 2019, Vol. 40
2019, Vol. 40文章信息
- 刘少博, 夏云婷, 王丽敏, 张梅, 赵振平, 徐婷玲, 张笑, 李纯, 黄正京, 李剑虹.
- Liu Shaobo, Xia Yunting, Wang Limin, Zhang Mei, Zhao Zhenping, Xu Tingling, Zhang Xiao, Li Chun, Huang Zhengjing, Li Jianhong.
- 2013年中国18岁及以上超重/肥胖人群体重测量行为分析
- Self-body weight measurement in overweight and obese adults in China, 2013
- 中华流行病学杂志, 2019, 40(11): 1386-1391
- Chinese Journal of Epidemiology, 2019, 40(11): 1386-1391
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.11.009
-
文章历史
收稿日期: 2019-03-07




2. 中国疾病预防控制中心农村改水技术指导中心检验室, 北京 102200;
3. 中国疾病预防控制中心中国现场流行病学培训项目, 北京 100050;
4. 中国疾病预防控制中心慢性非传染性疾病预防控制中心危险因素监测室, 北京 100050
2. Laboratory, National Center for Rural Water Supply Technical Guidance, Chinese Center for Disease Control and Prevention, Beijing 102200, China;
3. Chinese Field Epidemiology Training Program, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
4. Division of Non-communicable Disease Risk Factor Surveillance, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
超重和肥胖是糖尿病、心脑血管疾病和恶性肿瘤等主要慢性病独立且可预防的危险因素之一,是全球共同面临的重大公共卫生问题[1]。超重和肥胖不仅造成多种慢性病患病率快速上升,还加重了疾病负担[2]。研究证明,体重增加与能量摄入增加和(或)能量消耗减少有关[3]。每月或更频繁(每周、每天)地监测体重可及时、准确地了解体重变化情况,合理调整膳食摄入和身体活动情况,以达到控制体重的效果[4-6],这被认为是减重干预措施的重要组成部分[5]。因此,促进超重/肥胖人群自主测量体重行为,提高其体重知晓水平,是有效控制体重的重要前提。中国CDC慢性非传染性疾病预防控制中心于2013年开展了中国慢性病及其危险因素监测项目,本研究对该项目收集到的相关信息进行分析,探讨我国≥18岁超重/肥胖人群体重测量情况及影响因素,为提高超重/肥胖人群体重监测意识、促进自主体重控制行为提供依据。
对象与方法1.研究对象:2013年中国慢性病及其危险因素监测按照多阶段分层整群随机抽样方法在中国31个省份的302个监测点调查≥18岁常住居民177 099人[7]。去除抽样设计具有独立性的新疆生产建设兵团的4个监测点和1个数据质量较差的监测点后,最终纳入297个监测点数据进行分析,实际纳入调查176 534人。本次监测的总体设计、区域划分、抽样方法、研究对象的纳入标准及调查内容见文献[8]。本研究选取该调查中所有超重/肥胖者为研究对象,剔除关键信息缺失者288人,最终对87 670名调查对象进行分析。本研究通过中国CDC慢性非传染性疾病预防控制中心伦理审查委员会的审查(审批号:201307),所有调查对象均签署知情同意书。
