 2021, Vol. 42
2021, Vol. 42文章信息
- 薛晓丹, 江国虹, 李威, 张颖, 李丹丹, 解美秋, 王德征.
- Xue Xiaodan, Jiang Guohong, Li Wei, Zhang Ying, Li Dandan, Xie Meiqiu, Wang Dezheng
- 1999-2018年天津市居民出血型脑卒中发病流行特征研究
- Epidemiological characteristics of hemorrhagic stroke among residents in Tianjin from 1999 to 2018
- 中华流行病学杂志, 2021, 42(8): 1460-1465
- Chinese Journal of Epidemiology, 2021, 42(8): 1460-1465
- http://dx.doi.org/10.3760/cma.j.cn112338-20201028-01288
-
文章历史
收稿日期: 2020-10-28




脑卒中是全球第二大死因,其主要亚型出血型脑卒中具有较高的病死率和致残率,随着预期寿命的增加,脑卒中造成的疾病负担也越来越重[1-2]。国际流行病学领域的很多研究均显示出血型脑卒中在亚洲人群和中、低收入国家高发,其流行率显著高于白人和高收入国家[3-4]。然而,随着我国经济发展和人民生活水平的提高,特别是健康中国策略和全民健康生活方式行动的实施,以及天津市在高血压管理[5]、无烟环境创建[6-8]及基本公共卫生服务等方面的投入增加[9],出血型脑卒中的主要危险因素逐步得到控制,因此研究天津市出血型脑卒中的流行特征变化成为制定预防策略和评价防治效果的核心基础。本研究对1999-2018年天津市出血型脑卒中发病数据进行分析,为进一步制定精准防控对策提供数据支持。
资料与方法1. 资料来源:于1999-2018年天津市慢性非传染病发病监测系统收集的出血型脑卒中监测数据[10]。监测诊断分类按照《疾病和有关健康问题的国际统计分类》(ICD-10)编码:I61(2002年以前使用ICD-9编码,431),并参考WHO多国心血管病趋势及决定因素研究中的定义[11],其发病的期限定义为急性发病后28 d,28 d后复发再住院记为另一次新发病事件。以病例入院日期为分析时间点。根据地理位置、经济水平、非农业人口数量等因素将天津市的16个行政区划为7个城市地区和9个农村地区。天津市户籍人口数来源于天津市公安局人口管理办公室。
根据脑卒中首诊报告卡的要求,收集病例一般信息,包括姓名、性别、年龄、户籍、民族、职业、现住址、诊断依据、发病时间、个人吸烟情况、填报日期等。由培训后的监测医生按照统一方式填报监测报告,当地CDC整理并上报给市CDC。
2. 质量控制与评价:根据天津市CDC对各辖区疾病控制考核的要求,心脑血管发病监测逻辑核查和查重的错误率 < 1%,每月对上报数据进行审核。年初对上一年度全年数据库进行核查,历年错误率均 < 1%。2011年开展了基于医院原始病历的天津市慢性非传染病发病监测(2010年)漏报调查,在调查的9 769例原始病例按照身份证号码、姓名、性别、年龄和街道等匹配策略与监测数据库进行比对,共有43例未报告,总漏报率为4.88%[12]。
3.统计学分析:采用SPSS 19.0软件进行统计学分析,计算发病率。以2010年全国第六次人口普查为标准人口计算标化发病率。率和构成比的比较采用χ2检验。采用SAS 8.0软件进行趋势χ2检验(统计量为Z值),分析发病率的时间趋势和年龄趋势;并通过正态近似法,估计发病率的95%CI。采用Joinpoint软件对年发病率的变化进行分析。双侧检验,以P < 0.05为差异有统计学意义。
结果1. 一般情况:研究期间,共有出血型脑卒中新发病例117 903例,占全部脑卒中病例的13.08%,且出血型脑卒中占比逐年下降(P < 0.01)。男性发病数高于女性,男女发病比为1.61∶1;城市发病高于农村,城乡发病比为1.20∶1。≥65岁老年人占总体构成的47.98%。
1999-2018年天津市居民出血型脑卒中粗发病率最高为75.38/10万,最低为46.70/10万,呈下降趋势(Z=-28.63,P < 0.01,APC=-1.45%)。经过年龄、性别调整后,标化发病率为57.93/10万~27.55/10万,均呈下降趋势(Z=-54.72,P < 0.01,APC=-3.38%)。见表 1。

2. 不同性别、年龄人群出血型脑卒中发病率:研究期间男性出血型脑卒中粗发病率为87.55/10万~60.28/10万,呈下降趋势(Z=-13.35,P < 0.01,APC=-0.87%),标化发病率为65.02/10万~35.70/10万,呈下降趋势(Z=-32.40,P < 0.01,APC=-2.57%);女性出血型脑卒中发病率为62.96/10万~33.03/10万,呈下降趋势(Z=-28.85,P < 0.01,APC=-2.34%),标化发病率为50.39/10万~18.88/10万,呈下降趋势(Z=-47.71,P < 0.01,APC=-4.75%)。见表 1。
