 2020, Vol. 41
2020, Vol. 41文章信息
- 王晨冉, 孟显峰, 王春平, 刘世炜.
- Wang Chenran, Meng Xianfeng, Wang Chunping, Liu Shiwei
- 1990-2017年中国人群缺血性心脏病疾病负担及其危险因素变化趋势研究
- Trends of burden on ischemic heart disease and epidemiological transition of related risk factors in China, 1990-2017
- 中华流行病学杂志, 2020, 41(10): 1703-1709
- Chinese Journal of Epidemiology, 2020, 41(10): 1703-1709
- http://dx.doi.org/10.3760/cma.j.cn112338-20191018-00743
-
文章历史
收稿日期: 2019-10-18




2. 潍坊市疾病预防控制中心 261061;
3. 潍坊医学院公共卫生学院, 社会领域健康风险协同创新中心“健康山东”重大社会风险预测与治理协同创新中心 261053;
4. 中国疾病预防控制中心慢性非传染性疾病预防控制中心, 北京 100050;
5. 中国疾病预防控制中心控烟办公室, 北京 100050
2. Weifang Municipal Center for Disease Control and Prevention, Weifang 261061, China;
3. School of Public Health, Weifang Medical University, Social Health Risk Collaborative Innovation Center, "Healthy Shandong"Collaborative Innovation Center for Prediction and Governance of Major Social Risks, Weifang 261053, China;
4. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
5. Tobacco Control Office, Chinese Center for Disease Control and Prevention, Beijing 100050, China
缺血性心脏病(ischemic heart disease,IHD)即冠状动脉粥样硬化性心脏病,简称冠心病,是导致人群死亡的主要慢性非传染性疾病(non-communicable diseases,NCDs)[1]。WHO预测,2020年IHD将成为导致全球人类死亡和伤残的主要病因[2]。全球疾病负担研究(Global Burden of Disease Study,GBD)显示,2017年全球IHD的伤残调整寿命年(DALYs)约17 000万人年,在全球NCDs疾病负担中居于首位[3-4]。心血管疾病(cardiovascular disease,CVD)所致疾病负担现已成为中国严重的公共卫生问题,其中IHD是CVD疾病负担的主要来源[5]。2017年,IHD是导致我国人群死亡和早死损失寿命年(YLLs)的第二位原因,预计未来将成为我国人群的首要死因[6]。由于目前我国少有开展覆盖全国IHD疾病负担及其危险因素的综合评价研究,本研究利用GBD2017对中国的最新研究结果,探讨1990-2017年中国IHD疾病负担及其危险因素的变化趋势,为慢性病防控提出有针对性的预防策略和措施。
