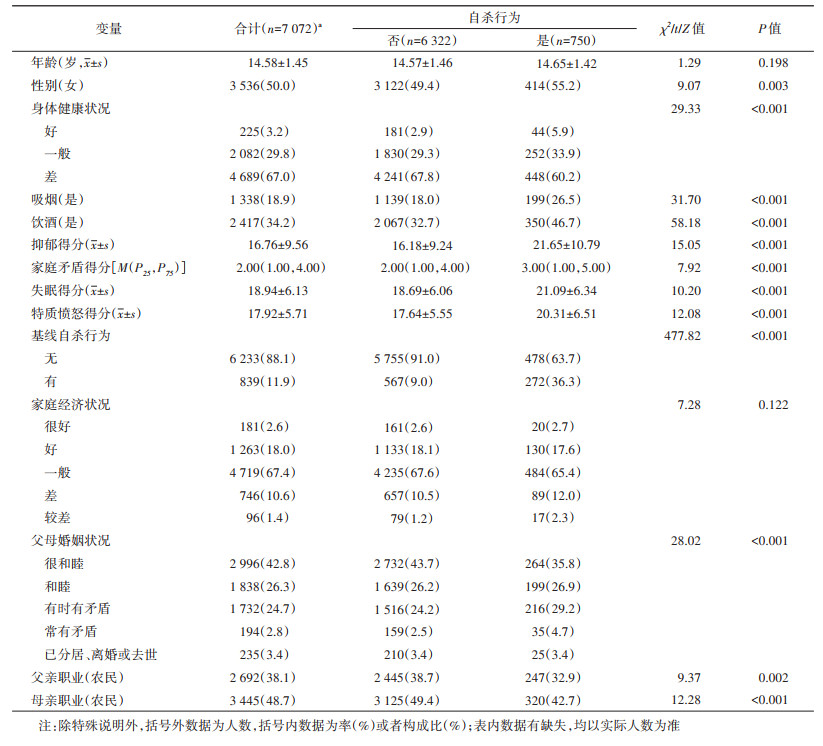
结果1.基本特征:共纳入分析7072人,其中750人在随访时有自杀行为。与没有自杀行为的人相比,有自杀行为者中女生居多、吸烟率、饮酒率以及父母婚姻状况不和谐报告率更高(Ps < 0.001)。存在自杀行为者的失眠、特质愤怒和抑郁水平均高于非自杀者,去年自杀行为报告率更高(Ps < 0.001)。见表 1。
2.自杀行为报告率:该研究基线调查时纳入7、8、10年级学生共8629人,一年后随访到7072名(82.0%)研究对象,有任何自杀行为的有750人(10.6%),其中自杀意念、自杀计划和自杀未遂的人数(报告率)分别为707人(10.0%)、258人(3.6%)和190人(2.7%)。男生和女生的自杀行为报告率差异有统计学意义(9.5%vs.11.7%,χ2=9.07,P=0.003)。女生自杀意念的报告率(11.2%)高于男生(8.8%),差异有统计学意义(P=0.001)。见图 1。剔除基线存在自杀行为的人后,共纳入基线未发生自杀行为者6233人,在该人群中随访一年时自杀行为人数(报告率)为478人(7.7%),其中自杀意念、自杀计划和自杀未遂的人数(报告率)分别为446人(7.2%)、155人(2.5%)、113人(1.8%)。基线未有任何自杀行为群体中,一年随访期间男生和女生的自杀行为报告率差异无统计学意义(Ps>0.05)。见图 2。

|
| 图 1 全样本中不同性别的自杀行为报告率(n=7 072) |

|
| 图 2 基线无自杀行为者中不同性别的自杀行为报告率(n=6 233) |
3.家庭矛盾得分情况:随访时没有自杀行为者其基线家庭矛盾得分M为2分,有自杀行为者家庭矛盾得分M为3分,得分差异有统计学意义(P < 0.001)。在男生(Z=5.30)和女生(Z=5.79)中两组间基线家庭矛盾得分差异均有统计学意义(Ps < 0.001)。
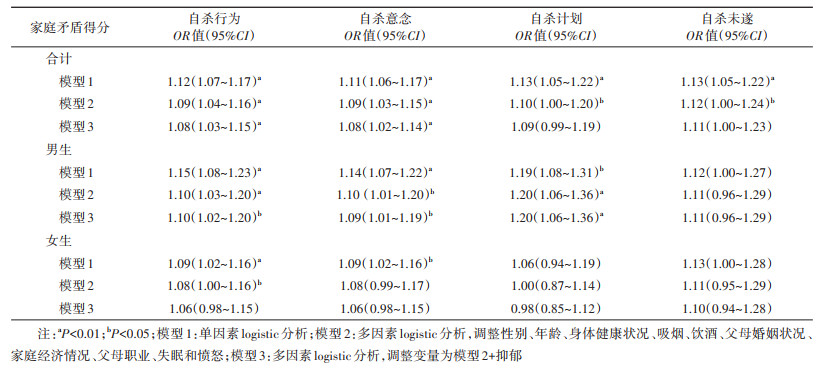
4.家庭矛盾得分和自杀行为的关系:单因素分析显示,家庭矛盾得分与自杀行为(OR=1.16,95%CI:1.12~1.20)、自杀意念(OR=1.15,95%CI:1.11~1.19)、自杀计划(OR=1.17,95%CI:1.11~1.24)和自杀未遂(OR=1.18,95%CI:1.11~1.26)均有统计学关联。经过调整以后,家庭矛盾得分与自杀行为、自杀意念、自杀计划和自杀未遂的关联性仍然有统计学意义,其OR值(95%CI)分别是1.05(1.01~ 1.10)、1.05(1.00~1.09)、1.08(1.01~1.16)和1.10(1.02~1.19)。考虑到性别的影响,随后进行分层logistic回归分析。结果显示,经过调整以后,男生家庭矛盾和自杀行为、自杀意念、自杀计划存在关联;而女生在未进行调整之前,家庭矛盾与自杀行为、自杀意念和自杀未遂有统计学关联,而调整后的家庭矛盾与自杀行为无统计学关联。见表 2。