20年间男、女性出血型脑卒中粗发病率、标化发病率均呈下降趋势,且在各年份及各年龄组男性发病率均高于女性(P < 0.01),发病率随年龄的增加而升高(P < 0.01)。见表 1。
分年龄别中,< 45岁年龄组发病率呈上升趋势(P < 0.01),而≥45岁年龄组发病率呈下降趋势(P < 0.01)。在男性中,< 55岁年龄组发病率呈上升趋势(P < 0.01),≥55岁年龄组发病率呈下降趋势(P < 0.01);而在女性中,仅 < 35岁年龄组发病率呈上升趋势(P < 0.01),其余年龄组发病率均呈下降趋势(P < 0.01)。出血型脑卒中发病率呈低龄化趋势。见表 1。
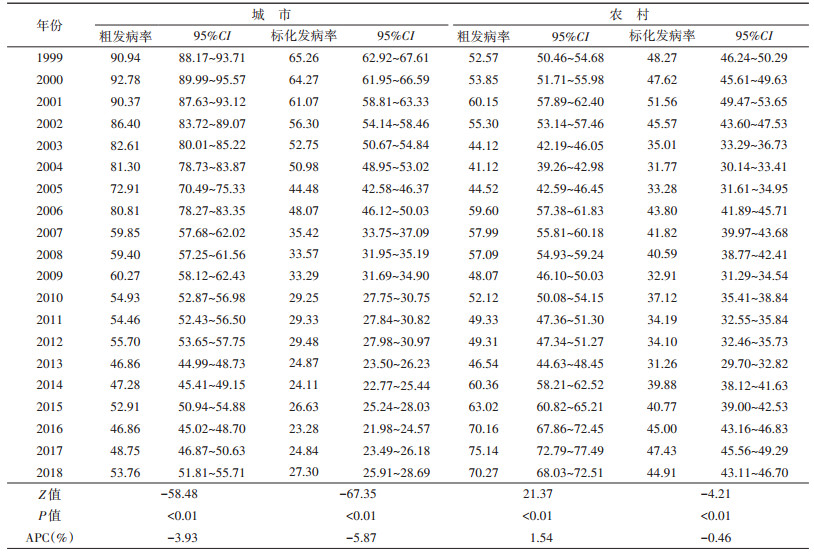
3. 不同地区人群出血型脑卒中发病率:1999-2018年天津市城市地区出血型脑卒中粗发病率为92.78/10万~46.86/10万,总体呈下降趋势(Z=-58.48,P < 0.01,APC=-3.93%),标化发病率为65.26/10万~23.28/10万,总体呈下降趋势(Z=-67.35,P < 0.01,APC=-5.87%);农村地区出血型脑卒中粗发病率为41.12/10万~75.14/10万,呈上升趋势(Z=21.37,P < 0.01,APC=1.54%),标化发病率为48.27/10万~31.26/10万,呈下降趋势(Z=-4.21,P < 0.01,APC=-0.46%)。见表 2。
本研究结果显示,1999-2018年天津市出血型脑卒中标化发病率呈下降趋势。在中国的MONICA研究中[13],1984-2004年北京市出血型脑卒中发病率自80.7/10万下降至35.2/10万,平均每年下降1.7%,另外中国3个城市研究中,20世纪90年代北京市出血型脑卒中标化发病率为38.1/10万,上海市发病率为27.1/10万,长沙市发病率为77.1/10万[14]。天津市出血型脑卒中标化发病水平与北京市类似,介于上海市与长沙市之间。而20年间出血型脑卒中发病占比由26.68%下降至7.88%。
美国、英国、澳大利亚出血型脑卒中占比约为8%~15%[15-16],在日本和韩国约为18%~24%[17-18]。出血型脑卒中标化发病率由57.93/10万下降至35.52/10万,国内外对于出血型脑卒中的发病趋势研究结果并不一致。在2013年发表的涉及全球119个国家(地区)缺血型脑卒中和出血型脑卒中疾病负担研究表明,自1990-2010年发达国家出血型脑卒中发病率呈下降趋势(53.30/10万~49.12/10万),而绝大部分发展中国家出血型脑卒中发病率呈上升趋势(81.40/10万~99.43/10万)[19],与此相同结论的还有法国[20]、英国(1981-2004年)[21]等研究。由此发现中国天津市出血型脑卒中发病特征与发达国家近似。
分性别研究中,20年间男、女性出血型脑卒中粗发病率、标化发病率均呈下降趋势,女性下降趋势更加明显,且在各年份及各年龄组男性发病率均高于女性,这与MONICA中国研究结论一致[15]。在分年龄别分析中发现,虽然总体出血型脑卒中发病呈下降趋势,但 < 45岁人群的发病率呈上升趋势,这种趋势在男性低年龄组中更加明显,提示出血型脑卒中发病呈低龄化趋势。分地区分析中,城市、农村地区均呈下降趋势,而城市地区下降趋势更加明显。因此,在未来实施干预策略中,应更加注重低年龄组及农村人群。
出血型脑卒中通常是由继发于高血压变化或其他血管异常的穿透性动脉破裂引起的脑内出血,高血压、吸烟、腰臀比、饮食和高乙醇摄入量是出血型脑卒中的主要危险因素,这些可改变的危险因素占人口归因风险的88.1%[22]。除此之外,出血型脑卒中发病趋势还与当地公共卫生政策实施效果相关[23]。天津市自2008年以来开展全民健康生活方式行动,同期基本公共卫生服务项目高血压患者社区健康管理开始实施,高血压控制率自2006年14.76%[24]上升至2015年的27.58%[数据来自《天津市成人居民营养与健康状况综合报告(2018年)》]。另一方面,天津市吸烟率20年来一直呈下降趋势[25],且2012年《天津市控制吸烟条例》出台[6],一系列健康措施及公共政策极大促进了公众健康行为的形成,使其主要危险因素逐步得到控制。未来人口老龄化问题仍然严峻,而与脑卒中相关的公共卫生负担仍会进一步加剧。脑卒中亚型构成比的改变,提示危险因素的变化、医疗资源配置、预防措施的推广、医保政策的调整等都需要做相应改变,对于精准防控脑卒中、降低疾病负担和医疗成本都有意义。未来应继续大力开展全民健康生活方式行动及相关政策干预,对重点人群开展有针对性的综合措施,进一步降低脑卒中的发病水平。
