 2020, Vol. 41
2020, Vol. 41文章信息
- 谢莉, 肖琳, 旷聃, 姜垣, 杨焱.
- Xie Li, Xiao Lin, Kuang Dan, Jiang Yuan, Yang Yan
- 2015-2018年央补项目戒烟门诊患者首诊后1个月随访时戒烟率影响因素分析
- Influencing factors on smoking cessation among outpatients from the National Central Subsidy Smoking Cessation Clinic Project, in 2015-2018
- 中华流行病学杂志, 2020, 41(6): 890-895
- Chinese Journal of Epidemiology, 2020, 41(6): 890-895
- http://dx.doi.org/10.3760/cma.j.cn112338-20191104-00780
-
文章历史
收稿日期: 2019-11-04




2. 成都市疾病预防控制中心职业病防治科 610041
2. Occupational Disease Prevention Office, Chengdu Center for Disease Control and Prevention, Chengdu 610041, China
烟草使用是最重要的导致疾病和死亡的可预防因素。2018年中国成年人吸烟率为26.6%,其中男性为50.5%,女性为2.1%,烟民数量达3.06亿[1]。严峻的烟草流行形势给中国社会带来了严重的疾病负担。2000年中国烟草归因死亡达到100万人[2],2013年达159万[3]。最新研究结果显示,2017年中国烟草归因死亡达到250万[4]。如对吸烟流行状况不加以控制,到2050年中国每年因烟草导致的死亡人数将突破300万[2]。
烟草依赖是一种慢性病,心理行为疗法加药物治疗相结合是目前治疗烟草依赖最有效的方法。戒烟门诊能有效实施两种疗法,使戒烟成功率成倍增加[5]。最新监测数据显示,中国有16.1%的现在吸烟者打算在未来12个月内戒烟[1],意味着有近5 000万吸烟者有戒烟需求。为满足我国吸烟者戒烟的需求,中央补助地方健康素养促进项目自2014年以来要求全国31个省(自治区,直辖市)和新疆生产建设兵团每年在省内选择不少于3家医院开设戒烟门诊,并要求设立的戒烟门诊具备专门诊室、诊疗设备和药品等,配备专门的戒烟服务提供者。控烟办对戒烟门诊医务人员开展戒烟技能培训,并制定统一问卷收集戒烟者信息。医务人员对前往戒烟门诊寻求帮助的吸烟者进行行为心理干预或药物治疗。经过4年多的项目实施,共支持了全国586家戒烟门诊创建。本研究旨在评估项目实施的效果,探索吸烟者戒烟成功的影响因素,用以指导戒烟服务的提供和戒烟门诊工作的开展。
对象与方法1.研究对象:2015-2018年全国前往中央补助地方健康素养促进项目的戒烟门诊中寻求戒烟帮助的吸烟者。