5.敏感性分析:对家庭矛盾得分和自杀行为的关系进行敏感性分析。对基线没有任何自杀行为者进行logistic回归分析。调整后的结果显示,在过去一年没有自杀行为的人中,男生家庭矛盾可以预测未来一年的自杀行为(OR=1.10,95%CI:1.02~ 1.20)、自杀意念(OR=1.09,95%CI:1.01~1.19)和自杀计划(OR=1.20,95%CI:1.06~1.36);在女生中则不具有预测作用。总体来说,家庭矛盾可以预测自杀行为(OR=1.08,95%CI:1.03~1.15)、自杀意念(OR=1.08,95%CI:1.02~1.14)。家庭矛盾对于男生自杀行为的预测作用较为稳定。见表 3。
青少年自杀行为的发生是生物、心理和环境因素综合作用的结果[18]。本研究结果显示性别、吸烟、饮酒、身体健康状况、抑郁水平、特质愤怒、父母婚姻状况等都与青少年自杀行为的发生有关,且去年存在自杀行为的青少年在随访一年时的自杀行为报告率明显增高。这与之前的研究结果一致[19-20],且已有综述认为先前的自杀行为对于后期自杀的影响具有较高的证据水平[21]。提示在青少年自杀预防工作中,应关注高危人群,尤其是应重点关注先前有过自杀行为的青少年,提高心理健康教育水平和增加多方面的人际支持,避免重复自杀行为的发生。
本研究青少年过去一年自杀行为的报告率均低于全球青少年过去一年自杀行为的报告率[22],但是与加拿大相比,中国青少年过去一年自杀行为报告率更高[23]。除自杀计划外,女性自杀行为的报告率普遍高于男性,这与韩国高中生调查的结果是一致的,但相比而言,中国女生的自杀意念和自杀未遂报告率均较低[24]。而在中国范围内,贵州省的自杀意念和自杀未遂报告率更高[25]。值得注意的是,基于队列研究的特点,本研究报告了过去一年没有任何自杀行为的青少年群体在随访一年时的自杀行为的报告率,该率依然居高不下,男生和女生自杀未遂的报告率分别为1.9%和1.7%,尽管自杀预防已经取得一定进展,近年来自杀率也有所下降[2],但是中国人口基数庞大,青少年自杀给社会带来的负担较大,对于青少年自杀仍然需要给予一定的重视。
家庭是青少年的原生环境,对青少年的生长发育有重要的作用,研究表明家庭冲突和体罚等多种家庭环境因素都与中国青少年的自杀行为有关[26-27]。家庭冲突是指家庭成员间的矛盾,本研究通过队列设计证实了家庭矛盾和青少年自杀行为的关系。这与柬埔寨的调查结果一致,但结果只针对于女性[28],并未对男性做出调查。相比之下,本研究结果显示,相比于女生,男生的家庭矛盾会显著增加其自杀意念和自杀计划发生的危险性。