 2020, Vol. 41
2020, Vol. 41文章信息
- 裴华莲, 王淑霞, 苏银霞, 孙勇, 刘静波, 符文慧, 田恬, 戴江红, 姚华.
- Pei Hualian, Wang Shuxia, Su Yinxia, Sun Yong, Liu Jingbo, Fu Wenhui, Tian Tian, Dai Jianghong, Yao Hua
- 乌鲁木齐市体检人群不同代谢综合征评分与其行为危险因素聚集关系分析
- Co-prevalence relationship analysis on different metabolic syndrome scores and behavioral risk factors in adults from Urumqi based
- 中华流行病学杂志, 2020, 41(4): 514-519
- Chinese Journal of Epidemiology, 2020, 41(4): 514-519
- http://dx.doi.org/10.3760/cma.j.cn112338-20190618-00446
-
文章历史
收稿日期: 2019-06-18




2. 新疆医科大学公共卫生学院, 乌鲁木齐 830011;
3. 新疆医科大学健康管理院, 乌鲁木齐 830000;
4. 冠新软件有限公司, 乌鲁木齐 830000
2. School of Public Health, Xinjiang Medical University, Urumqi 830011, China;
3. Hospital of Public Health, Xinjiang Medical University, Urumqi 830000, China;
4. Guanxin Software Company Limited, Urumqi 830000, China
MS是一组以肥胖、高血糖(糖尿病或糖调节受损)、高血压以及血脂异常(TG偏高、HDL-C偏低)等聚集发病、严重影响机体健康的临床症候群[1]。我国正在进入高速老龄化时期[2],由于经济增长及生活方式的巨大转变,与年龄相关的MS的发病率逐年升高,大量研究已经证明MS疾病的发病与吸烟、过量饮酒、食盐、油脂、肉类过多、活动不足等行为危险因素有关[3-6],而在我国新疆维吾尔自治区(新疆)多民族聚居地区,由于特殊的饮食生活习惯,行为危险因素流行与聚集对MS的影响不容忽视。自2016年以来新疆开展的全民健康体检工作,每年对新疆籍城乡居民进行免费体检一次,是一项造福当地各族群众的医疗惠民工程。本研究选取2017年新疆全民健康体检监测数据库乌鲁木齐体检数据,旨在探讨不同人群行为危险因素的流行聚集性对MS评分的影响,以为控制行为危险因素相关的慢性疾病的发生发展提供科学依据。
对象与方法1.研究对象:来自2017年新疆乌鲁木齐市参与全民健康体检人群,共597 829人。按照纳入标准:年龄30~90岁,且人口学特征及MS评分5项无缺失记录者,共选取175 927人。
2.研究方法:本研究数据通过对乌鲁木齐健康体检人群的人体测量、实验室检查以及问卷调查获得,人体测量指标包括身高、体重、腰围,血压等,实验室检查指标包括血脂、空腹血糖,问卷信息包括基本人口学信息、自我报告的吸烟、饮酒、饮食、身体活动等相关信息,血液样品采集、指标测量以及相关实验室检查均由专业人员完成。
3.分析指标及标准:MS评分项目依据JCDCG诊断标准[7-9]:①中心性肥胖:腰围≥90 cm(男性)、≥85 cm(女性);②TG≥1.70 mmol/L;③HDL-C<1.04 mmol/L;④SBP≥130或DBP≥85 mmHg(1 mmHg=0.133 kPa);⑤FPG≥6.1 mmol/L,每符合一项得分为1分,分值为0~5分,≥3分定义为MS。
行为风险因素界定:(1)吸烟:①现在吸烟者:累积吸烟量≥100支,且调查时仍存在吸烟行为者;②戒烟者:过去曾经吸烟,但调查时已不再吸烟者;③从不吸烟者:一生累积吸烟量<100支[10]。(2)饮酒:①过量饮酒:男性日均酒精摄入量≥41 g的饮酒行为者或女性日均酒精摄入量≥21 g的饮酒行为者;②偶尔饮酒:指饮酒但男性日均酒精摄入量≤41 g的饮酒行为者或女性日均酒精摄入量≤21 g的饮酒行为者[11]。(3)饮食:食盐、食油摄入因难以定量,故采用自我汇报的嗜盐/油作为标准。(4)身体活动:中等强度运动时间≤150 min/周为身体活动不足[12],本研究将具备上述4种危险因素的数量判为危险因素聚集个数,共分为4个等级(0、1、2、≥3个)。
