 2020, Vol. 41
2020, Vol. 41文章信息
- 邵志宏, 石璟, 姚添, 冯丹, 董爽, 石珊, 冯永亮, Zhang Yawei, 王素萍.
- Shao Zhihong, Shi Jing, Yao Tian, Feng Dan, Dong Shuang, Shi Shan, Feng Yongliang, Zhang Yawei, Wang Suping
- 美沙酮维持治疗门诊患者特征和HBsAg阳性影响因素的贝叶斯网络模型分析
- Characteristics of methadone maintenance treatment clinic patients and influencing factors for HBsAg positivity based on Bayesian network model
- 中华流行病学杂志, 2020, 41(3): 331-336
- Chinese Journal of Epidemiology, 2020, 41(3): 331-336
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2020.03.010
-
文章历史
收稿日期: 2019-07-09




2. 南宁市红十字会医院美沙酮门诊 530012;
3. 耶鲁大学公共卫生学院环境健康科学系, 美国康涅狄格州纽黑文市 06520
2. Methadone Maintenance Treatment Clinic, Nanning Red Cross Hospital, Nanning 530012, China;
3. Division of Environment Health Sciences, School of Public Health, Yale University, New Haven, Connecticut 06520, USA
HBV感染是全球重大的公共卫生问题,尽管我国在HBV感染防控方面取得了巨大的成效[1-2],有数学模型估计2016年我国HBsAg流行率仍达6.10%[1],原因之一是高危人群的HBV感染率高且是向一般人群传播的纽带,吸毒人群是高危人群中HBV感染预防控制的关键人群,而美沙酮维持治疗(MMT)是控制吸毒人群海洛因或其他阿片类药物成瘾的一种常用的替代疗法[3]。我国自2003年开展MMT门诊以来,在减少毒品依赖、降低毒品危害等方面取得了一定成效,但MMT门诊患者HBV感染率仍较高[4],且该人群感染HBV后,极易出现HCV、HIV、梅毒等合并感染,严重影响该人群治疗效果及生命健康[5-7]。本研究选取广西壮族自治区(广西)3个MMT门诊患者进行特征分析,通过贝叶斯网络模型分析MMT门诊患者HBsAg阳性的影响因素及因素间复杂的网络关系[8],为做好该人群HBV感染的防控提供参考依据。
对象与方法1.研究对象:于2014年9-11月,将广西3所MMT门诊(南宁市红十字会医院MMT门诊、南宁市疾病预防控制中心MMT门诊和宾阳市MMT门诊)患者作为研究对象。纳入标准:①经过多次戒毒治疗仍不能戒断毒瘾的滥用阿片类物质成瘾者;②年龄≥ 20岁;③维持治疗机构所在县(市、区)居民或在本地居住>6个月且具有当地暂住证的外地户籍公民;④具有完全民事行为能力;⑤经过书面知情同意。排除标准:①由于聋哑或患有精神疾病不能完成问卷调查者;②不能提供书面知情同意书者[9]。本研究已获得山西医科大学伦理委员会批准。
2.研究方法:采用面对面问卷调查收集研究对象一般人口学特征、吸毒情况、治疗情况、性行为等;通过病历查阅收集HIV、HCV感染情况和近3个月的吗啡尿检结果等;采集研究对象5 ml非抗凝静脉血,分离血清,由培训合格的专业人员采用ELISA法对血清中的HBsAg、抗-HBs进行检测。
3.相关定义[9]:①脱失:MMT期间,要求受治者每天到MMT门诊服药1次,3个月内累计未服药或连续有15 d未服药,即为脱失。②吗啡尿检:MMT门诊受治者每月不定期吗啡尿检,治疗期间吸食毒品即为阳性。本研究采用最近3个月的吗啡尿检结果,阳性次数≥ 1次判断为吗啡尿检阳性。
