 2021, Vol. 42
2021, Vol. 42文章信息
- 张晓帆, 刘峰, 刘万普, 叶先明, 崔缤尹, 王惠君.
- Zhang Xiaofan, Liu Feng, Liu Wanpu, Ye Xianming, Cui Binyin, Wang Huijun
- 中国四省中老年人睡眠时长与抑郁症状的关联性研究
- Relationship between sleep duration and depressive symptoms in middle-aged and elderly people in four provinces of China
- 中华流行病学杂志, 2021, 42(11): 1955-1961
- Chinese Journal of Epidemiology, 2021, 42(11): 1955-1961
- http://dx.doi.org/10.3760/cma.j.cn112338-20200930-01210
-
文章历史
收稿日期: 2020-09-30




2. 陕西省疾病预防控制中心, 西安 710054;
3. 河北省沧县疾病预防控制中心 061000;
4. 庆元县疾病预防控制中心 323800;
5. 湖南省衡阳市疾病预防控制中心 421001
2. Shaanxi Provincial Centre for Disease Control and Prevention, Xi'an 710054, China;
3. Cangxian County Center for Disease Control and Prevention, Cangxian 061000, China;
4. Qingyuan County Center for Disease Control and Prevention, Qingyuan 323800, China;
5. Hengyang Prefectural Center for Disease Control and Prevention, Hengyang 421001, China
抑郁症是一种常见的精神障碍,也是全球范围内导致残疾的主要原因之一。2017年全球疾病负担报告指出,在全球范围内,超过2.64亿的人都患有抑郁症[1]。在中国,约40%的≥60岁老年人有抑郁症状[2]。抑郁症会严重损害人们工作或学习的能力以及应对日常生活的能力,严重时甚至可能导致自杀,抑郁症的预防和治疗已成为公共卫生领域的热门话题。睡眠作为非常重要的健康相关因素,近期引起学者越来越多的关注。研究表明,睡眠时间对总死亡率、心血管疾病、代谢综合征等常见的慢性病有很大影响[3-5]。也有研究探索了睡眠时间与抑郁症状的关系,但结果并不一致。一些研究显示,睡眠时间与抑郁症状存在U形关联[6-7],而其他研究仅发现睡眠不足与抑郁症状有关[8-9]。因此,睡眠时长与抑郁症状的关系需要进一步研究予以证实。本研究利用“神经系统疾病专病社区队列研究”2018年基线调查数据,分析中国四省≥55岁中老年人睡眠时长与抑郁症状的关系,为相关预防策略提供科学依据。
对象与方法1.研究对象:本研究数据来源于“神经系统疾病专病社区队列研究”的2018-2019年基线调查数据。由中国CDC营养与健康所牵头,河北医科大学、浙江省CDC、陕西省CDC及湖南省CDC共同合作,采用分层多阶段整群随机抽样的方法,在河北、浙江、陕西及湖南省,每个省抽取2个城市点及2个县城点,每个城市点选择1个城市居委会和1个郊区村,每个县城点选择1个县城居委会和1个农村。2018-2019年完成了基线调查,包括问卷调查、体格测量与血液采集。本研究中调查对象的纳入标准:①常住人口或计划暂时离开居住地 < 1个月的人口;②≥55岁;③未患阿尔茨海默病(AD)、帕金森病(PD)和癫痫。排除标准:①先天或后天因素引起的智障者;②听力或视力不正常且佩戴矫正工具仍无法保证听力和视力正常者。在上述纳入和排除标准上,进一步将年龄、性别、睡眠时长及老年抑郁量表得分缺失或异常者820人剔除,最终纳入的样本量为11 931人。其中男性占43.03%,女性占56.97%。该课题已通过中国CDC营养与健康所伦理审查委员会的审查(No. 2017-020),所有调查对象在调查前均签署了知情同意书。