4.统计学方法:所有数据应用SAS 9.4软件包完成变量的提取及异常值的纠正、剔除等数据清洗。在一列分析指标数据中与均值的偏差超过3倍标准差的值判定为异常值,再与原始问卷进行核对,予以纠正或剔除。应用SPSS 23.0软件进行数据处理,采用均数、标准差、率及构成比等进行统计学描述,组间各数据比较采用秩和检验、χ2及趋势性χ2检验,有序变量Kendall’s tau-b相关分析,采用有序结果的logistic回归分析各行为危险因素聚集对MS评分的影响,检验水准α=0.05。
结果1.研究对象入选过程:参与全民体检人数共597 829例,符合年龄纳入标准的476 333例,剔除了人口学特征缺失数据9 705例及代谢风险相关指标缺失数据290 701例,最终纳入175 927例。剔除数据与纳入分析数据进行基线比较显示,年龄、性别分布差异无统计学意义(P>0.05)。见图 1。

|
| 图 1 研究对象入选流程 |
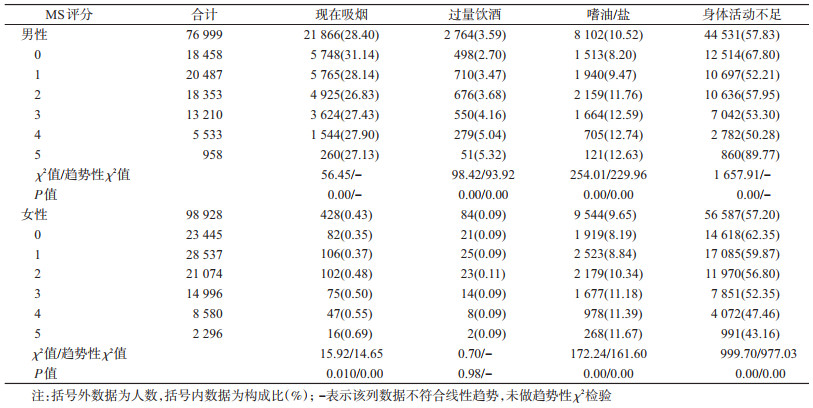
2.研究样本概况及MS评分:本研究纳入有效样本175 927人,年龄30~90岁,56.23%为女性,以城市人口居多,占70.00%,汉族占70.03%。行为危险因素中饮酒率、现在吸烟率、嗜油/盐率、身体活动不足率分别为10.98%、12.69%、9.99%、58.39%;危险因素得分0~5分别占23.82%、27.87%、22.41%、16.03%、8.02%、1.85%。MS组分异常(≥1分)的比例为76.28%,MS(≥3分)患病比例达25.80%。MS评分在不同年龄、民族、饮酒量、饮食的人群中的分布不同,差异均有统计学意义(P<0.05)。见表 1。

3. MS得分水平与各行为危险因素的关系:在男性人群中,行为危险因素流行率较高的为身体活动不足(57.83%)及现在吸烟率(28.40%)。男性MS评分随过量饮酒率、嗜油/盐率的升高而升高(P<0.01),评分5分者身体活动不足率最高。在女性群体中,流行率较高的行为危险因素为身体活动不足(57.20%)及嗜油/盐(9.65%)。女性评分随现在吸烟率、嗜油/盐率的升高而升高,而随身体活动不足率的降低而升高(P<0.01)。见表 2。
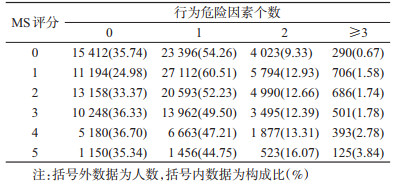
4.乌鲁木齐体检人群代谢风险得分水平与其行为危险因素的聚集关系分布:乌鲁木齐市男女性体检人群代谢风险得分均随着危险因素聚集数量的增加而升高,Kendall’s tau-b相关系数为0.004,差异有统计学意义(P=0.03)。见表 3。
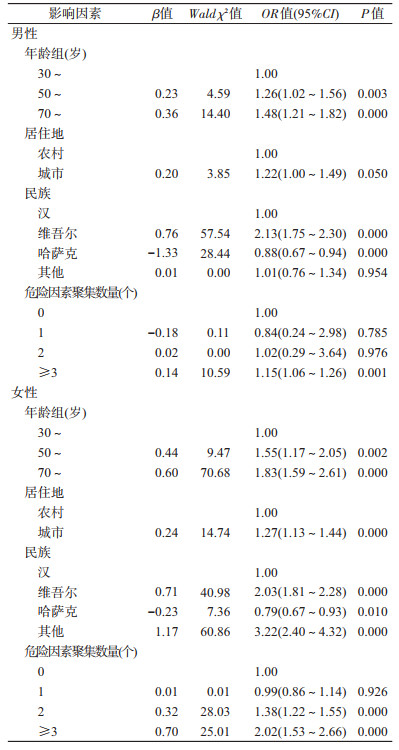
5.影响MS评分水平的多因素分析:采用有序结果的logistic分析方法,调整性别、年龄、民族、居住地等人口学因素影响后,男性危险因素≥3个组,其MS评分是不具有危险因素组的1.15(1.06~1.26)倍,女性危险因素2个和≥3个组,分别是不具有危险因素组的1.38(1.22~1.55)及2.02(1.53~2.66)倍。见表 4。
本研究发现,高龄、过量饮酒及嗜油/盐等是MS高评分的影响因素。增龄性慢性病患病率增高,饮酒、油脂等的过量摄入与MS的正相关性已得到证实[13-14]。维吾尔族居民高评分比例高于汉族,多因素分析结果类似,分析原因为新疆维吾尔族居民的饮食习惯中,素食偏少,油脂、面食、肉类摄入量更高[15],而哈萨克族饮食习惯与维吾尔族有共同之处,但哈萨克族高评分比例低于其他民族,与以往研究有所不同[16],可能与本研究中哈萨克族人群的样本量较少有关。
乌鲁木齐体检人群中MS组分异常(≥1分)或MS(≥3分)的比例高于全国平均水平[17],可能与研究人群的行为危险因素有关。本研究人群普遍存在不健康行为生活方式,其男性饮酒率、女性吸烟率及男女性嗜油/盐率均与MS评分呈正相关趋势,且MS评分较高者具有更多的行为危险因素聚集。多项研究支持食盐与油脂摄入与高血压、肥胖及高脂血症的显著关联性[18-19],因此,戒烟限酒、减少食盐及油脂摄入量能够有望降低MS的发生。然而女性身体活动不足率与MS评分成负相关,可能因为女性患者尤其是老年人更有时间保证,或因女性患者更关注自身身体状况而加强身体锻炼,从而造成身体活动不足率最高的反而评分最低,但具体原因还有待进一步研究证实。