本研究存在局限性。数据监测过程中经历数次新旧报告卡更新及医院电子病案系统变更,尽管变更后进行系统数据补漏,但数据庞大难免存在疏漏,未来应加大数据质控力度,提高数据质量。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
O'Donnell M, Yusuf S. Tackling the global burden of stroke: the need for large-scale international studies[J]. Lancet Neurol, 2009, 8(4): 306-307. DOI:10.1016/S1474-4422(09)70024-9 |
| [2] |
Feigin VL. Stroke in developing countries: can the epidemic be stopped and outcomes improved?[J]. Lancet Neurol, 2007, 6(2): 94-97. DOI:10.1016/S1474-4422(07)70007-8 |
| [3] |
Krishnamurthi RV, Moran AE, Forouzanfar MH, et al. The global burden of hemorrhagic stroke: a summary of findings from the GBD 2010 study[J]. Glob Heart, 2014, 9(1): 101-106. DOI:10.1016/j.gheart.2014.01.003 |
| [4] |
An SJ, Kim TJ, Yoon BW. Epidemiology, risk factors, and clinical features of intracerebral hemorrhage: an update[J]. J Stroke, 2017, 19(1): 3-10. DOI:10.5853/jos.2016.00864 |
| [5] |
杨文秀, 闫娟, 李鹏, 等. 天津市以社区为基础开展慢性病控制管理的策略[J]. 医学与社会, 2009, 22(8): 4-6. Yang WX, Yan J, Li P, et al. Strategies of community-based chronic disease control and management in Tianjin[J]. Med Soc, 2009, 22(8): 4-6. DOI:10.3870/YXYSH.2009.08.002 |
| [6] |
江国虹, 李威, 郑文龙, 等. 《天津市控制吸烟条例》实施效果的综合评价[J]. 中华流行病学杂志, 2015, 36(6): 561-564. Jiang GH, Li W, Zheng WL, et al. Comprehensive assessment on the outcome of Tianjin Act of Tobacco Control[J]. Chin J Epidemiol, 2015, 36(6): 561-564. DOI:10.3760/cma.j.issn.0254-6450.2015.06.005 |
| [7] |
教育部、卫生部. 关于进一步加强学校控烟工作的意见[EB/OL]. (2010-07-13). http://www.gov.cn/gzdt/2010-07/13/content_1653147.htm. Ministry of Education, Ministry of Health. Opinions on Further Strengthening tobacco control in schools[EB/OL]. (2010-07-13). http://www.gov.cn/gzdt/2010-07/13/content_1653147.htm. |
| [8] |
国家卫生健康委, 国家中医药局. 关于进一步加强无烟医疗卫生机构建设工作的通知[EB/OL]. (2020-07-23)[2020-08-03]. http://www.gov.cn/zhengce/zhengceku/2020-08/04/content_5532281.htm. Health Commission of China, State Administration of Traditional Chinese Medicine. Notice on further strengthening the construction of smokeless medical and health institutions[EB/OL]. (2020-07-23)[2020-08-03]. http://www.gov.cn/zhengce/zhengceku/2020-08/04/content_5532281.htm. |