2.调查方法:首诊由经过项目培训的医务人员,对吸烟者进行面对面访谈,填写统一的调查问卷,问卷内容包括年龄、文化程度、职业等一般人口学特征及吸烟频率、吸烟量、吸烟年限、晨起后第一支烟、既往戒烟史、戒烟意愿等吸烟相关问题。随后,医务人员对吸烟者进行面对面心理行为干预。干预内容主要为WHO推荐的“5A”和“5R”戒烟干预技巧[6]。已配备相应戒烟药物的医院,干预后为患者开具相应药物。项目医院配备的戒烟药物主要包括酒石酸伐尼克兰、盐酸安非他酮、中药等。
完成首诊后,由经过培训的医务人员在首诊1个月后开展随访干预。随访方式包括电话和面访,询问患者是否戒烟、戒断症状、吸烟量的变化和戒烟失败原因等信息,并解答疑问,提供心理支持和帮助。电话随访如果不同时段至少拨打5次仍不能联系到,或者约定面访但未前来的视为失访。失访者视为仍在吸烟。
1个月随访7 d时点戒烟率定义为1个月随访时前溯≥7 d患者自我报告未吸烟。减烟率定义为1个月随访时患者自我报告吸烟量与首诊吸烟量之差除以首诊吸烟量。
3.统计学分析:采用EpiData软件建立数据库,录入数据;统计分析采用SPSS 19.0软件,计量资料用x±s描述,计数资料用百分比(%)表示,多因素分析采用非条件logistic回归分析,P<0.05为差异有统计学意义。
结果1.一般情况:共收到2015-2018年除西藏自治区外的30个省(自治区,直辖市)和新疆生产建设兵团的35 372人次首诊患者数据,共有273家医院对其中的27 937例患者开展了随访,随访开展率为78.9%,随访方式主要为电话随访(81.5%)。本次分析剔除未做随访的所有病例,视失访者为仍在吸烟。
2.首诊情况:研究对象以男性(96.1%)为主,年龄(48.0±14.7)岁。从事职业以企业/商业/服务业人员(24.4%)和务农(20.7%)者居多、文化程度以初中(25.1%)和高中(21.3%)为主。烟龄(22.3±13.5)年。89.2%的研究对象首诊时自报健康状况良好,就诊戒烟门诊的途径主要为本院医生告知(54.5%)和医院内的宣传(25.6%)。56.3%的研究对象有过失败戒烟史。大部分研究对象(90.4%)准备在就诊后30 d内或就诊时已进入戒烟状态。由于戒烟药物尚未进入我国医疗保险体系,仅部分医院配备戒烟药物,首诊后医务人员未对23 661人(84.7%)开药。
前来戒烟的原因主要为关注自己和家人的健康,但不同年龄组就诊原因有差异,随着年龄的增大,由于自身患病前来戒烟的比例越来越大,从<40岁组的16.6%上升到40~59岁组的35.7%,≥60岁组该比例达64.4%。<40岁组患者更易受周围环境影响而戒烟。
3.随访情况:1个月随访7 d时点戒烟率为34.1%,1个月随访未戒烟者减烟率中位数为50%(P25~P75:25%~80%),其中11 089人(71.8%)的减烟率≥25%。自报对戒烟帮助最大的因素:自己决心(51.5%)、医生的帮助(20.1%)、家人的支持(9.6%)、药物支持(4.6%)等。
与首诊时相比,1个月随访时自报身体状况更差。其中自报身体好的比例由首诊的89.2%下降至51.1%,自报一般的比例从10.8%上升到37.2%,首诊时无自报身体差,但随访时有3.5%的患者自报身体状况差。随访时17.1%的研究对象自报体重上升。见图 1。