2.调查内容:包括问卷调查、身体测量和实验室检测。问卷由中国CDC慢性非传染性疾病预防控制中心开发设计,调查由经过统一培训的调查员以面对面询问的方式收集调查对象的个人基本信息、体重测量信息、主要慢性病(高血压、糖尿病、血脂异常)患病情况等内容。身体测量包括身高、体重、腰围和血压。实验室检测包括FPG、服糖后2 h血糖(OGTT-2h)和血脂(TC、LDL-C、HDL-C和TG)[8]。质量控制方法见文献[9-10]。
3.分析指标及标准:①体重测量时间(分类型变量)通过面对面询问调查对象“您最近一次测量体重的时间”获得。体重测量时间分布情况中将该变量分为1周内、1个月内、1年内、1年以前和从未测量过5组。多因素回归分析中,将在1年内或1年以前测量过体重的定义为测量过体重,从未测量过体重和记不清的定义为未测量过体重。②超重和肥胖[11]:以24.0 kg/m2≤BMI<28.0 kg/m2为超重,BMI≥28.0 kg/m2为肥胖,BMI=体重(kg)/身高(m)2。③中心性肥胖:腰围(WC)男性≥85 cm,女性≥80 cm。④糖尿病:FPG≥7.0 mmol/L和(或)OGTT-2h≥11.1 mmol/L,或已被乡镇(社区)级或以上医院确诊为糖尿病。⑤血脂异常:TG≥2.26 mmol/L,或TC≥6.22 mmol/L,或HDL-C<1.04 mmol/L,或LDL-C≥4.14 mmol/L,或已被乡镇(社区)级或以上医院诊断为血脂异常。⑥高血压:SBP≥140 mmHg和(或)DBP≥90 mmHg(1 mmHg=0.133 kPa),或已被乡镇(社区)级或以上医院确诊为高血压且近2周服药[8]。
4.统计学分析:采用SAS 9.4软件完成所有数据的清理、描述和分析,所有调查结果(率)均经过复杂加权进行调整,抽样权重的具体计算参见文献[7]。不同特征成年人的超重/肥胖者体重测量加权构成比和加权率比较采用基于复杂抽样设计矫正的Rao-Scott χ2检验来完成。趋势性检验采用基于复杂抽样logistic回归系数的假设检验。采用Survey logistic回归模型对超重/肥胖者体重测量情况进行多因素分析[12],以双侧检验P<0.05为差异有统计学意义。
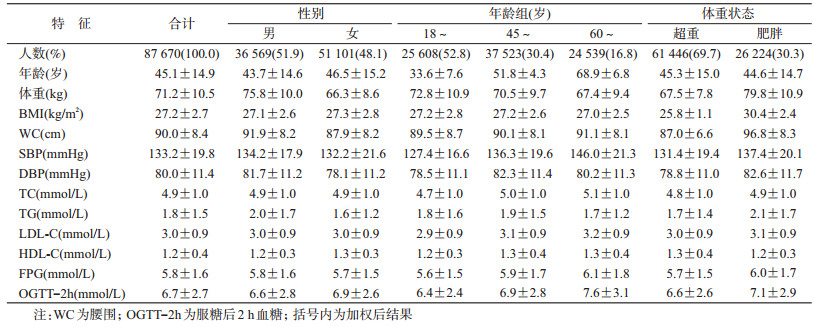
结果1.一般情况:超重/肥胖成年人有效样本共87 670例,男性36 569人(51.9%),女性51 101人(48.1%),年龄(45.1±14.9)岁;超重者61 446人(69.7%),肥胖者26 224人(30.3%)。样本人群体重、BMI、WC、SBP、DBP、TC、TG、LDL-C、HDL-C、FPG和OGTT-2h水平分别为(27.2±2.7)kg/m2、(90.0±8.4)cm、(133.2±19.8)mmHg、(80.0±11.4)mmHg、(4.9±1.0)mmol/L、(1.8±1.5)mmol/L、(3.0±0.9)mmol/L、(1.2±0.4)mmol/L、(5.8±1.6)mmol/L和(6.7±2.7)mmol/L。见表 1。
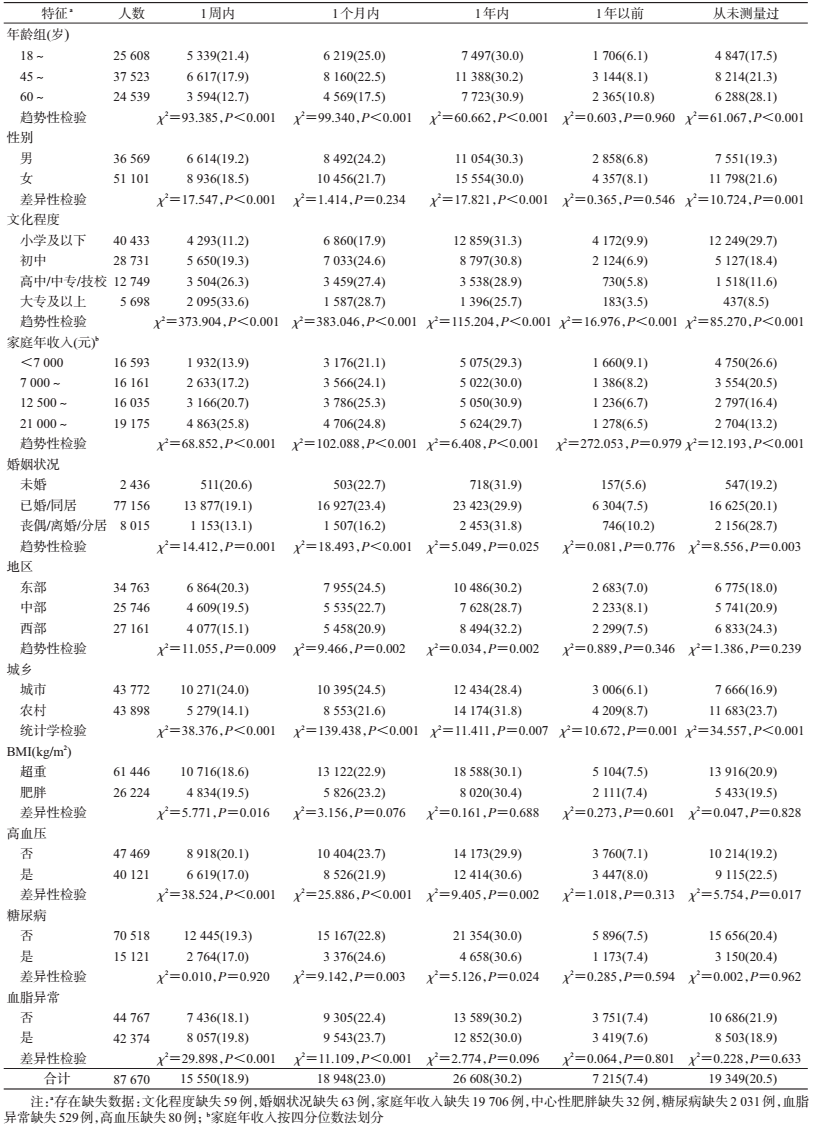
2.体重测量时间分布情况:2013年我国超重/肥胖成年人最近1次测量体重的时间在1周内、1个月内、1年内、1年以前的比例分别为18.9%、23.0%、30.2%、7.4%。其中,1周内、1个月内的体重测量率均为男性高于女性,城市高于农村,东部高于中部和西部地区,肥胖者高于超重者,未婚高于丧偶(丧偶/分居),血脂异常者高于非血脂异常者,大专及以上文化程度者高于高中/中专/技校、初中和小学及以下,60~岁组最低,家庭年收入2.1~万元组最高,差异均有统计学意义(P<0.05)。从未测量过体重的比例为20.5%,女性高于男性,农村高于城市,非汉族高于汉族,丧偶/离婚/分居高于已婚/同居和未婚,西部地区高于中部和东部地区,超重者高于肥胖者,非血脂异常者高于血脂异常者,家庭年收入<0.7万元最高,60~岁年龄组最高,差异均有统计学意义(P<0.05)。见表 2。