4.统计学分析:采用EpiData 3.1软件进行数据双录入,采用SAS 9.4软件进行数据整理和分析,其中单因素分析采用χ2检验,多因素以MMT门诊患者是否HBsAg阳性为因变量(1=是,0=否),将单因素分析有意义的变量和文献中报道的相关变量纳入logistic回归模型。贝叶斯网络模型是基于概率的不确定性推理方法,通过构建有向无环图直观反映多因素间的潜在关系,利用条件概率分布来反映关系强度,能深入探讨因素之间复杂的网络关系,采用R 3.3.4软件中的“bnlearn”贝叶斯网络软件包进行HBsAg阳性影响因素及因素间关系的分析,通过Netica软件绘制贝叶斯网络及条件概率分布表。
结果1. MMT门诊患者特征:有效问卷1 031份,其中抗-HCV阳性者740例,由于抗-HCV阳性者较多,本次以MMT门诊患者和抗-HCV阳性者分别作为研究对象,描述其各因素的分布特征。
1 031例MMT门诊患者中男女性别比为4.18:1,年龄(42.20±7.60)岁;最近3个月静脉注射吸毒者164例,占15.91%(164/1 031);服用美沙酮的剂量大多为40~100 ml,占76.43%(788/1 031);HIV感染者156例,占15.13%(156/1 031)。
740例抗-HCV阳性者中,男女性比例为4:1,≥ 40岁者居多,占61.49%(455/740);最近3个月静脉注射吸毒者占20.41%(151/740);服用美沙酮的剂量大多在40~100 ml,占74.46%(551/740);HIV感染者135例,占18.24%(135/740)。见表 1。
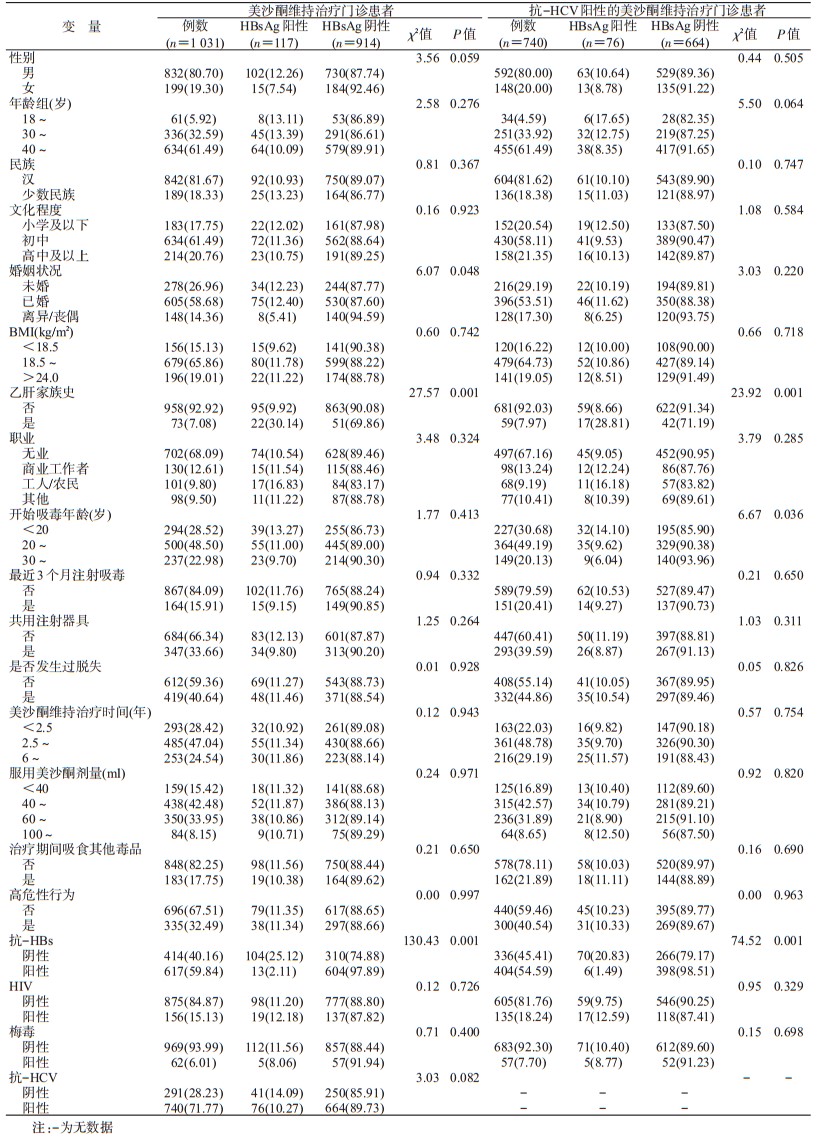
2. HBsAg阳性情况及相关因素:MMT门诊HBsAg阳性者117例,阳性率为11.35%(117/1 031),抗-HCV阳性者740例,占71.77%(740/1 031);将MMT门诊患者分为HBsAg阳性组和阴性组,单因素分析结果显示,婚姻状况、乙肝家族史和抗-HBs在两组间差异有统计学意义(χ2值分别为6.07、27.57和130.43;P < 0.05)。
在抗-HCV阳性者中HBsAg阳性者76例,阳性率为10.27%(76/740),分析HBsAg阳性的影响因素,结果显示,乙肝家族史、吸毒开始年龄和抗-HBs在两组之间的差异有统计学意义(χ2值分别为23.92、6.67和74.52;P < 0.05)。见表 1。
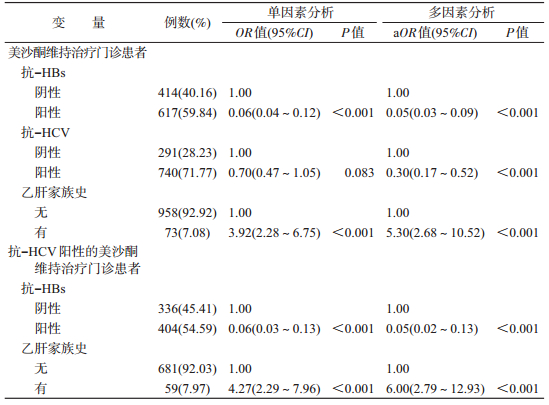
3. MMT门诊患者HBsAg阳性影响因素logistic回归分析:结果显示,控制性别、职业、婚姻状况、民族、治疗期间吸食其他毒品、吸毒方式、不安全性行为、梅毒、HIV感染、吗啡尿检和脱失后,抗-HBs阳性与阴性者相比,不易出现HBsAg阳性(OR=0.05,95%CI:0.03~0.09);抗-HCV阳性与阴性者相比,也不易出现HBsAg阳性(OR=0.30,95%CI:0.17~0.52);有乙肝家族史与无乙肝家族史者相比,出现HBsAg阳性的风险较大(OR=5.30,95%CI:2.68~10.52)。调整与上述相同的变量后,抗-HCV阳性者HBsAg阳性影响因素logistic回归分析结果显示,有乙肝家族史比无乙肝家族史者更容易出现HBsAg阳性(OR=6.00,95%CI:2.79~12.93);抗-HBs阳性与阴性者相比,不易出现HBsAg阳性(OR=0.05,95%CI:0.02~0.13)。见表 2。
4.基于贝叶斯网络模型的MMT门诊患者HBsAg阳性影响因素分析:进一步分析MMT门诊患者HBsAg阳性影响因素之间复杂的网络关系,从表 1与HBsAg阳性相关的变量中,选择文献中报道及专业上认为与HBsAg阳性相关的变量构建包含9个节点、10条有向边的贝叶斯网络模型,并获得各节点的条件概率。结果显示:乙肝家族史、抗-HBs与HBsAg阳性直接相关;最近3个月注射吸毒、治疗期间吸食其他毒品与抗-HCV直接相关,与HBsAg阳性间接相关。见图 1。

|
| 图 1 美沙酮维持治疗门诊患者HBsAg阳性影响因素贝叶斯网络模型 |
抗-HCV阳性者分析显示,乙肝家族史、抗-HBs和最近3个月注射吸毒与HBsAg阳性直接相关;治疗期间吸食其他毒品与最近3个月注射吸毒相关,与HBsAg阳性间接相关。
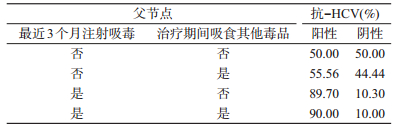
基于条件概率分布基础,以最近3个月注射吸毒和治疗期间吸食其他毒品为父节点,其与抗-HCV的条件概率分布表明:两者同时存在时,抗-HCV阳性的条件概率最高(90.00%),两者都不存在时,条件概率最低(50.00%),最近3个月非注射吸毒但治疗期间吸食其他毒品时抗-HCV阳性的条件概率为55.56%,低于最近3个月注射吸毒但治疗期间未吸食其他毒品(89.70%)。提示最近3个月注射吸毒和治疗期间吸食其他毒品均会导致抗-HCV阳性率升高。见表 3。