资料与方法1.资料来源:GBD研究是一个集人群出生和死亡(含死因)、发病与危险因素关系等健康指标、针对全世界所有国家和地区人群健康状况的统计报告[7]。GBD2017对全球不同年龄和性别人群疾病、伤害和危险因素研究进行了科学、全面的评估,提供了从1990-2017年在195个国家和地区359种疾病或伤害、84种危险因素的疾病负担数据[1, 3-4, 8]。
本研究数据来自于GBD2017对中国IHD疾病负担的估计结果[9]。GBD对我国疾病负担估计采用的死因数据主要来自中国疾病监测系统、中国妇幼卫生监测网和中国CDC死因报告等;发病和患病数据主要来自疾病监测、国家卫生服务调查、已发表的文献研究;危险因素数据主要来自慢性病与危险因素监测、国家健康和营养调查、系统综述和Meta分析等。具体研究背景在全球疾病负担报告中已有详尽描述[1, 3-4, 8]。GBD2017对中国疾病负担的估计在以往研究的基础上对数据来源、估计模型、统计分析方法等进行了更新,且遵循《准确可观的健康估计报告指南》[1-4, 8],其评估结果具有较好的全国代表性。并利用时空高斯过程回归综合数据源[8],以确保不同年代数据的可比性。本研究包括1990年、2007年、2017年中国人群IHD疾病负担数据及其归因危险因素数据。
2.疾病分类:IHD的分类以《疾病和有关健康问题的国际统计分类(第十次修订本)》(ICD-10)为标准,其疾病编码为I20~I25[1]。
3.评价指标:
(1)疾病负担的评价指标:GBD2017主要使用贝叶斯Meta回归模型DisMod-MR 2.1对非致死性疾病的疾病负担进行估计[3];用死因整体模型对死亡率和致死性疾病进行估计[4]。DALYs是一项将该人群伤残损失寿命年(YLDs)和YLLs结合起来评价疾病所致伤残和早死两方面疾病负担的综合性指标(DALYs=YLDs+YLLs)。本研究以YLDs、YLLs、DALYs作为测量IHD健康损失的主要指标[1, 3-4]。
(2)危险因素的评价指标:GBD对危险因素的归因疾病负担分析采用风险比较评估(comparative risk assessment)理论,通过反事实分析方法假定理论最小风险暴露(theoretical minimum risk exposure level,TMREL),即在其他危险因素不变的情况下,比较研究人群实际暴露与TMREL的水平,估计死亡和DALYs归因于危险因素的比例[8]。此理论下的统计指标为人群归因分值(population attributable faction,PAF),即人群归因危险度百分比。指全人群某种疾病的发病或死亡中,归因于某种危险因素暴露引起的发病或死亡占总人群全部发病或死亡的百分比。用此指标说明危险因素暴露对全人群的危害程度,以及消除此暴露后全人群发病或死亡可能降低的程度[10]。
4. IHD危险因素分类:与IHD有病因关联的可改变危险因素分为环境危险因素、行为危险因素、代谢危险因素3大类,共24种:室外颗粒物污染、室内空气污染、铅暴露;吸烟、二手烟、饮酒、蔬菜摄入不足、水果摄入不足、豆类摄入不足、谷类摄入不足、坚果摄入不足、加工肉摄入过多、含糖饮料摄入过多、纤维摄入不足、omega-3脂肪酸(促进调节血脂的多元不饱和脂肪酸)摄入不足、多不饱和脂肪酸摄入不足、反式脂肪酸摄入过多、钠摄入过多、身体活动不足;高血糖、高LDL-C(引起动脉粥样硬化的独立危险因子)、高血压、高BMI、肾脏功能受损。