本研究的男性现在吸烟率低于全国一般水平(67.9%)[20],可能与少数民族男性吸烟率低有关[21],但不排除自我报告吸烟率偏低的可能。本研究未观察到吸烟与MS评分的相关性,与Kim等[22]结果一致,但与闫慧敏等[4]和Slagter等[23]结果不一致。可能原因包括本研究人群的现在吸烟率较低,同时,吸烟也可能存在与其他行为因素(如饮酒)的交互效应,或吸烟对MS某些组分的影响高于对整体评分的影响[23-24],且不排除存在因患病而改变自身健康行为从而造成的误差。因此,吸烟与MS的关系仍有待进一步研究证实。
本研究在控制混杂因素后,发现危险因素聚集数量越多代谢风险得分越高,但MS疾病行为危险因素个数呈算术级数增长时,代谢风险评分升高的OR值并未呈现相应倍数增长。因此,MS疾病行为危险因素在个体聚集时产生的MS水平升高作用不是单个因素作用的叠加,而是不同行为方式以不同量效关系影响MS的不同组分并可能存在一种复杂的交互或综合作用[25]。但从整体趋势来看,危险因素聚集数量增多仍是MS评分增加的主要因素,因此,应针对多种不健康行为方式聚集的高危人群采取综合干预措施,以控制MS各个组分的异常,从而防止疾病的发生发展。
本研究存在局限性。全民体检由于实际条件所限,加之本研究涉及变量比较多,各变量均存在一定的缺失,主要体现在血脂和血糖数据的不完整性,导致用于分析的数据量明显降低,对研究结果的外推性产生影响。在今后大规模人群体检需要加强质量控制,严格过程监督,以保证体检数据的完整性和科学性。
综上所述,本研究利用乌鲁木齐市大样本健康体检人群分析了成年人群代谢风险得分水平与吸烟、过量饮酒、嗜油/盐、身体活动不足的行为危险因素存在相关性,且随个人危险因素聚集数量的增加而升高。该结论还需要前瞻性随访研究数据进一步验证。
利益冲突 所有作者均声明不存在利益冲突
志谢 感谢新疆医科大学健康管理院提供的乌鲁木齐市健康体检人群数据支持
| [1] |
中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2017年版)[J]. 中国实用内科杂志, 2018, 38(4): 292-344. Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition)[J]. Chin J Pract Int Med, 2018, 38(4): 292-344. DOI:10.19538/j.nk2018040108 |
| [2] |
付晓光, 汪早立, 杨胜慧. 人口老龄化对农村居民医疗费用影响研究[J]. 中国卫生统计, 2018, 35(2): 237-238. Fu XG, Wang ZL, Yang SH. Study on the influence of population aging on medical expenses of rural residents[J]. Chin J Health Stat, 2018, 35(2): 237-238. |
| [3] |
Luke JN, Brown A, Daniel M, et al. The metabolic syndrome and CVD outcomes for a central Australian cohort[J]. Diabet Res Clin Pract, 2013, 100(3): e70-73. DOI:10.1016/j.diabres.2013.03.020 |
| [4] |
闫慧敏, 张梅, 张笑, 等. 中国老年人代谢综合征流行特征及其影响因素研究[J]. 中华流行病学杂志, 2019, 40(3): 284-289. Yan HM, Zhang M, Zhang X, et al. Study of epidemiological characteristics of metabolic syndrome and influencing factors in elderly people in China[J]. Chin J Epidemiol, 2019, 40(3): 284-289. DOI:10.3760/cma.j.issn.0254-6450.2019.03.006 |