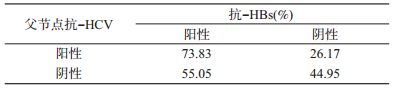
以抗-HCV为父节点时,其与抗-HBs水平的条件概率分布表明,抗-HCV阳性时,抗-HBs阳性的条件概率(73.83%)高于抗-HCV阴性(55.05%),提示抗-HCV阳性是抗-HBs阳性的保护因素。见表 4。
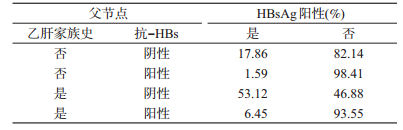
以乙肝家族史和抗-HBs为父节点,HBsAg阳性情况的条件概率分布显示,有乙肝家族史且抗-HBs阴性时,HBsAg阳性的条件概率最高(53.12%),无乙肝家族史且抗-HBs阳性时,条件概率最低(1.59%),有乙肝家族史且抗-HBs阳性时HBsAg阳性的条件概率(6.45%)低于无乙肝家族史且抗-HBs阴性时HBsAg阳性的条件概率(17.86%),提示乙肝家族史是HBsAg阳性的危险因素,抗-HBs阳性是HBsAg阳性的保护因素。见表 5。
本研究MMT门诊患者HBsAg阳性率11.35%,高于2013年调查显示的广西农村地区1~59岁一般人群的9.04%[10]。可能是由于研究现场广西与越南接壤,中越边境通道多,进出便利,使得地理位置特殊的广西成为毒品流通和泛滥的重要市场[11],吸毒问题较为严重,MMT门诊患者这类特殊人群存在易脱失、抗体阳性率低等自身特点及在参加治疗前及治疗过程中存在注射吸毒、共用注射器、高危性行为等,加之当地吸毒人群文化程度可能相对较低,健康意识薄弱,对传染病的认识不足,导致其成为HBsAg阳性率高的高危人群。
本研究logistic回归和贝叶斯网络模型结果都显示:①抗-HBs阳性是MMT门诊患者HBsAg阳性的保护因素,一方面抗-HBs可以特异性结合体内的HBsAg,启动机体的免疫应答,达到清除病毒的作用,从而有效降低HBsAg阳性率[12];另一方面,具有保护性抗体,说明其既往注射过乙肝疫苗,而注射疫苗也是一个传染病防控健康教育的过程,可有效提高个体自我保护意识[13]。②乙肝家族史是HBsAg阳性的危险因素,可能是由于HBV感染具有家族聚集性的特点[14],日常生活密切接触和母婴垂直传播[15],使其HBsAg阳性率较高。
有研究认为[16],在MMT门诊患者中HCV感染是HBsAg阳性的危险因素。与上述研究不同,本研究结果均显示,抗-HCV阳性是HBsAg阳性的保护因素。抗-HCV阳性,表明患者正在感染或既往感染过HCV[17],HCV感染经过特定的抗病毒治疗之后,多数可以治愈[18],但其抗-HCV在很长一段时间内仍能检测到。研究者在进入MMT门诊时会进行HCV的检测,一旦发现抗-HCV阳性或HCV RNA阳性,医生会建议其进行抗病毒治疗和接种乙肝疫苗[19],在一定程度上降低了其他肝炎病毒的感染;另外在治疗的过程中接受健康教育,增强了健康意识,降低了HBV感染的风险。本研究得出抗-HCV阳性是HBsAg阳性的保护因素,这一结果也为上述抗-HCV阳性者HBsAg阳性率(10.27%)低于MMT门诊患者HBsAg阳性率(11.35%)提供了数据支持。
贝叶斯网络模型结果显示注射吸毒和治疗期间吸食其他毒品与抗-HCV阳性直接相关,与HBsAg阳性间接相关。注射吸毒者由于存在共用注射器等高危行为,长期反复针刺增加了通过血液途径传播HCV的风险,这与国内外研究结果相一致[20-21]。另外,在MMT期间,一些患者吸食其他毒品,且静脉注射居多[22],发生共用针具、不安全性行为的风险较大,因而其抗-HCV阳性率较高。
本研究是横断面调查,主要关注MMT门诊患者HBsAg阳性的影响因素,但在HBV感染者中,抗-HBc和其他乙肝相关指标与HBV感染密切相关,也值得关注。因此,后期研究可对抗-HBc和其他乙肝相关指标的检测做进一步分析。
综上所述,广西3所MMT门诊患者HBsAg阳性率高于一般人群;抗-HBs、乙肝家族史、抗-HCV、最近3个月注射吸毒及治疗期间吸食其他毒品与MMT门诊患者HBsAg阳性相关,应对MMT门诊患者进行健康教育,提高该人群的健康意识,减少高危行为的发生,降低其HBV感染风险。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
The Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016:a modelling study[J]. Lancet Gastroenterol Hepatol, 2018, 3(6): 383-403. DOI:10.1016/S2468-1253(18)30056-6 |
| [2] |
Liang XF, Bi SL, Yang WZ, et al. Epidemiological serosurvey of hepatitis B in China-declining HBV prevalence due to hepatitis B vaccination[J]. Vaccine, 2009, 27(47): 6550-6557. DOI:10.1016/j.vaccine.2009.08.048 |
| [3] |
Shi J, Zhao LY, Epstein DH, et al. The effect of methadone maintenance on illicit opioid use, human immunodeficiency virus and hepatitis C virus infection, health status, employment, and criminal activity among heroin abusers during 6 months of treatment in China[J]. J Addict Med, 2007, 1(4): 186-190. DOI:10.1097/adm.0b013e318156cc19 |
| [4] |
Chen W, Xia YH, Hong Y, et al. Predictors of continued HIV-risk behaviors among drug users in methadone maintenance therapy program in China-A prospective study[J]. Harm Reduct J, 2013, 10(1): 23. DOI:10.1186/1477-7517-10-23 |
| [5] |
UNAIDS. Global report: UNAIDS report on the global AIDS epidemic 2010[R]. Geneva: UNAIDS, 2010: 553-556.
|
| [6] |
Han Y, Zeng AJ, Liao HY, et al. The efficacy and safety comparison between tenofovir and entecavir in treatment of chronic hepatitis B and HBV related cirrhosis:a systematic review and Meta-analysis[J]. Int Immunopharmacol, 2017, 42: 168-175. DOI:10.1016/j.intimp.2016.11.022 |
| [7] |
Thomas DL, Astemborski J, Rai RM, et al. The natural history of hepatitis C virus infection:host, viral, and environmental factors[J]. JAMA, 2000, 284(4): 450-456. DOI:10.1001/jama.284.4.450 |
| [8] |
García-Herrero S, Mariscal MA, Gutiérrez JM, et al. Using Bayesian networks to analyze occupational stress caused by work demands:preventing stress through social support[J]. Accid Anal Prev, 2013, 57: 114-123. DOI:10.1016/j.aap.2013.04.009 |
| [9] |