2.研究方法:①问卷调查:由经过统一培训且合格的调查员进行面对面询问调查,包括住户调查和个人调查两个部分,住户调查问卷内容包括家庭成员基本情况、家庭收入等信息;个人调查问卷内容包括地区、性别、年龄、文化程度、职业等人口学信息,吸烟、饮酒、睡眠时长、身体活动等生活方式信息,食物频率问卷调查,高血压、糖尿病等既往疾病史和用来筛查抑郁症状的老年抑郁量表(GDS-30)等。调查后由调查点负责人进行数据核查,确保调查质量。②体格测量:由经过统一培训且合格的调查员采用统一的器械测量调查对象的身高和体重。身高测量统一采用SECA206型卷筒式量高尺,体重测量统一采用SECA882型电子秤。身高以cm单位,保留小数点后1位;体重以kg为单位,保留小数点后1位。根据公式:BMI(kg/m2)=体重(kg)/身高2(m2)计算每位受试者的BMI值。
3.指标和定义:①抑郁症状的评价方法:采用1982年专门为老年人设计的老年抑郁量表(Geriatric depression scale,GDS)筛查抑郁症状[10-11],信效度研究证明其中文版量表内部一致性和稳定性较好[12]。该量表由30个条目组成,每个条目均为“是”“否”二分类回答。选择代表“有抑郁表现”的答案记1分,选择代表“无抑郁表现”的答案记0分,总分范围为0~30分,分值越高代表抑郁症状越严重。使用量表发明者推荐的且大多数研究中使用的11分作为筛选有抑郁症状的切点值[11, 13]。②睡眠时长:本研究中的睡眠时长源于研究对象的自报数据,指包括晚上和白天,每天通常的睡眠时间,受访者只能以1h为单位进行报告。本研究将自报睡眠时长分为≤5、6、7~8和≥9h组,依据美国国家睡眠基金会的推荐[14],以睡眠时间7~8h为参照组。
4.其他协变量:社会人口经济学变量包括地区、年龄、性别、文化程度、工作情况和家庭人均月收入,其中,地区分为城市和农村两组,将城市点的城市居委会和县城点中的县城居委会合并为城市,将城市点中的郊区村和县城点中的农村合并为农村;文化程度是指研究对象已经完成学业、毕业获国家承认的最高文凭学历,分为小学以下、小学、初中和高中及以上组。生活方式变量包括吸烟、饮酒、身体活动、饮茶和咖啡情况,其中,中高强度身体活动量是指代谢当量≥3METs的各类身体活动量,包括职业性、家务性、交通性和休闲性4大类;吸烟是指平均每天吸≥1支烟,否则为不吸烟,以前吸烟现在不吸烟则为以前吸,现在仍然吸烟则为现在吸;饮酒是指过去1年喝过啤酒、白酒或其他酒精饮料,具体分为每周 < 1次和每周≥1次。根据标准的食物频率问卷(FFQ)调查过去1年研究对象饮茶和咖啡的频率,分为不饮、每周不到1次和每周≥ 1次。身体健康状况包括高血压、糖尿病患病情况和BMI,根据医生是否曾经给出相关疾病的临床诊断判定研究对象是否有高血压和糖尿病。
5.统计学分析:采用SAS9.4软件进行数据的清理和分析。研究对象基本特征中分类变量采用例数和百分比描述,连续变量采用x±s和M(四分位数间距)描述。不同抑郁症状研究对象的组间比较,分类变量采用χ2检验,连续性变量为非正态分布,采用Wilcoxon秩和检验。睡眠时长与抑郁症状的关联性分析采用限制性立方样条模型和多因素logistic回归分析。检验水准α=0.05,双侧P < 0.05为差异有统计学意义。
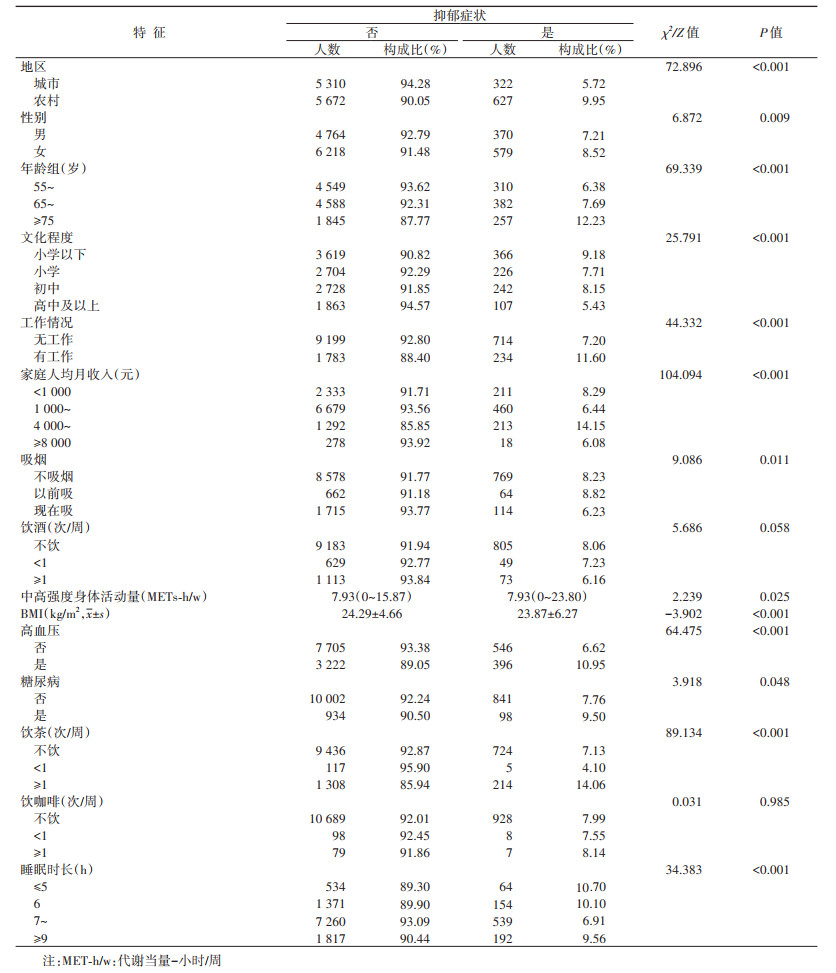
结果1.基本情况:本研究共纳入≥55岁中老年人11931人,其中男性5134人,占43.03%,女性6797人,占56.97%;55~64岁中老年人4859人,占40.73%,65~74岁老年人4970人,占41.66%,≥75岁老年人2102人,占17.62%。17.79%的中老年人睡眠时长 < 7h,16.84%的中老年人睡眠时间≥9h。其中,女性(19.32%)睡眠不足7h的比例高于男性(15.78%);随着年龄的增长,睡眠不足7h的比例逐渐增加,从15.25%上升到23.60%。利用GDS-30共检出7.95%的中老年人患有抑郁症状。见表 1。

2.不同抑郁症状中老年人特征分布:被调查的中老年人中,9.95%的农村中老年人检出抑郁症状,高于城市中老年人(5.72%);8.52%的女性检出抑郁症状,高于男性(7.21%);随年龄增长,抑郁症状检出比例逐渐增加,从6.38%上升到12.23%;有工作的中老年人(11.60%)抑郁症状检出率高于无工作者(7.20%);10.95%的高血压患者检出抑郁症状,高于非高血压患者(6.62%);饮茶≥1次/周的中老年人抑郁症状检出率最高,为14.06%;睡眠时长为7~8h的中老年人抑郁症状检出率最低,为6.91%,睡眠时长低于或高于7~8h的中老年人抑郁症状检出率均增加。不同地区、性别、年龄、文化程度、工作情况、家庭人均月收入、吸烟、高血压、糖尿病、中高强度身体活动量、BMI、饮茶频率和睡眠时长间,中老年人群抑郁症状的检出率不同,差异均有统计学意义(P < 0.05)。见表 2。
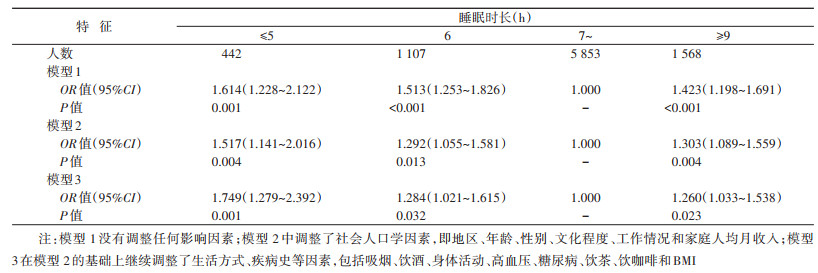