5.统计学分析:采用YLDs、YLLs、DALYs对中国不同性别和年龄人群IHD所致疾病负担进行描述,同时结合PAF分析IHD归因于危险因素的疾病负担。用1990-2017年总变化率,以及1990-2007和2007-2017年的年均变化率分析IHD疾病负担的变化趋势。采用Excel软件进行数据整理和统计分析。
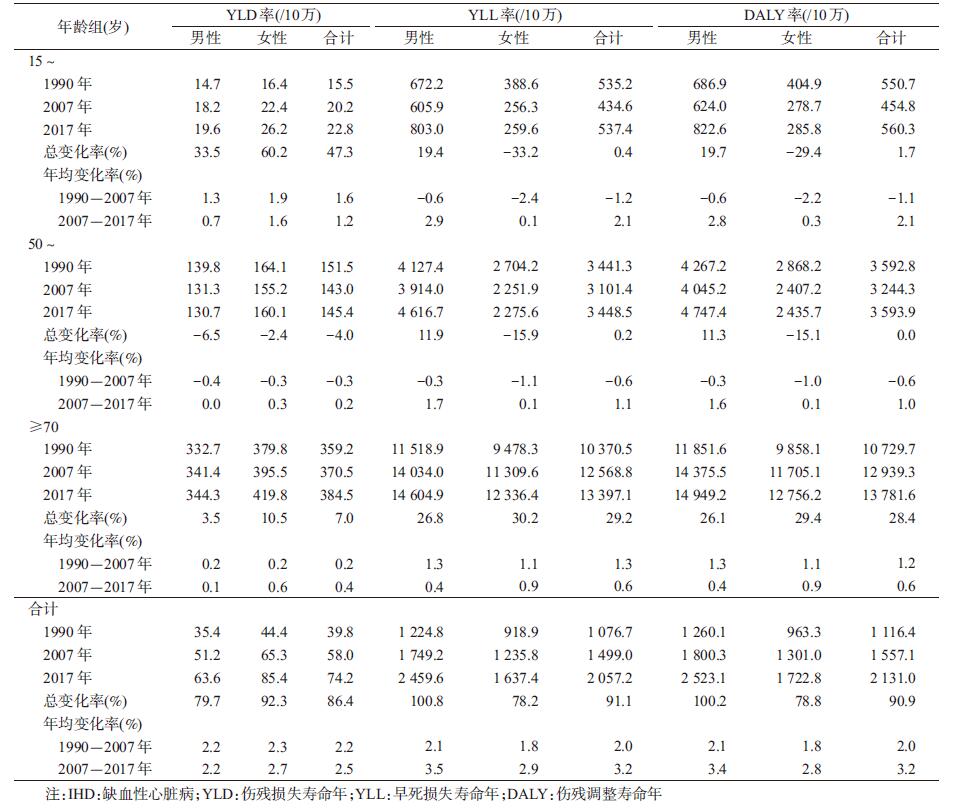
结果1. 2017年中国IHD疾病负担及危险因素归因疾病负担情况:2017年中国人群IHD的YLD率、YLL率、DALY率分别为74.2/10万、2 057.2/10万、2 131.0/10万。YLD率、YLL率、DALY率均随着年龄的增长而升高,在≥70岁人群达到峰值,分别为384.5/10万、13 397.1/10万、13 781.6/10万。IHD的YLD率为女性(85.4/10万)高于男性(63.6/10万),而YLL率和DALY率为男性(2 459.6/10万、2 523.1/10万)高于女性(1 637.4/10万、1 722.8/10万)。见表 1。
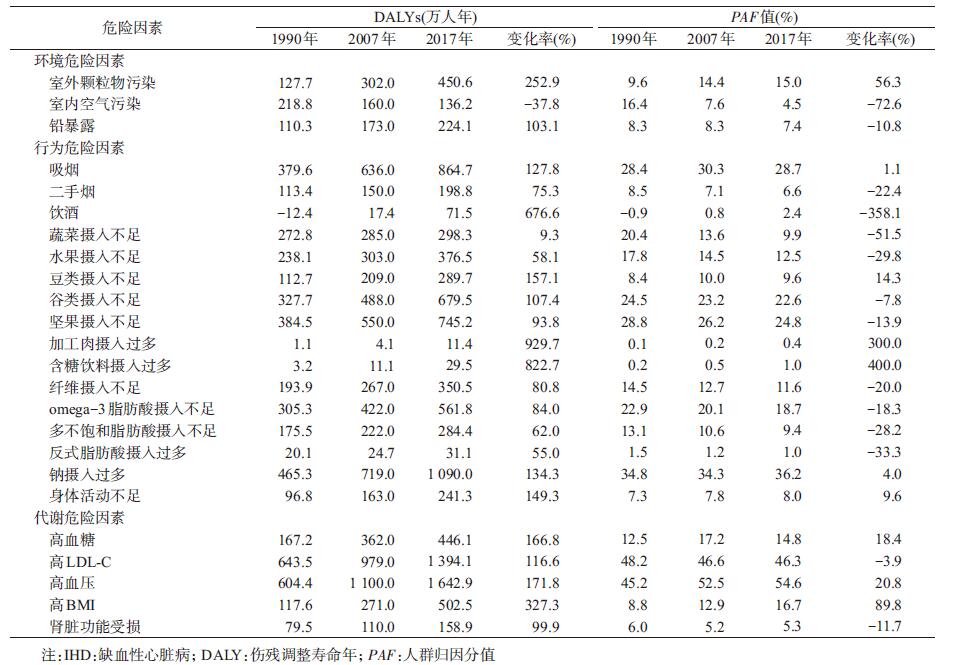
IHD的行为危险因素占比在环境(12.5%)、行为(66.7%)、代谢(20.8%)3大类24种危险因素中居于首位。2017年,DALYs、PAF、DALY率前5位的危险因素均为高血压、高LDL-C、钠摄入过多、吸烟和坚果摄入不足。见表 2,图 1。

|
| 图 1 1990-2017年中国IHD 24种危险因素DALY率(/10万)的顺位变化 |
2. 1990-2017年中国IHD疾病负担变化趋势:1990-2017年,中国人群IHD的YLD率、YLL率、DALY率均有不同幅度增长。DALY率由1990年1 116.4/10万增至2017年2 131.0/10万,增长率为90.9%。与1990年相比,2017年15~和≥70岁人群IHD的YLD率增加,且女性的增长率(60.2%、10.5%)高于男性(33.5%、3.5%)。YLL率和DALY率在男性人群中随年龄增长始终呈上升趋势,且≥70岁人群增幅最大,分别为26.8%、26.1%。≥70岁人群IHD的YLD率在2007-2017年年均增长率(0.4%)高于1990-2007年年均增长率(0.2%),但YLL率和DALY率在2007-2017年年均增长率(0.6%、0.6%)低于1990-2007年年均增长率(1.3%、1.2%)。见表 1。
3. 1990-2017年中国IHD 24种危险因素归因疾病负担变化趋势:1990-2017年仅室内空气污染的DALYs下降(-37.8%),其余23种IHD危险因素均上升,其中归因于加工肉摄入过多(929.7%)、含糖饮料摄入过多(822.7%)、高BMI(327.3%)的DALYs增幅最大。与1990年相比,2017年13种IHD危险因素的PAF上升,其中上升幅度最大的为含糖饮料摄入过多(400.0%),其次为加工肉摄入过多(300.0%)和高BMI(89.8%)。见表 2。
1990-2017年IHD 24种危险因素所致DALY率的顺位变化见图 1。与1990年相比,除蔬菜摄入不足、室内空气污染的DALY率下降外,其余22种危险因素的DALY率均增加。1990-2007年,IHD归因于高血压、吸烟、高血糖等9种危险因素的DALY率顺位上升,9种危险因素的顺位下降。2007-2017年,归因于高BMI、纤维摄入不足、豆类摄入不足等8种危险因素的DALY率顺位上升;归因于高血糖、水果摄入不足、蔬菜摄入不足等7种危险因素的顺位下降。见图 1。