姚添, 冯丹, 潘明虎, 等. 美沙酮维持治疗门诊受治者艾滋病病毒与丙型肝炎病毒共感染相关因素及交互作用分析[J]. 中华流行病学杂志, 2018, 39(5): 631-635. Yao T, Feng D, Pan MH, et al. Related factors and interaction on HIV/HCV co-infection of patients access to methadone maintenance treatment[J]. Chin J Epidemiol, 2018, 39(5): 631-635. DOI:10.3760/cma.j.issn.0254-6450.2018.05.017 |
| [10] |
张维璐, 吉兆华, 付婷, 等. 中国2007-2016年59岁以下普通人群HBsAg阳性率的Meta分析[J]. 中华流行病学杂志, 2017, 38(9): 1278-1284. Zhang WL, Ji ZH, Fu T, et al. Meta analysis on HBsAg-positive rate among general populations aged 1-59 years, 2007-2016, China[J]. Chin J Epidemiol, 2017, 38(9): 1278-1284. DOI:10.3760/cma.j.issn.0254-6450.2017.09.027 |
| [11] |
陆贤杰, 覃云鹏, 梁峰, 等. 广西西部吸毒人员艾滋病病毒感染情况及有关危险因素调查分析[J]. 中国药物依赖性杂志, 2006, 15(6): 475-477. Lu XJ, Qin YP, Liang F, et al. Survey on HIV infection status in drug users and related factors in western Guangxi[J]. Chin J Drug Depend, 2006, 15(6): 475-477. DOI:10.3969/j.issn.1007-9718.2006.06.015 |
| [12] |
Guidotti LG, Rochford R, Chung J, et al. Viral clearance without destruction of infected cells during acute HBV infection[J]. Science, 1999, 284(5415): 825-829. DOI:10.1126/science.284.5415.825 |
| [13] |
朱大伟, Wangen KR, 王健, 等. 中国农村地区成人乙肝疫苗接种及影响因素[J]. 中国公共卫生, 2012, 28(10): 1291-1293. Zhu DW, Wangen KR, Wang J, et al. Influencing factors of vaccination of hepatitis B vaccine in rural adults in China[J]. Chin J Public Health, 2012, 28(10): 1291-1293. DOI:10.11847/zgggws2012-28-10-10 |
| [14] |
杨瑗, 金李, 王静, 等. 不良结局家族聚集性乙型肝炎病毒感染家系的分子流行病学[J]. 中华传染病杂志, 2016, 34(9): 540-544. Yang Y, Jin L, Wang J, et al. Study of molecular epidemiology in families with clusters of hepatitis B virus infection and unfavorable outcome[J]. Chin J Infect Dis, 2016, 34(9): 540-544. DOI:10.3760/cma.j.issn.1000-6680.2016.09.006 |
| [15] |
Zhu YY, Mao YZ, Wu WL, et al. Does hepatitis B virus prenatal transmission result in postnatal immunoprophylaxis failure?[J]. Clin Vaccine Immunol, 2010, 17(12): 1836-1841. DOI:10.1128/CVI.00168-10 |
| [16] |