3.老年人睡眠时长与抑郁症状的关系:以是否患抑郁症状为因变量,采用限制性立方样条模型分析,调整了地区、年龄、性别、文化程度、工作情况和家庭人均月收入、吸烟、饮酒、身体活动、高血压、糖尿病、饮茶、饮咖啡和BMI情况后,结果显示睡眠时间与抑郁症状的患病风险存在U形关联(χ2=17.41,P < 0.001,自由度=2),非线性剂量反应关系有统计学意义(χ2=10.62,P=0.001,自由度=1)。见图 1。单因素logistic分析结果显示,睡眠时间与抑郁症状存在关联(P < 0.05);在调整了地区、年龄等因素后,多因素logistic分析结果显示,与睡眠7~8h相比,睡眠时长为≤5h、6h和≥9h的≥55岁中老年人患抑郁症状的风险分别是前者的1.749倍、1.284倍和1.260倍,差异均有统计学意义(P < 0.05)。见表 3。

|
| 图 1 中老年人睡眠时间与抑郁症状的剂量反应关系 |
分性别进行多因素logistic回归分析,调整了上述所有的混杂因素后,与睡眠7~8 h相比,男性睡眠时长与抑郁症状的关联无统计学意义(P>0.05),女性睡眠时长≤5 h、6 h和≥9 h患抑郁症状的风险分别是前者的2.115倍、1.605倍和1.313倍,差异均有统计学意义(P < 0.05)。见表 4。
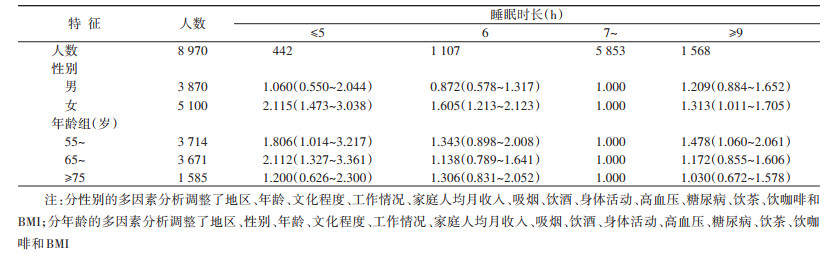
分年龄进行多因素logistic回归分析,调整了所有混杂因素后,与睡眠7~8h相比,55~64岁中老年人睡眠时长≤5h和≥9h患抑郁症状的风险分别是前者的1.806倍和1.478倍;65~74岁中老年人睡眠时长≤5h患抑郁症状的风险是前者的2.112倍,差异均有统计学意义(P < 0.05)。≥75岁中老年人睡眠时长与抑郁症状的关联无统计学意义(P>0.05)。见表 4。
讨论在这个横断面研究中,我们发现睡眠时间较短(≤6h)或较长(≥9h)均与抑郁症状风险增加有关,而且在调整了社会人口学因素、生活方式、饮食及健康状况等诸多相关混杂因素后,这一关联仍有统计学意义,自报睡眠时长与≥55岁中老年人抑郁症状存在U形关联,这与多个国内外研究结果一致[6-7, 15-16]。Sun等[6]对512891名30~79岁中国居民的研究(睡眠不足OR=2.32,95%CI:2.14~2.51;睡眠较长OR=1.56,95%CI:1.34~1.81)和Zhai等[15]对涉及7个前瞻性研究(包括6个美国的研究和1个日本的研究)进行的Meta分析(睡眠不足RR=1.31,95%CI:1.04~1.64;睡眠较长RR=1.42,95%CI:1.04~ 1.92)均显示,睡眠不足或过长与成年人抑郁症的风险增加有关,与国外相比,中国居民睡眠时间不足与抑郁的关联性更大。但Li等[8]对≥45岁中国中老年人群的纵向研究仅得出睡眠时间不足(≤6h)与抑郁症相关的结论,没有发现睡眠时间过长(>9h)与抑郁的关联。可能原因在于,Li等[8]的研究中睡眠时间仅包括夜晚睡眠时间而不是全天24h的睡眠时间,可能存在午睡时间的影响;此外,该研究中只有284个调查对象报告睡眠时间≥9h,可能由于样本量较小导致睡眠时间过长无关联的结果。另外,本研究对性别和年龄进行分组分析后,发现对于女性和55~74岁人群,睡眠时间与抑郁发生的风险有关;而对于男性和≥75岁人群,睡眠时长与抑郁症状无关联;提示睡眠时间与抑郁症状的关联可能存在性别和年龄上的差异。目前缺乏不同性别、不同年龄段中老年人睡眠时长与抑郁症状的关联性研究,需进一步研究来证实。
睡眠和抑郁症状之间的关联机制尚不完全清楚。一方面,睡眠不足可能增加抑郁症状发生的风险。首先,睡眠不足引起的身体或心理疲劳[17]可能破坏昼夜节律并引起激素水平的变化,从而导致抑郁的发生[18-19]。其次,越来越多的证据显示,与非抑郁人群比较,抑郁患者过短或过长的睡眠时间与体内有害物质水平升高有关,低水平的慢性炎症可能是将睡眠和抑郁症状关联起来的关键生物学途径[20-21]。再者,一些研究人员发现,较短的睡眠时间可能是精神障碍的前兆[22]。而且,睡眠不足会导致抑郁,抑郁也会导致睡眠不足,二者在因果关系上相互作用、相互促进,从而会进一步加重抑郁和睡眠问题。另一方面,长时间的睡眠与身体活动水平较低有关[23],而身体活动可以通过增加神经递质(特别是多巴胺和5-羟色胺)的水平,增强大脑胺能突触传递[24],增加内啡肽分泌[25],缓解压力刺激[26],或提高自我效能和自尊[27]来降低抑郁发生的风险。未来有必要进一步研究睡眠时间与抑郁症状相关的潜在生物学机制。