|
| 图 1 首诊与随访时患者自报身体状况对比(%) |
4.戒烟成功的影响因素:
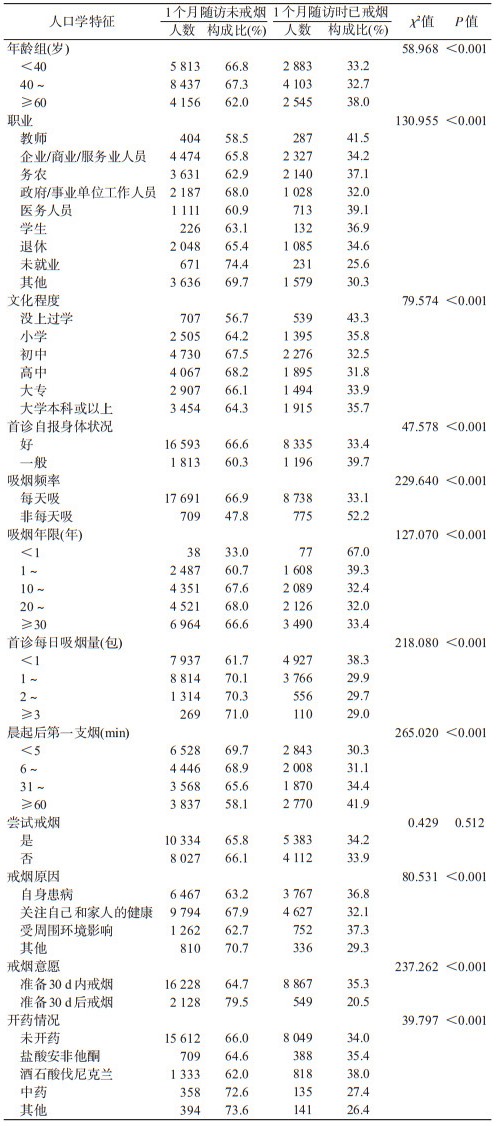
(1)单因素分析:单因素分析发现,不同年龄、职业、文化程度、首诊自报的身体状况、吸烟频率、吸烟年限、吸烟量、晨起第一支烟、戒烟意愿、首诊开药情况下戒烟成功率均差异有统计学意义(P<0.05),是否有过失败戒烟史的戒烟成功率差异无统计学意义(P>0.05);年龄≥60岁、职业为教师、医务人员或务农、文化程度高或未上过学、首诊自报健康状况较差、非每天吸烟者、每日吸烟量越小、吸烟年限越低、晨起后第一支烟越不急迫、戒烟原因为自身患病或受周围环境影响,以及使用酒石酸伐尼克兰或盐酸安非他酮药物的患者戒烟率更高。见表 1。
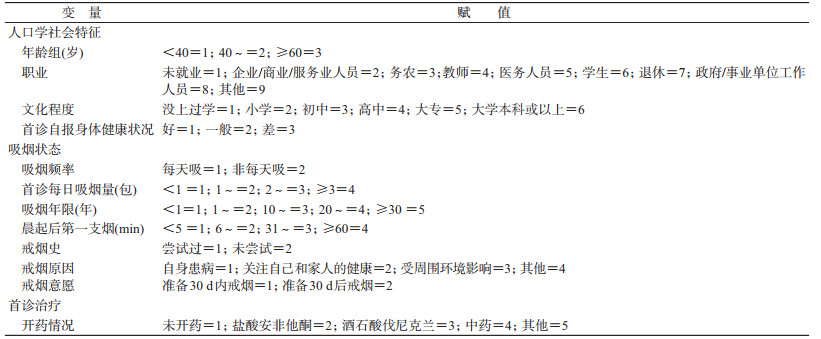
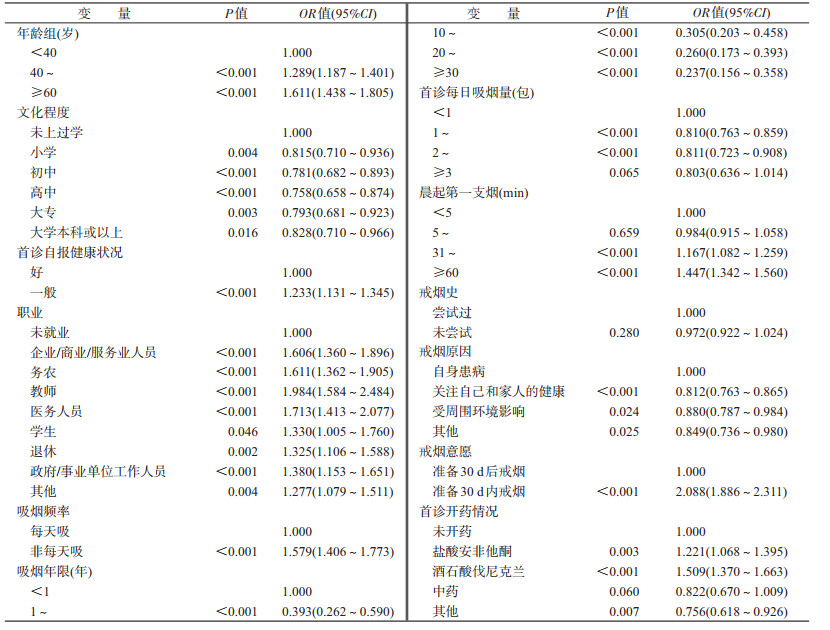
(2)多因素logistic回归分析:将1个月随访时是否戒烟作为因变量,表 2中因素作为自变量,进行多元logistic回归模型,按α=0.05水平筛选戒烟的影响因素。分析结果表明,年龄越大越可能戒烟,≥60岁组人群戒烟可能性最大;自身患病、首诊非每天吸烟、准备在30 d内戒烟、使用酒石酸伐尼克兰和盐酸安非他酮的患者,戒烟成功的可能性更大;未就业者相对于就业者更不利于戒烟;每日吸烟量越大、吸烟年限越长、晨起后第一支烟越急迫的患者,戒烟的可能性越小;是否有戒烟史对戒烟可能性没有影响。见表 3。
5.戒烟失败的原因:1个月随访时未戒烟者自报戒烟的阻碍因素:烟瘾发作(56.0%)、身边有其他吸烟者(20.0%)、感到有压力(10.8%)、喝酒或喝茶时(4.4%)、遇到悲伤或挫折(3.5%)等。
讨论本研究1个月随访7 d时点戒烟率为34.1%,高于2008年美国卫生与人口服务部的Meta分析结果,2次咨询加药物治疗的戒烟率为28.0%(23.0%~33.6%)[7]。我国大部分戒烟门诊工作刚起步,宣传不足,本研究中知道戒烟门诊的途径主要为患者前往项目医院就医时本院医生告知(54.5%)和医院内的宣传(25.6%),提示本身可能已患病,而且大部分研究对象(90.4%)具有近期戒烟的意愿,因此1个月随访7 d时点戒烟率较高。同时,未戒烟者中的减烟效果较好,同样提示项目医院戒烟门诊的心理行为干预加药物治疗有效。
分析患者戒烟的影响因素发现:①高年龄段、自身患病者更可能戒烟,<60岁吸烟者更多因为关注自身和家人健康或受周围环境影响而戒烟。随着年龄的增加,因自身患病前来戒烟的比例增加,≥60岁吸烟者自身患病的比例远高于其他年龄组。尽管判断是否戒烟的随访时长不尽相同,但国内外研究结果均提示[8-9],患病会提高患者的戒烟意愿,戒烟成功率相应提高,与本研究结果一致。而<60岁患者的戒烟原因更倾向于关注自身和家人健康,以及受周围环境的影响。因此可从“为了自身和家人健康”作为健康宣教的切入点,提高吸烟者的戒烟尝试率。此外,周围环境对吸烟者的影响也值得关注。