邱望龙, 李福元, 唐洪彦, 等. 重叠HCV感染对HBV/C基因热点变异的影响[J]. 中华传染病杂志, 1997, 15(2): 65-67. Qiu WL, Li FY, Tang HY, et al. Influence of hepatitis C virus surperinfection upon core "hot" mutations of hepatitis B virus[J]. Chin J Infect Dis, 1997, 15(2): 65-67. DOI:10.3760/j.issn:1000-6680.1997.02.002 |
| [17] |
李宏志, 张婧, 杨柳. 定量检测丙型肝炎病毒核酸的临床意义[J]. 中国热带医学, 2006, 6(9): 1679, 1660. Li HZ, Zhang J, Yang L. The clinical significance of quantitative detection of HBV nuclear acid[J]. Chin Trop Med, 2006, 6(9): 1679, 1660. DOI:10.3969/j.issn.1009-9727.2006.09.082 |
| [18] |
姚光弼. 丙型病毒性肝炎治疗的决策和选择[J]. 中华传染病杂志, 2003, 21(6): 381-385. Yao GB. Decision and choice of treatment for hepatitis C virus[J]. Chin J Infect Dis, 2003, 21(6): 381-385. DOI:10.3760/j.issn:1000-6680.2003.06.001 |
| [19] |
饶慧瑛, 魏来. 慢性丙型肝炎直接抗病毒药物的研究进展和应用前景[J]. 传染病信息, 2012, 25(2): 83-86. Rao HY, Wei L. Recent progress and future prospects of direct-acting antiviral agents for chronic hepatitis C[J]. Infect Dis Inf, 2012, 25(2): 83-86. DOI:10.3969/j.issn.1007-8134.2012.02.006 |
| [20] |
Oyaro M, Wylie J, Chen CY, et al. Human immunodeficiency virus infection predictors and genetic diversity of hepatitis B virus and hepatitis C virus co-infections among drug users in three major Kenyan cities[J]. S Afr J HIV Med, 2018, 19(1): a737. DOI:10.4102/sajhivmed.v19i1.737 |
| [21] |
王敏, 廖峭, 许茹, 等. 广州地区吸食毒品人员丙型肝炎病毒感染的分子流行病学研究[J]. 中国病毒病杂志, 2017, 7(3): 201-206. Wang M, Liao Q, Xu R, et al. Molecular epidemiology of hepatitis C virus infections among intranasal drug users in Guangzhou, China[J]. Chin J Viral Dis, 2017, 7(3): 201-206. DOI:10.16505/j.2095-0136.2017.03.008 |
| [22] |
Launonen E, Wallace I, Kotovirta E, et al. Factors associated with non-adherence and misuse of opioid maintenance treatment medications and intoxicating drugs among Finnish maintenance treatment patients[J]. Drug Alcohol Depend, 2016, 162: 227-235. DOI:10.1016/j.drugalcdep.2016.03.017 |