另外,系统综述表明家庭矛盾也是中低收入国家年轻人自杀的危险因素[29],而治疗学研究表明家庭矛盾水平高的人在治疗过程中的自杀行为变化最大[30],间接证实了本研究结论的可靠性。青春期是一个认知不成熟、情绪冲动和自尊发展不足的时期[31]。家庭矛盾作为青少年可能的压力来源,可能通过直接的压力效应和缺乏家庭支持而对青少年自杀产生影响,自杀也成为青少年逃避家庭冲突、缓解精神压力的一种方式[26]。家庭矛盾是青少年情绪和行为问题的危险因素[32],情绪问题可能对青少年的个人动机和认知产生影响,行为问题可能通过冲动等加剧自杀行为发生的可能性[33],对自杀行为的发生具有一定的预测作用[13, 34-35],研究证明抑郁情绪可能是中介因素之一[36]。不同情绪和行为问题的个体对于冲突有不同的应对方式[37],而青少年个体本身应对压力的能力较弱,根据已有研究提出的心理扭力理论[38-39],当个人遭遇某种危机处境,长期处于某种压力中而没有足够能力应对时,会体验到应对扭力,极端的扭力后果便是自杀。社会支持对于心理扭力和自杀有一定的支持作用[40],因此青少年群体在面对包括家庭矛盾在内的各种压力问题时,应当学会主动调节自我情绪问题,积极寻求来自家庭内外的支持。
本研究存在局限性。首先,本研究所有资料的获得都是通过自填问卷的方式进行,可能存在一定程度的报告偏倚,且所利用的数据未能更新,存在一定程度的滞后性;其次,本研究未能全面考察所有可能的家庭环境因素和青少年个体在儿童期的经历,调查时未能全面纳入所有可能影响自杀行为的因素,未能比较不同的家庭矛盾以及童年期的经历等因素对于自杀行为的影响;同时本研究未能继续探究家庭矛盾和自杀行为的中间因素,不能明确家庭因素影响自杀行为的途径;另外,本研究样本在山东省范围内获得,且研究中未能涉及所有年级的中学生,没有调查其学业压力并对其进行控制,所得结论是否能够推广到其他人群和地区,尚有待验证。
青少年正处于一个快速发展变化的阶段,独立的辨别能力和正确的应对能力尚未成熟,面对危机处境和环境压力,较易出现情绪和行为问题,乃至采用自杀的方式来逃避或应对。本研究结果提示家庭环境对于青少年自杀行为具有重要作用,家庭矛盾作为压力源可能成为青少年自杀行为发生的远端因素,因此为预防青少年自杀行为的发生,应保持良好和谐的家庭氛围。同时对于青少年,应当给予足够的家庭支持和社会支持,积极开展心理干预,预防青少年不良行为的发生。
利益冲突 所有作者均声明不存在利益冲突
致谢 感谢山东省邹城市、利津县和阳谷县的CDC工作人员以及参与组织调查的学校领导、老师及参与调查的学生
| [1] |
World Health Organization. Preventing suicide: a global imperative[R]. Geneva: WHO, 2014.