相对于未就业,就业者更利于戒烟,而从业者中教师和医务人员的戒烟率较高,可能与我国陆续发布的医疗机构和学校的相关控烟规定有一定关系[10-11]。研究还发现[8],处于严格的无烟环境限制中的吸烟者更能成功戒烟。随着《“健康中国2030”规划纲要》的出台[12],我国如果运用价格、税收等手段加强控烟效果,同时积极推进无烟环境建设,这些举措的落实势必促进戒烟需求的增长,对于我国的戒烟门诊将是一个机遇同时也是一个挑战。因此,加强我国戒烟服务提供的能力迫在眉睫。②使用被证实有效的药物能加大成功戒烟的可能性。WHO在《戒烟指南》中明确指出[13],提高戒烟的成功率并预防复吸的最佳方法是应用有效的戒烟方法,避免使用未被证实有效的治疗方法[14]。本研究显示酒石酸伐尼克兰和盐酸安非他酮均能提高戒烟的可能性,2种药物均为WHO推荐并被证实有效的药品。但项目医院有效戒烟药物的配备率和使用率很低,仅11.6%吸烟者使用了有效的戒烟药。在条件成熟时,政府可考虑将有效药物纳入医疗保险范畴。③首诊时每日吸烟量越大、吸烟年限越长、晨起后第一支烟越急迫,戒烟的可能性越小,相反非每天吸烟者戒烟的可能性更大。提示尼古丁依赖程度越高,越影响戒烟成功的可能性。同现有研究结果一致[15-21]。应加大对烟民的健康教育,越早采取戒烟行动,才越有可能戒断烟瘾。由于是否有戒烟失败史对戒烟可能性没有影响,应鼓励复吸者不要丧失信心,继续戒烟。
戒烟者戒烟障碍主要为烟瘾发作(56.0%)和身边有其他吸烟者(20.0%),提示吸烟者在戒烟过程中要面临烟瘾的挑战,以及身边环境的影响。同时,随访时自报身体健康状况较首诊时更差,可能是患者戒烟或减烟过程中面临戒断症状导致。国外研究也表明,强烈的吸烟欲望与复吸之间有非常大的关联[22-23]。因此戒烟门诊医生在戒烟过程帮助患者制定戒烟计划,克服戒断症状很重要。
综上所述,尽管患病会增加吸烟者的戒烟意愿,但由于患者尼古丁依赖程度越高,越影响戒烟干预的效果,应加大对吸烟者的宣传,越早戒烟越好。戒烟过程中,医务人员使用专业的干预方法帮助患者克服戒断症状,对于防止复吸很重要。使用酒石酸伐尼克兰和盐酸安非他酮能增加戒烟的可能性,应提高戒烟门诊有效药物的配备率。由于我国烟草流行形式严峻,吸烟者众多,科学地提供戒烟服务,并与其他控烟措施相结合,能使戒烟门诊在控制烟草流行中发挥越来越大的作用。
本研究存在不足。我国戒烟门诊工作刚刚起步,很多门诊工作开展尚不规范,随访开展率有待提高。随访失访率同样有待改善。由于央补项目仅要求一次随访,因此只能以1个随访时的7 d时点戒烟率作为患者是否戒烟的参考,缺乏更长时段随访资料判断的戒烟率。此外,本研究电话随访的自报戒烟情况,可能与实际情况存在一定偏差。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