| [9] |
天津市卫生局, 天津市财政局. 关于加强天津市社区公共卫生项目投入与管理的意见[EB/OL]. (2006-09-22). http://www.gov.cn/gzdt/2006-09/22/content_395693.htm. Tianjin Health Bureau, Tianjin Finance Bureau. Opinions on strengthening investment and management of community public health projects in Tianjin[EB/OL]. (2006-09-22). http://www.gov.cn/gzdt/2006-09/22/content_395693.htm. |
| [10] |
江国虹, 薛晓丹, 王德征, 等. 天津市心脑血管疾病发病监测系统的评价研究[J]. 疾病监测, 2018, 33(8): 685-689. Jiang GH, Xue XD, Wang DZ, et al. Assessment study of cardio-cerebrovascular disease surveillance system in Tianjin[J]. Dis Surveill, 2018, 33(8): 685-689. DOI:10.3784/j.issn.1003-9961.2018.08.017 |
| [11] |
The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO Monica project principal investigators[J]. J Clin Epidemiol, 1988, 41(2): 105-114. DOI:10.1016/0895-4356(88)90084-4 |
| [12] |
王德征, 沈成凤, 张颖, 等. 天津市15年急性心肌梗死发病率变化趋势分析[J]. 中华心血管病杂志, 2017, 45(2): 154-159. Wang DZ, Shen CF, Zhang Y, et al. Fifteen-year trend in incidence of acute myocardial infarction in Tianjin of China[J]. Chin J Cardiol, 2017, 45(2): 154-159. DOI:10.3760/cma.j.issn.0253-3758.2017.02.016 |
| [13] |
Zhao D, Liu J, Wang W, et al. Epidemiological transition of stroke in China: twenty-one-year observational study from the Sino-MONICA-Beijing project[J]. Stroke, 2008, 39(6): 1668-1674. DOI:10.1161/STROKEAHA.107.502807 |
| [14] |
Jiang B, Wang WZ, Chen HL, et al. Incidence and trends of stroke and its subtypes in China: results from three large cities[J]. Stroke, 2006, 37(1): 63-68. DOI:10.1161/STROKEAHA.107.502807 |
| [15] |
Feigin VL, Lawes CM, Bennett DA, et al. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review[J]. Lancet Neurol, 2009, 8(4): 355-369. DOI:10.1016/S1474-4422(09)70025-0 |
| [16] |
Sacco S, Marini C, Toni D, et al. Incidence and 10-year survival of intracerebral hemorrhage in a population-based registry[J]. Stroke, 2009, 40(2): 394-399. DOI:10.1161/STROKEAHA.108.523209 |
| [17] |