|
| [2] |
邹广顺, 吕军城, 董璐. 中国城乡2002-2018年自杀死亡率发展趋势的Joinpoint回归分析[J]. 中国心理卫生杂志, 2020, 34(10): 828-833. Zou GS, Lyv JC, Dong L. Joinpoint regression analysis of suicide mortality rate trends among urban and rural in China from 2002 to 2018[J]. Chin Ment Health J, 2020, 34(10): 828-833. DOI:10.3969/j.issn.1000-6729.2020.10.005 |
| [3] |
高欣, 王临虹, 金叶, 等. 1990年与2013年中国人群自杀疾病负担分析[J]. 中华流行病学杂志, 2017, 38(10): 1325-1329. Gao X, Wang LH, Jin Y, et al. Disease burden caused by suicide in the Chinese population, in 1990 and 2013[J]. Chin J Epidemiol, 2017, 38(10): 1325-1329. DOI:10.3760/cma.j.issn.0254-6450.2017.10.006 |
| [4] |
赵建彬, 陶建蓉. 亲子冲突对青少年自杀意愿的影响[J]. 中国卫生事业管理, 2019, 36(10): 784-786,795. Zhao JB, Tao JR. The influence of parent-child conflict on adolescents' suicide willingness[J]. Chin Health Serv Manage, 2019, 36(10): 784-786,795. |
| [5] |
肖水源, 周亮, 徐慧兰. 危机干预与自杀预防(二): 自杀行为的概念与分类[J]. 临床精神医学杂志, 2005, 15(5): 298-299. Xiao SY, Zhou L, Xu HL. Crisis intervention and suicide prevention (2) concept and classification of suicidal behaviors[J]. J Clin Psychol, 2005, 15(5): 298-299. DOI:10.3969/j.issn.1005-3220.2005.05.036 |
| [6] |
莫娟婵. 大学生自伤行为和冲动性的关系——负性情绪和家庭环境矛盾的作用[D]. 天津: 天津师范大学, 2018. Mo JC. The relationship between self-injury and impulsivity in Chinese undergraduates: the effect of negative affect and family environment[D]. Tianjin: Tianjin Normal University, 2018. |
| [7] |
de Ville DC, Whalen D, Breslin FJ, et al. Prevalence and family-related factors associated with suicidal ideation, suicide attempts, and self-injury in children aged 9 to 10 years[J]. JAMA Netw Open, 2020, 3(2): e1920956. DOI:10.1001/jamanetworkopen.2019.20956 |
| [8] |
van Meter AR, Paksarian D, Merikangas KR. Social functioning and suicide risk in a community sample of adolescents[J]. J Clin Child Adolesc Psychol, 2019, 48(2): 273-287. DOI:10.1080/15374416.2018.1528549 |
| [9] |
Lee GY, Ham OK. Behavioral and psychosocial factors associated with suicidal ideation among adolescents[J]. Nurs Health Sci, 2018, 20(3): 394-401. DOI:10.1111/nhs.12422 |
| [10] |
赵建彬, 陶建蓉, 李丹雯. 父母冲突对青少年自杀意愿的影响[J]. 赣南师范大学学报, 2020, 41(4): 106-111. Zhao JB, Tao JR, Li DW. An influence of parental conflict on the suicidal willingness of middle school students[J]. J Gannan Norm Univ, 2020, 41(4): 106-111. DOI:10.13698/j.cnki.cn36-1346/c.2020.04.019 |
| [11] |
Liu XC, Chen H, Liu ZZ, et al. Prevalence of suicidal behaviour and associated factors in a large sample of Chinese adolescents[J]. Epidemiol Psychiatr Sci, 2019, 28(3): 280-289. DOI:10.1017/S2045796017000488 |
| [12] |
Liu XC, Chen H, Bo QG, et al. Poor sleep quality and nightmares are associated with non-suicidal self-injury in adolescents[J]. Eur Child Adolesc Psychiatry, 2017, 26(3): 271-279. DOI:10.1007/s00787-016-0885-7 |
| [13] |
Liu XC, Zhao ZT, Jia CX. Insomnia symptoms, behavioral/emotional problems, and suicidality among adolescents of insomniac and non-insomniac parents[J]. Psychiatry Res, 2015, 228(3): 797-802. DOI:10.1016/j.psychres.2015.05.023 |