中国疾病预防控制中心.一图读懂2018年中国成人烟草调查结果[EB/OL]. (2019-05-31)[2019-06-01]. https://www.sohu.com/a/317971366_100167044. Chinese Center for Disease Control and Prevention. A picture to read the results of China's Adult Tobacco Survey in 2018[EB/OL]. (2019-05-31)[2019-06-01]. https://www.sohu.com/a/317971366_100167044. |
| [2] |
Chen ZM, Peto R, Zhou MP, et al. Contrasting male and female trends in tobacco-attributed mortality in China:evidence from successive nationwide prospective cohort studies[J]. Lancet, 2015, 386(1002): 1447-1456. DOI:10.1016/S0140-6736(15)00340-2 |
| [3] |
刘韫宁, 刘江美, 刘世炜, 等. 2013年中国居民吸烟对归因死亡和期望寿命的影响[J]. 中华流行病学杂志, 2017, 38(8): 1005-1010. Liu YN, Liu JM, Liu SW, et al. Death and impact of life expectancy atrributable to smoking in China, 2013[J]. Chin J Epidemiol, 2017, 38(8): 1005-1010. DOI:10.3760/cma.j.issn.0254-6450.2017.08.002 |
| [4] |
Zhou MG, Wang HD, Zeng XY, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2019, 394(10204): 1145-1158. DOI:10.1016/S0140-6736(19)30427-1 |
| [5] |
WHO. WHO Report on the Global Tobacco Epidemic: offer help to quit tobacco use, 2019[R]. Geneva: World Health Organization, 2019.
|
| [6] |
WHO. Toolkit for delivering the 5A's and 5R's brief tobacco interventions in primary care[R]. Geneva: World Health Organization, 2014.
|
| [7] |
Michael CF, Carlos RJ, Timothy BB, et al. Clinical practice guideline treating tobacco use and dependence: 2008 update[J]. U.S. Department of Health and Human Services, 2008.