讨论2017年IHD是造成中国人群死亡的第2位原因,仅次于脑卒中[11],与Yang等[12]基于GBD2010开展的中国死因分析结果相同,表明IHD仍是威胁我国人群健康的重要疾病。2017年IHD导致的YLLs约为2 905.76万人年,是其所致YLDs的27.71倍,因此早死是造成我国IHD疾病负担的主要原因[1, 3]。
研究已证实年龄能够增加IHD的患病风险[13]。本研究表明,1990-2017年我国≥70岁人群IHD疾病负担明显加重,推测人口增长和老龄化对心血管疾病的疾病负担产生了很大影响。我国不同性别人群心血管疾病的死亡率具有差异性[14],本研究发现IHD疾病负担也存在明显的性别差异。IHD对男性患者的影响主要为早死所致疾病负担,而对女性则主要为失能所致疾病负担,除了男性不良生活习惯如吸烟、酗酒、体力活动不足、职业暴露等使其心血管疾病基线死亡率高于女性外[15-18],男/女性生理差异、基因表达差异、雌激素的保护作用、女性预期寿命较男性长、更关注自己的身心健康、更积极寻求医疗卫生服务等原因也可能导致疾病负担性别差异[19-20]。
与以往开展的IHD疾病负担研究相比[15-16, 20-21],本研究首次采用GBD2017数据估计中国人群IHD归因于环境、行为、代谢3大类24种危险因素的变化趋势。本研究发现吸烟、高盐饮食、坚果摄入不足等不合理膳食习惯为主的可控的行为危险因素是影响IHD疾病负担的最主要原因,这与WHO提出的慢性病关键危险因素一致[22]。1990-2017年,归因于加工肉摄入过多、含糖饮料摄入过多等饮食因素的疾病负担明显上升。经济发展水平的提高使中国居民的饮食结构从以植物性食物为主的东方膳食模式逐渐转为高胆固醇、高脂肪的动物性食物为主的西方膳食模式,这种转变加重了脂类的代谢负担,以致血管内血脂沉积,进而增加了心血管病的患病风险[23]。2007-2017年,高血压始终为我国人群IHD DALYs和PAF最高的危险因素,推测与中国居民高血压、高胆固醇血症、糖尿病、超重和肥胖症等慢性疾病流行率的增加有关[6, 24-25]。我国在2012-2015年开展的国家调查表明[26],18~24岁中国居民高血压的知晓率、治疗率、控制率仅为5.70%、3.40%、0.60%,预计未来高血压将继续成为我国IHD的首要危险因素[27-28]。因此分析高血压低知晓率、治疗率、控制率的原因并及时采取针对性措施将成为今后降低IHD疾病负担的重要研究领域[6]。
本研究表明,≥70岁人群IHD的YLLs增长得到了有效控制,但其YLDs上升幅度加快。2007年我国《全民健康生活方式行动倡议书》的出台鼓励全民健康生活方式,加强疾病一级预防[29];我国关于慢性病相关政策的制定以新医改为节点,2009年《中共中央国务院关于深化医药卫生体制改革的意见》的出台进一步加强了我国政府对慢性病的政策落实[22],此外,近年来医疗服务水平的改善和心脏康复的推广显著降低了IHD患者的死亡率[20]。而YLDs的上升可能与我国疾病诊断技术的发展提高了IHD的检出率[21]、人口预期寿命延长[4]、居民生活方式的改变密切相关[21]。本研究结果提示基层卫生服务机构应重点加强对中老年男性群体的健康宣教活动,提升其对IHD三级预防知识的认知水平,降低疾病危害。