| [5] |
Zou TT, Zhou YJ, Zhou XD, et al. Mets risk score:a clear scoring model to predict a 3-year risk for metabolic syndrome[J]. Hormone Metabol Res, 2018, 50(9): 683-689. DOI:10.1055/a-0677-2720 |
| [6] |
Tzoulaki I, Elliott P, Kontis V, et al. Worldwide exposures to cardiovascular risk factors and associated health effects:Current knowledge and data gaps[J]. Circulation, 2016, 133(23): 2314-2333. DOI:10.1161/CIRCULATIONAHA.115.008718 |
| [7] |
中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南(2016年修订版)[J]. 中国循环杂志, 2016, 31(10): 937-953. Joint Committee for Developing Chinese Guidelines on Prevention and Treatment of Dyslipidemia in Adults. Chinese guidelines on prevention and treatment of dyslipidemia in adults (Revised Edition 2016)[J]. Chin Circulat J, 2016, 31(10): 937-953. DOI:10.3969/j.issn.1000-3614.2016.10.001 |
| [8] |
Yoon H, Gi MY, Cha JA, et al. The association between the metabolic syndrome and metabolic syndrome score and pulmonary function in non-smoking adults[J]. Diab Vasc Dis Res, 2018, 15(2): 131-138. DOI:10.1177/1479164117746022 |
| [9] |
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel Ⅲ). Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel Ⅲ) final report[J]. Circulation, 2002, 106(25): 3143-3421. DOI:10.1001/jama.285.19.2486 |
| [10] |
刘志强, 何斐, 蔡琳. 吸烟、被动吸烟与肺癌发病风险的病例对照研究[J]. 中华疾病控制杂志, 2015, 19(2): 145-149. Liu ZQ, He F, Cai L. A case-control study on smoking, passive smoking and the risk of lung cancer[J]. Chin J Dis Control Prev, 2015, 19(2): 145-149. DOI:10.16462/j.cnki.zhjbkz.2015.02.011 |
| [11] |
Desapriya EBR, Stockwell T, Doll SR, et al. International guide for monitoring alcohol consumption and related harm[R]. WHO/MSD/MSB/00.4. Geneva: World Health Organization, 2000. DOI: 10.13140/RG.2.2.29007.48808.