| [14] |
汪向东, 王希林, 马弘. 心理卫生评定量表手册[M]. 北京: 中国心理卫生杂志社, 1999: 134-142. Wang XD, Wang XL, Ma H. Rating scales for mental health[M]. Beijing: Chinese Mental Health Journal Publisher, 1999: 134-142. |
| [15] |
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population[J]. Appl Psychol Meas, 1977, 1(3): 385-401. DOI:10.1177/014662167700100306 |
| [16] |
Liu XC, Yang YY, Liu ZZ, et al. Psychometric properties of Youth Self-Rating Insomnia Scale (YSIS) in Chinese adolescents[J]. Sleep Biol Rhythms, 2019, 17(3): 339-348. DOI:10.1007/s41105-019-00222-3 |
| [17] |
Spielberger CD, Jacobs GH, Russell SF, et al. Assessment of anger: the state-trait anger-scale[M]//Butcher NJ, Spielberger CD. Advances in personality assessment. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc, 1983: 159-187.
|
| [18] |
Cha CB, Franz PJ, Guzmán EM, et al. Annual Research Review: suicide among youth-epidemiology, (potential) etiology, and treatment[J]. J Child Psychol Psychiatry, 2018, 59(4): 460-482. DOI:10.1111/jcpp.12831 |
| [19] |
Siu AMH. Self-harm and suicide among children and adolescents in Hong Kong: a review of prevalence, risk factors, and prevention strategies[J]. J Adolesc Health, 2019, 64(Suppl 6): S59-64. DOI:10.1016/j.jadohealth.2018.10.004 |
| [20] |
Adewuya AO, Oladipo EO. Prevalence and associated factors for suicidal behaviours (ideation, planning, and attempt) among high school adolescents in Lagos, Nigeria[J]. Eur Child Adolesc Psychiatry, 2020, 29(11): 1503-1512. DOI:10.1007/s00787-019-01462-x |
| [21] |
Fazel S, Runeson B. Suicide[J]. N Engl J Med, 2020, 382(3): 266-274. DOI:10.1056/NEJMra1902944 |
| [22] |
Lim KS, Wong CH, McIntyre RS, et al. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018:a Meta-analysis[J]. Int J Environ Res Public Health, 2019, 16(22): 4581. DOI:10.3390/ijerph16224581 |
| [23] |
Palay J, Taillieu TL, Afifi TO, et al. Prevalence of mental disorders and suicidality in canadian provinces[J]. Can J Psychiatry, 2019, 64(11): 761-769. DOI:10.1177/0706743719878987 |
| [24] |
Lee SA, Jang SY, Shin JY, et al. The association between inappropriate weight control behaviors and suicide ideation and attempt among Korean adolescents[J]. J Korean Med Sci, 2016, 31(10): 1529-1537. DOI:10.3346/jkms.2016.31.10.1529 |
| [25] |
杨婷婷, 卢次勇, 陈钢, 等. 贵州少数民族地区中学生自杀意念及尝试自杀影响因素分析[J]. 中国学校卫生, 2019, 40(7): 1017-1020. Yang TT, Lu CY, Chen G, et al. Factors influencing suicidal ideation and suicide attempt of middle school students in minority areas of Guizhou province[J]. Chin J Sch Health, 2019, 40(7): 1017-1020. DOI:10.16835/j.cnki.1000-9817.2019.07.016 |
| [26] |
Liu XC, Sun ZX, Yang YY. Parent-reported suicidal behavior and correlates among adolescents in China[J]. J Affect Disord, 2008, 105(1/3): 73-80. DOI:10.1016/j.jad.2007.04.012 |
| [27] |
van Orden KA, Witte TK, Cukrowicz KC, et al. The interpersonal theory of suicide[J]. Psychol Rev, 2010, 117(2): 575-600. DOI:10.1037/a0018697 |
| [28] |