本研究存在一定的局限性。首先,横断面研究无法得出因果关联;其次,睡眠时间源于研究对象自报数据而非客观测量,可能存在测量误差;但已有研究显示,自我报告的睡眠时间同样可以可靠地预测死亡率和其他健康结局[28-29]。另外,本研究只考虑到睡眠的一个方面,缺乏关于睡眠质量、睡眠潜伏期、睡眠障碍等其他睡眠相关的重要信息,可能会对结果产生一定的影响。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017:a systematic analysis for the Global Burden of Disease study 2017[J]. Lancet, 2018, 392(10159): 1789-1858. DOI:10.1016/S0140-6736(18)32279-7 |
| [2] |
Ni YH, Tein JY, Zhang MQ, et al. Changes in depression among older adults in China: A latent transition analysis[J]. J Affect Disord, 2017, 209: 3-9. DOI:10.1016/j.jad.2016.11.004 |
| [3] |
Liu TZ, Xu C, Rota M, et al. Sleep duration and risk of all-cause mortality: A flexible, non-linear, Meta-regression of 40 prospective cohort studies[J]. Sleep Med Rev, 2017, 32: 28-36. DOI:10.1016/j.smrv.2016.02.005 |
| [4] |
Covassin N, Singh P. Sleep duration and cardiovascular disease risk: epidemiologic and experimental evidence[J]. Sleep Med Clin, 2016, 11(1): 81-89. DOI:10.1016/j.jsmc.2015.10.007 |
| [5] |
Smiley A, King D, Bidulescu A. The association between sleep duration and metabolic syndrome: the NHANES 2013/2014[J]. Nutrients, 2019, 11(11): 2582. DOI:10.3390/nu11112582 |
| [6] |
Sun XY, Zheng B, Lv J, et al. Sleep behavior and depression: Findings from the China Kadoorie Biobank of 0.5 million Chinese adults[J]. J Affect Disord, 2018, 229: 120-124. DOI:10.1016/j.jad.2017.12.058 |
| [7] |
Jiang MH, Guo XF, Sun YX. Association between sleep time and depression: a cross-sectional study from countries in rural Northeastern China[J]. J Int Med Res, 2017, 45(3): 984-992. DOI:10.1177/0300060517701034 |
| [8] |
Li YJ, Wu YL, Zhai L, et al. Longitudinal association of sleep duration with depressive symptoms among middle-aged and older Chinese[J]. Sci Rep, 2017, 7(1): 11794. DOI:10.1038/s41598-017-12182-0 |
| [9] |
Berger AT, Wahlstrom KL, Widome R. Relationships between sleep duration and adolescent depression: a conceptual replication[J]. Sleep Health, 2019, 5(2): 175-179. DOI:10.1016/j.sleh.2018.12.003 |
| [10] |
Brink TL, Yesavage JA, Lum O, et al. Screening tests for geriatric depression[J]. Clin Gerontol, 1982, 1(1): 37-43. DOI:10.1300/J018v01n01_06 |