|
| [12] |
Kunene SH, Taukobong NP. Level of physical activity of health professionals in a district hospital in KwaZulu-Natal, South Africa[J]. S Afr J Physiother, 2015, 71(1): 234. DOI:10.4102/sajp.v71i1.234 |
| [13] |
何佳, 郭恒, 马儒林, 等. 新疆农村维吾尔族代谢综合征患病率及其肥胖组分适宜腰围切点的研究[J]. 中华内分泌代谢杂志, 2018, 34(3): 211-216. He J, Guo H, Ma RL, et al. Study on the prevalence rate and optimal waist circumference cut-off points of obesity for the components of metabolic syndrome in Uygur from Xinjiang[J]. Chin J Endocrinol Metabol, 2018, 34(3): 211-216. DOI:10.3760/cma.j.issn.1000-6699.2018.03.005 |
| [14] |
Zhang XE, Cheng B, Wang Q, et al. Association of gender-specific risk factors in metabolic and cardiovascular diseases:an NHANES-based cross-sectional study[J]. J Investig Med, 2017, 66(1): 22-31. DOI:10.1136/jim-2017-000434 |
| [15] |
何宇纳, 赵文华, 白国银, 等. 中国成年人肉类食物摄入与代谢综合征的相关性研究[J]. 中华流行病学杂志, 2018, 39(7): 892-897. He YN, Zhao WH, Bai GY, et al. Relationship between meat consumption and metabolic syndrome in adults in China[J]. Chin J Epidemiol, 2018, 39(7): 892-897. DOI:10.3760/cma.j.issn.0254-6450.2018.07.006 |
| [16] |
郭恒, 马儒林, 张景玉, 等. 新疆哈萨克族与汉族代谢综合征流行特点比较与分析[J]. 中华高血压杂志, 2011, 19(6): 538-543. Guo H, Ma RL, Zhang JY, et al. Comparative analysis of epidemic characteristic of metabolic syndrome of Kazakh and Hans in Xinjiang[J]. Chin J Hypertens, 2011, 19(6): 538-543. DOI:10.16439/j.cnki.1673-7245.2011.06.001 |
| [17] |
何宇纳, 赵文华, 赵丽云, 等. 中国2010-2012年成年人代谢综合征流行特征[J]. 中华流行病学杂志, 2017, 38(2): 212-215. He YN, Zhao WH, Zhao LY, et al. Prevalence of metabolic syndrome in Chinese adults in 2010-2012[J]. Chin J Epidemiol, 2017, 38(2): 212-215. DOI:10.3760/cma.j.issn.0254-6450.2017.02.015 |
| [18] |
Forman JP, Stampfer MJ, Curhan GC. Diet and lifestyle risk factors associated with incident hypertension in women[J]. JAMA, 2009, 302(4): 401-411. DOI:10.1001/jama.2009.1060 |
| [19] |
Gingras V, Leroux C, Fortin A, et al. Predictors of cardiovascular risk among patients with type 1 diabetes:A critical analysis of the metabolic syndrome and its components[J]. Diabetes Metab, 2017, 43(3): 217-222. DOI:10.1016/j.diabet.2016.10.007 |
| [20] |
申倩, 祝楠波, 余灿清, 等. 中国成年人吸烟与心血管疾病发病风险的关联及其性别差异分析[J]. 中华流行病学杂志, 2018, 39(1): 8-15. Shen Q, Zhu NB, Yu CQ, et al. Sex-specific associations between tobacco smoking and risk of cardiovascular diseases in Chinese adults[J]. Chin J Epidemiol, 2018, 39(1): 8-15. DOI:10.3760/cma.j.issn.0254-6450.2018.01.002 |
| [21] |
邢睿, 葛华, 刘继文. 乌鲁木齐市社区居民吸烟行为的调查分析[J]. 新疆医科大学学报, 2015, 38(1): 99-102. Xing R, Ge H, Liu JW. Investigation and analysis of smoking behavior among community residents in Urumqi[J]. J Xinjiang Med Univ, 2015, 38(1): 99-102. DOI:10.3969/j.issn.1009-5551.2015.01.027 |
| [22] |
Kim BJ, Han JM, Kang JG, et al. Relationship of cotinine-verified and self-reported smoking status with metabolic syndrome in 116, 094 Korean adults[J]. J Clin Lipidol, 2017, 11(3): 638-645. DOI:10.1016/j.jacl.2017.03.011 |
| [23] |
Slagter SN, van Vliet-Ostaptchouk JV, Vonk JM, et al. Associations between smoking, components of metabolic syndrome and lipoprotein particle size[J]. BMC Med, 2013, 11(1): 195. DOI:10.1186/1741-7015-11-195 |
| [24] |
Slagter SN, van Vliet-Ostaptchouk JV, Vonk JM, et al. Combined effects of smoking and alcohol on metabolic syndrome:the Life Lines cohort study[J]. PLoS One, 2014, 9(4): e96406. DOI:10.1371/journal.pone.0096406 |
| [25] |
de Boer MD, Filipp SL, Gurka MJ. Use of a metabolic syndrome severity Z score to track risk during treatment of prediabetes:an analysis of the diabetes prevention program[J]. Diabetes Care, 2018, 41(11): 2421-2430. DOI:10.2337/dc18-1079 |