Seponski DM, Somo CM, Kao S, et al. Family, health, and poverty factors impacting suicide attempts in Cambodian women[J]. Crisis, 2019, 40(2): 141-145. DOI:10.1027/0227-5910/a000548 |
| [29] |
Aggarwal S, Patton G, Reavley N, et al. Youth self-harm in low- and middle-income countries: systematic review of the risk and protective factors[J]. Int J Soc Psychiatry, 2017, 63(4): 359-375. DOI:10.1177/0020764017700175 |
| [30] |
Adrian M, McCauley E, Berk MS, et al. Predictors and moderators of recurring self-harm in adolescents participating in a comparative treatment trial of psychological interventions[J]. J Child Psychol Psychiatry, 2019, 60(10): 1123-1132. DOI:10.1111/jcpp.13099 |
| [31] |
Zahn-Waxler C, Shirtcliff EA, Marceau K. Disorders of childhood and adolescence: gender and psychopathology[J]. Annu Rev Clin Psychol, 2008, 4: 275-303. DOI:10.1146/annurev.clinpsy.3.022806.091358 |
| [32] |
陈洁, 刘金同, 王旸, 等. 有自杀意念高中生的情绪和行为问题及与家庭环境的关系[J]. 中国儿童保健杂志, 2013, 21(6): 587-590. Chen J, Liu JT, Wang Y, et al. Study on emotional and behavioral problems among the high school students with suicidal ideation and their relations with family environment[J]. Chin J Child Health Care, 2013, 21(6): 587-590. |
| [33] |
Guo L, Wang WX, Wang T, et al. Association of emotional and behavioral problems with single and multiple suicide attempts among Chinese adolescents: modulated by academic performance[J]. J Affect Disord, 2019, 258: 25-32. DOI:10.1016/j.jad.2019.07.085 |
| [34] |
Piqueras JA, Soto-Sanz V, Rodríguez-Marín J, et al. What is the role of internalizing and externalizing symptoms in adolescent suicide behaviors?[J]. Int J Environ Res Public Health, 2019, 16(14): 2511. DOI:10.3390/ijerph16142511 |
| [35] |
Soto-Sanz V, Castellví P, Piqueras JA, et al. Internalizing and externalizing symptoms and suicidal behaviour in young people: a systematic review and Meta-analysis of longitudinal studies[J]. Acta Psychiatr Scand, 2019, 140(1): 5-19. DOI:10.1111/acps.13036 |
| [36] |
Sigfusdottir ID, Asgeirsdottir BB, Gudjonsson GH, et al. Suicidal ideations and attempts among adolescents subjected to childhood sexual abuse and family conflict/violence: the mediating role of anger and depressed mood[J]. J Adolesc, 2013, 36(6): 1227-1236. DOI:10.1016/j.adolescence.2013.10.001 |
| [37] |
Rhoades KA. Children's responses to interparental conflict: a Meta-analysis of their associations with child adjustment[J]. Child Dev, 2008, 79(6): 1942-1956. DOI:10.1111/j.1467-8624.2008.01235.x |
| [38] |
Zhang J. The strain theory of suicide[J]. J Pac Rim Psychol, 2019, 13: e27. DOI:10.1017/prp.2019.19 |
| [39] |
Zhang J, Wieczorek WF, Conwell Y, et al. Psychological strains and youth suicide in rural China[J]. Soc Sci Med, 2011, 72(12): 2003-2010. DOI:10.1016/j.socscimed.2011.03.048 |
| [40] |
Lew B, Chistopolskaya K, Liu YZ, et al. Testing the strain theory of suicide-the moderating role of social support[J]. Crisis, 2020, 41(2): 82-88. DOI:10.1027/0227-5910/a000604 |