本研究基于GBD2017数据对1990-2017年中国IHD疾病负担及其危险因素的变化趋势进行探讨,其结果可为今后制定相关政策提供依据。但本研究仅在国家层面分析IHD的疾病负担和危险因素变化,尚未深入至省、地区和县级层面人群的疾病负担估计和城乡间的比较,提示未来应进一步加强我国地方层面的疾病负担研究[30-31]。虽然GBD2017在GBD2016的基础上进行了数据和模型的更新[1, 3-4, 8],但GBD关于YLD的估计中,残疾权重来自全球多个国家数据统计结果,因此对中国疾病的估计会存在不确定性[3]。在收集不同年代数据时,不同年代疾病诊断标准的不一致可能会对结果产生影响,这也是GBD中难以避免的局限性。此外,对疾病负担的全面评价还应包括经济、家庭、社会等层面的负担,因此今后将增加多维度的分析以提高结果的准确性[32]。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1736-1788. DOI:10.1016/S0140-6736(18)32203-7 |
| [2] |
宋昕. WHO公布全球十大死亡原因[J]. 中华灾害救援医学, 2018, 6(11): 661. Song X. The top 10 causes of global death announced by WHO[J]. Chin J Dis Med, 2018, 6(11): 661. |
| [3] |
James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1789-1858. DOI:10.1016/S0140-6736(18)32279-7 |
| [4] |
Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1859-1922. DOI:10.1016/S0140-6736(18)32335-3 |
| [5] |
高晓琪, 何君, 邓颖, 等. 2015年四川省缺血性心脏病死亡状况分析[J]. 职业卫生与病伤, 2017, 32(3): 132-135. Gao XQ, He J, Deng Y, et al. Mortality of ischemic heart disease in Sichuan Province[J]. J Occ Health and Damage, 2017, 32(3): 132-135. |
| [6] |
Zhao D, Liu J, Wang M, et al. Epidemiology of cardiovascular disease in China:current features and implications[J]. Nat Rev Cardiol, 2019, 16(4): 203-212. DOI:10.1038/s41569-018-0119-4 |
| [7] |
宇传华, 崔芳芳. 全球疾病负担研究及其对我国的启示[J]. 公共卫生与预防医学, 2014, 25(2): 1-5. Yu CH, Cui FF. The global burden of disease study and the enlightenment to China[J]. Public Health Prev Med, 2014, 25(2): 1-5. |
| [8] |
Stanaway JD, Afshin A, Gakidou E, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1923-1994. DOI:10.1016/S0140-6736(18)32225-6 |
| [9] |
Institute for Health Metrics and Evaluation. Global Health Data Exchange[EB/OL]. http://ghdx.healthdata.org/geography/china.