| [11] |
Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: A preliminary report[J]. J Psychiatr Res, 1982-1983, 17(1): 37-49. DOI:10.1016/0022-3956(82)90033-4 |
| [12] |
孙晓艳, 李怡雪, 余灿清, 等. 中文版抑郁量表信效度研究的系统综述[J]. 中华流行病学杂志, 2017, 38(1): 110-116. Sun XY, Li YX, Yu CQ, et al. Reliability and validity of depression scales of Chinese version: a systematic review[J]. Chin J Epidemiol, 2017, 38(1): 110-116. DOI:10.3760/cma.j.issn.0254-6450.2017.01.021 |
| [13] |
Hickie C, Snowdon J. Depression scales for the elderly: GDS, Gilleard, Zung[J]. Clin Gerontol, 1987, 6(3): 51-53. |
| [14] |
Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation's updated sleep duration recommendations: final report[J]. Sleep Health, 2015, 1(4): 233-243. DOI:10.1016/j.sleh.2015.10.004 |
| [15] |
Zhai L, Zhang H, Zhang DF. Sleep duration and depression among adults: a Meta-analysis of prospective studies[J]. Depr Anxiety, 2015, 32(9): 664-670. DOI:10.1002/da.22386 |
| [16] |
翟龙. 成年人睡眠时间与抑郁关系的研究[D]. 青岛: 青岛大学, 2015. Zhai L. Research on the relationship between adult sleep time and depression[D]. Qingdao: Qingdao University, 2015. |
| [17] |
Shen JH, Barbera J, Shapiro CM. Distinguishing sleepiness and fatigue: focus on definition and measurement[J]. Sleep Med Rev, 2006, 10(1): 63-76. DOI:10.1016/j.smrv.2005.05.004 |
| [18] |
Luik AI, Zuurbier LA, Direk N, et al. 24-hour activity rhythm and sleep disturbances in depression and anxiety: a population-based study of middle-aged and older persons[J]. Depr Anxiety, 2015, 32(9): 684-692. DOI:10.1002/da.22355 |
| [19] |
van Noorden MS, van Fenema EM, van der Wee NJA, et al. Predicting outcome of depression using the depressive symptom profile: the Leiden Routine Outcome Monitoring Study[J]. Depr Anxiety, 2012, 29(6): 523-530. DOI:10.1002/da.21958 |
| [20] |
Prather AA, Vogelzangs N, Penninx BWJH. Sleep duration, insomnia, and markers of systemic inflammation: results from the Netherlands Study of Depression and Anxiety (NESDA)[J]. J Psychiatr Res, 2015, 60: 95-102. DOI:10.1016/j.jpsychires.2014.09.018 |