Toyoda K. Epidemiology and registry studies of stroke in Japan[J]. J Stroke, 2013, 15(1): 21-26. DOI:10.5853/jos.2013.15.1.21 |
| [18] |
Hong KS, Bang OY, Kang DW, et al. Stroke statistics in Korea: partⅠ. Epidemiology and risk factors: a report from the korean stroke society and clinical research center for stroke[J]. J Stroke, 2013, 15(1): 2-20. DOI:10.5853/jos.2013.15.1.2 |
| [19] |
Krishnamurthi RV, Feigin VL, Forouzanfar MH, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010:findings from the Global Burden of Disease Study 2010[J]. Lancet Global Health, 2013, 1(5): e259-281. DOI:10.1016/S2214-109X(13)70089-5 |
| [20] |
Benatru I, Rouaud O, Durier J, et al. Stable stroke incidence rates but improved case-fatality in Dijon, France, from 1985 to 2004[J]. Stroke, 2006, 37(7): 1674-1679. DOI:10.1161/01.STR.0000226979.56456.a8 |
| [21] |
Rothwell PM, Coull AJ, Giles MF, et al. Change in stroke incidence, mortality, case-fatality, severity, and risk factors in Oxfordshire, UK from 1981 to 2004(Oxford Vascular Study)[J]. Lancet, 2004, 363(9425): 1925-1933. DOI:10.1016/S0140-6736(04)16405-2 |
| [22] |
O'Donnell MJ, Xavier D, Liu LS, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study[J]. Lancet, 2010, 376(9735): 112-123. DOI:10.1016/S0140-6736(10)60834-3 |
| [23] |
Mendis S. Prevention and care of stroke in low- and middle-income countries; the need for a public health perspective[J]. Int J Stroke, 2010, 5(2): 86-91. DOI:10.1111/j.1747-4949.2010.00406.x |
| [24] |
李威, 陆春梅. 天津市居民高血压病患病和控制情况调查研究[J]. 新乡医学院学报, 2010, 27(3): 253-255. Li W, Lu CM. Investigation and study on prevalence and control condition of hypertension in residents of Tianjin city[J]. J Xinxiang Med Coll, 2010, 27(3): 253-255. |
| [25] |
薛晓丹, 江国虹, 李威, 等. 天津市城区居民吸烟现状及20年间吸烟行为模式的改变[J]. 中华流行病学杂志, 2019, 40(9): 1095-1098. Xue XD, Jiang GH, Li W, et al. Status quo on smoking and related change pattern of smoking related behavior in past 20 years in urban residents in Tianjin[J]. Chin J Epidemiol, 2019, 40(9): 1095-1098. DOI:10.3760/cma.j.issn.0254-6450.2019.09.014 |