|
| [10] |
陶庄, 杨功焕. 反事实和归因疾病负担研究[J]. 中华流行病学杂志, 2010, 31(4): 466-468. Tao Z, Yang GH. Counterfactual and burden of disease attributable to risk factors[J]. Chin J Epidemiol, 2010, 31(4): 466-468. DOI:10.3760/cma.j.issn.0254-6450.2010.04.025 |
| [11] |
周脉耕, 梁晓峰. 降低疾病负担, 促进全民健康[J]. 中国循环杂志, 2018, 33(12): 1145-1146. Zhou MG, Liang XF. Decrease the disease burden and promote the national health[J]. Chin Circ J, 2018, 33(12): 1145-1146. DOI:10.3969/j.issn.1000-3614.2018.12.002 |
| [12] |
Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990-2010:findings from the Global Burden of Disease Study 2010[J]. Lancet, 2013, 381(9882): 1987-2015. DOI:10.1016/S0140-6736(13)61097-1 |
| [13] |
王秀英.云南省通海县农村居民主要心血管疾病的疾病负担研究[D].昆明医科大学, 2013. Wang XY. Study on burden of major cardiovascular disease in Tonghai county of Yunnan province[D]. Kunming Medical University, 2013. |
| [14] |
刘明波, 刘韫宁, 王文, 等. 2004-2011年中国人群心血管病死亡的性别差异分析[J]. 中国慢性病预防与控制, 2014, 22(3): 267-269. Liu MB, Liu YN, Wang W, et al. Gender differences in cardiovascular disease mortality in China from 2004 to 2011[J]. Chin J Pre Contr Chron Dis, 2014, 22(3): 267-269. |
| [15] |
张干深, 宇传华, 罗丽莎, 等. 1990-2015年中国缺血性心脏病疾病负担趋势分析[J]. 中华预防医学杂志, 2017, 51(10): 915. Zhang GS, Yu CH, Luo LS, et al. Trend analysis of the burden of ischemic heart disease in China, 1990 to 2015[J]. Chin J Pre Med, 2017, 51(10): 915. DOI:10.3760/cma.j.issn.0253-9624.2017.10.009 |
| [16] |
刘明法, 周脉耕, 刘世炜, 等. 1990与2015年天津市心脑血管病疾病负担分析[J]. 中国慢性病预防与控制, 2018, 26(6): 421-425. Liu MF, Zhou MG, Liu SW, et al. The analysis on the burden of cardiovascular diseases in 1990 and 2015 of Tianjin[J]. Chin J Pre Contr Chron Dis, 2018, 26(6): 421-425. |
| [17] |
罗丽莎, 张干深, 宇传华, 等. 1990年与2015年中国归因于水果摄入不足的疾病负担分析[J]. 中国卫生统计, 2018, 35(2): 168-171, 176. Luo LS, Zhang GS, Yu CH, et al. Analysis of burden of disease attributable to diet low in fruits in 1990 and 2015 in China[J]. Chin J Health Stat, 2018, 35(2): 168-171, 176. |
| [18] |
刘明波, 王文, 周脉耕. 2004-2011年中国35岁以上人群缺血性心脏病死亡趋势与特征分析[J]. 中华预防医学杂志, 2014, 48(6): 502-506. Liu MB, Wang W, Zhou MG. Analysis of trends and characteristics of mortality of ischemic heart disease over the age of 35 years old in China, 2004-2011[J]. Chin J Pre Med, 2014, 48(6): 502-506. DOI:10.3760/cma.j.issn.0253-9624.2014.06.015 |
| [19] |
李建华.青岛市城阳区居民死因及疾病负担性别差异研究[D].山东大学, 2014. Li JH. Study on gender difference in the causes of death and disease burden of the residents in Chengyang district, Qingdao city[D]. Shandong University, 2014. |
| [20] |
Zhang G, Yu C, Zhou M, et al. Burden of ischemic heart disease and attributable risk factors in China from 1990 to 2015:findings from the global burden of disease 2015 study[J]. BMC Cardiovascular Disorders, 2018, 18(1): 18. DOI:10.1186/s12872-018-0761-0 |
| [21] |
Liu S, Li Y, Zeng X, et al. Burden of Cardiovascular Diseases in China, 1990-2016:Findings From the 2016 Global Burden of Disease Study[J]. JAMA Cardiol, 2019, 4: 342-352. DOI:10.1001/jamacardio.2019.0295 |