|
| [8] |
Fu H, Feng D, Tang SF, et al. Prevalence of tobacco smoking and determinants of success in quitting smoking among patients with chronic diseases:a cross-sectional study in rural western China[J]. Int J Environ Res Public Health, 2017, 14(2): 167. DOI:10.3390/ijerph14020167 |
| [9] |
Layoun N, Hallit S, Waked M, et al. Predictors of past quit attempts and duration of abstinence among cigarette smokers[J]. J Epidemiol Global Health, 2017, 7(3): 199-206. DOI:10.1016/j.jegh.2017.06.003 |
| [10] |
卫生部.关于2011年起全国医疗卫生系统全面禁烟的决定.卫妇社发[2009]48号[EB/OL]. (2019-05-22)[2019-06-22]. http://www.gov.cn/zwgk/2009-05/22/content_1321944.htm. Ministry of Health of the PRC. Decision on banning smoking completely in the medical and health system from 2011.[2009] No. 48[EB/OL]. (2019-05-22)[2019-06-22]. http://www.gov.cn/zwgk/2009-05/22/content_1321944.htm. |
| [11] |
教育部.教育部、卫生部关于进一步加强学校控烟工作意见.教体艺厅[2010]5号[EB/OL]. (2010-07-23)[2019-06-22]. http://www.gov.cn/gzdt/2010-07/13/content_1653147.htm. Ministry of Education. Opinions on further strengthening school tobacco control work.[2010]NO.5[EB/OL]. (2010-07-23)[2019-06-22]. http://www.gov.cn/gzdt/2010-07/13/content_1653147.htm. |
| [12] |
中国共产党中央委员会, 中华人民共和国国务院.中共中央国务院印发《"健康中国2030"规划纲要》[EB/OL]. (2016-10-25)[2019-06-22]. http://www.gov.cn/xinwen/2016-10/25/content_5124174.htm. The Central Committee and the State Council. The Central Committee of the CPC and the State Council Print and Issue the Outline of the "Healthy China 2030" Plan[EB/OL]. (2016-10-25)[2019-06-22]. http://www.gov.cn/xinwen/2016-10/25/content_5124174.htm. |
| [13] |
World Health Organization. A guide for tobacco users to quit[M]. Geneva: World Health Organization, 2014.
|
| [14] |
Bacha ZA, Layoun N, Khayat G, et al. Factors associated with smoking cessation success in Lebanon[J]. Pharm Pract, 2018, 16(1): 1111. DOI:10.18549/PharmPract.2018.01.1111 |
| [15] |
Siddiquea BN, Islam MA, Bam TS, et al. High quit rate among smokers with tuberculosis in a modified smoking cessation programme in Dhaka, Bangladesh[J]. Public Health Act, 2013, 3(3): 243-246. DOI:10.5588/pha.13.0051 |
| [16] |
Chiappetta V, García-Rodriguez O, Jin CJ, et al. Predictors of quit attempts and successful quit attempts among individuals with alcohol use disorders in a nationally representative sample[J]. Drug Alcohol Depend, 2014, 141: 138-144. DOI:10.1016/j.drugalcdep.2014.05.019 |
| [17] |
Berg CJ, Schauer GL, Buchanan TS, et al. Perceptions of addiction, attempts to quit, and successful quitting in nondaily and daily smokers[J]. Psychol Addict Behav, 2013, 27(4): 1059-1067. DOI:10.1037/a0033790 |
| [18] |
Huang WH, Hsu HY, Chang BCC, et al. Factors correlated with success rate of outpatient smoking cessation services in Taiwan[J]. Int J Environ Res Public Health, 2018, 15(6): 1218. DOI:10.3390/ijerph15061218 |
| [19] |
Lee JS, Kim Y, Kim WN, et al. Changes in smoking status among current male smokers and factors associated with smoking cessation success[J]. J Prev Med Public Health, 2006, 39(4): 339-345. |
| [20] |
Tsoh JY, Tong EK, Gildengorin G, et al. Individual and family factors associated with intention to quit among male Vietnamese American smokers:implications for intervention development[J]. Addict Behav, 2011, 36(4): 294-301. DOI:10.1016/j.addbeh.2010.11.009 |
| [21] |
Vangeli E, Stapleton J, Smit ES, et al. Predictors of attempts to stop smoking and their success in adult general population samples:a systematic review[J]. Addiction, 2011, 106(12): 2110-2121. DOI:10.1111/j.1360-0443.2011.03565.x |
| [22] |
Taniguchi C, Tanaka H, Saka H, et al. Cognitive, behavioural and psychosocial factors associated with successful and maintained quit smoking status among patients who received smoking cessation intervention with nurses' counselling[J]. J Adv Nurs, 2017, 73(7): 1681-1695. DOI:10.1111/jan.13258 |
| [23] |
Fillo J, Alfano CA, Paulus DJ, et al. Emotion dysregulation explains relations between sleep disturbance and smoking quit-related cognition and behavior[J]. Addict Behav, 2016, 57: 6-12. DOI:10.1016/j.addbeh.2016.01.013 |