| [21] |
Hall MH, Smagula SF, Boudreau RM, et al. Association between sleep duration and mortality is mediated by markers of inflammation and health in older adults: the Health, Aging and Body Composition Study[J]. Sleep, 2015, 38(2): 189-195. DOI:10.5665/sleep.4394 |
| [22] |
Judd LL, Akiskal HS, Maser JD, et al. A prospective 12-year study of subsyndromal and syndromal depressive symptoms in unipolar major depressive disorders[J]. Arch Gen Psychiatry, 1998, 55(8): 694-700. DOI:10.1001/archpsyc.55.8.694 |
| [23] |
Stranges S, Dorn JM, Shipley MJ, et al. Correlates of short and long sleep duration: a cross-cultural comparison between the United Kingdom and the United States: the Whitehall Ⅱ Study and the Western New York Health Study[J]. Am J Epidemiol, 2008, 168(12): 1353-1364. DOI:10.1093/aje/kwn337 |
| [24] |
Weicker H, Strüder HK. Influence of exercise on serotonergic neuromodulation in the brain[J]. Amino Acids, 2001, 20(1): 35-47. DOI:10.1007/s007260170064 |
| [25] |
Janal MN, Colt EWD, Clark WC, et al. Pain sensitivity, mood and plasma endocrine levels in man following long-distance running: effects of naloxone[J]. Pain, 1984, 19(1): 13-25. DOI:10.1016/0304-3959(84)90061-7 |
| [26] |
Salmon P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory[J]. Clin Psychol Rev, 2001, 21(1): 33-61. DOI:10.1016/s0272-7358(99)00032-x |
| [27] |
Paluska SA, Schwenk TL. Physical activity and mental health: current concepts[J]. Sports Med, 2000, 29(3): 167-180. DOI:10.2165/00007256-200029030-00003 |
| [28] |
Gangwisch JE, Malaspina D, Boden-Albala B, et al. Inadequate sleep as a risk factor for obesity: analyses of the NHANES Ⅰ[J]. Sleep, 2005, 28(10): 1289-1296. DOI:10.1093/sleep/28.10.1289 |
| [29] |
Kripke DF, Garfinkel L, Wingard DL, et al. Mortality associated with sleep duration and insomnia[J]. Arch Gen Psychiatry, 2002, 59(2): 131-136. DOI:10.1001/archpsyc.59.2.131 |