| [22] |
孙晓东, 吕筠, 李立明. 慢性病的主要危险因素流行水平及其预防策略的发展[J]. 中国慢性病预防与控制, 2008, 16(5): 538-540. Sun XD, Lv J, Li LM. Epidemiology of leading risk factors of non-communicable diseases and the development of prevention and control strategies[J]. Chin J Pre Contr Chron Dis, 2008, 16(5): 538-540. DOI:10.3969/j.issn.1004-6194.2008.05.041 |
| [23] |
徐明达, 毛彬. 饮食习惯对心脑血管疾病的影响[J]. 中国医药指南, 2011, 9(8): 194. Xu MD, Mao B. The impact of diet habits on cardiovascular disease[J]. Guide Chin Med, 2011, 9(8): 194. DOI:10.3969/j.issn.1671-8194.2011.08.143 |
| [24] |
Gordon-Larsen P, Wang H, Popkin BM. Overweight dynamics in Chinese children and adults[J]. Obesity Reviews, 2014, 15: 37-48. DOI:10.1111/obr.12121 |
| [25] |
杨静, 王卓群, 赵艳芳, 等. 2013年中国归因于高血清总胆固醇的疾病负担研究[J]. 中华预防医学杂志, 2016, 50(9): 764-768. Yang J, Wang ZQ, Zhao YF, et al. Burden of disease attributed to high total cholesterol in 2013 in China[J]. Chin J Pre Med, 2016, 50(9): 764-768. DOI:10.3760/cma.j.issn.0253-9624.2016.09.004 |
| [26] |
Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China:results from the China hypertension survey, 2012-2015[J]. Circulation, 2018, 137: 2344-2356. DOI:10.1161/CIRCULATIONAHA.117.032380 |
| [27] |
张雷, 崔红月, 刘爱萍, 等. 北京市城乡结合部居民心血管疾病危险因素及其与饮食习惯和体力活动的关系[J]. 中国慢性病预防与控制, 2009, 17(5): 447-450. Zhang L, Cui HY, Liu AP, et al. Prevalence of cardiovascular disease risk factors and their associations with dietary habits and physical activity in suburban area in Beijing[J]. Chin J Pre Contr Chron Dis, 2009, 17(5): 447-450. |
| [28] |
陈建功. 缺血性心脑血管疾病危险因素与预防[J]. 世界最新医学信息文摘, 2016, 16(57): 198-199. Chen JG. Prevention on risks factors of ischemic heart disease[J]. World Last Medicine Information, 2016, 16(57): 198-199. DOI:10.3969/j.issn.1673-9701.2009.12.024 |
| [29] |
张勇, 白雅敏, 邵月琴, 等. 新千年发展目标框架下的全球慢性病防控政策的回顾与建议[J]. 中国慢性病预防与控制, 2016, 24(8): 629-632. Zhang Y, Bai YM, Shao YQ, et al. Review and recommendation on prevention and control strategies of global non-communicable diseases under the in the new millennium development goals[J]. Chin J Pre Contr Chron Dis, 2016, 24(8): 629-632. DOI:10.16386/j.cjpccd.issn.1004-6194.2016.08.021 |
| [30] |
Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990-2013:A systematic subnational analysis for the Global Burden of Disease Study 2013[J]. Lancet, 2015, 387(10015): 251-272. DOI:10.1016/S0140-673(15)00551-6 |
| [31] |
Jiang G, Wang D, Li W, et al. Coronary heart disease mortality in China:age, gender, and urban-rural gaps during epidemiological transition[J]. Revista Panamericana de Salud Pública, 2012, 31(4): 317-324. DOI:10.1590/S1020-49892012000400008 |
| [32] |
王富珍, 齐亚莉, 李辉. 疾病负担研究的方法学进展——疾病负担综合评价[J]. 中华疾病控制杂志, 2003, 7(6): 537-539. Wang FZ, Qi YL, Li H. The methodological development of disease burden's research comprehensive evaluation of disease burden[J]. Chin J Dis Control Pre, 2003, 7(6): 537-539. DOI:10.3969/j.issn.1674-3679.2003.06.018 |