3.体重测量情况多因素分析:采用复杂抽样设计的非条件logistic回归模型,将体重测量设定为应变量(是=1;否=0),性别、年龄、文化程度、婚姻状况、年收入、地区、城乡、BMI分组、是否患有糖尿病、是否患有高血压、是否患有血脂异常为自变量。结果显示,较高年龄阻碍体重测量行为的形成,而女性、较高文化程度、较高家庭年收入、糖尿病、血脂异常者更倾向于测量体重。见表 3。

体重是反映人体健康状况的基本测量指标。定期监测体重可及时、准确地掌握体重变化情况,对维持健康体重、促进健康具有重要意义[4]。体重测量被证明是辅助超重/肥胖人群成功减重并维持减重效果的重要干预策略,定期(每天或每周)测量体重可以帮助个体及时掌握体重状态,了解进食或身体活动与体重变化的关系,促使个体维持支持积极结果的行为改变,或对那些可能导致体重反弹或增重的行为采取纠正措施,以此来激励减肥行为[13]。
本研究结果显示,2013年我国超重/肥胖人群从未测量过体重的比例为20.5%,60.6%的超重/肥胖人群最近1次测量过体重的时间为1个月到1年以前,而1周内测量过体重者仅为18.9%,说明我国超重/肥胖人群关注自身体重的意识较低,自主监测体重的行为习惯还没有养成。2002-2010年,我国成年人体重测量率从59.9%上升至77.3%,而能够每月进行体重测量的仅占33.5%[14-16],但我国居民同期的超重/肥胖率则呈快速上升趋势,由2004年的23.1%和7.0%上升至2013年的32.4%和14.1%[17]。超重/肥胖是多种健康问题的重要危险因素[18],将体重控制在合理范围,可以减少慢性病的发生与发展并改善与肥胖相关的健康状况[19]。国家卫生健康委员会于2016年提出开展“三减三健”行动,保持健康体重是该专项活动的重要组成部分。大力推广自我体重测量技术既是防治超重/肥胖、维持健康体重、预防相关慢性病的基础,同时也可以促使超重/肥胖人群自觉形成每周或每天测量体重的行为习惯。同时,推广在工作场所、公共场所、医疗机构、家庭、学校等设立体重秤作为健康测量工具,有助于养成全民体重测量习惯,提高其自主监测的依从性。针对老年或伴有慢性病的超重/肥胖者,还应细化干预指导措施,设定合理减重目标,制定科学饮食运动方案。
国外研究也表明,超重成年人自我称重频率与健康体重控制行为之间存在正相关关系[20-23],每日和每周测量都会促使体重变化,但每天进行体重测量的超重人群实现了最佳的减肥效果。同时,监测体重并伴随相应的反馈,可有效地在男性超重者中产生微小但可持续的减重效果[6]。2013年,美国心脏学会(AHA)、美国心脏病学院(ACC)和肥胖学会(TOS)联合发布的《成人超重与肥胖管理指南》指出[24],对于超重/肥胖人群,为减小体重并维持减重效果,应规律进行体重测量(如每周或更频繁)。
综上所述,2013年我国超重/肥胖人群从未测量过体重的比例仍较低,尚未养成自主监测体重的行为习惯,相关机构还应继续加强体重测量知识的宣传和干预工作,以便养成全民体重测量习惯,更好的预防超重/肥胖引发的健康问题。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
李晓燕, 姜勇, 胡楠, 等. 2010年我国成年人超重及肥胖流行特征[J]. 中华预防医学杂志, 2012, 46(8): 683-686. Li XY, Jiang Y, Hu N, et al. Prevalence and characteristic of overweight and obesity among adults in China, 2010[J]. Chin J Prev Med, 2012, 46(8): 683-686. DOI:10.3760/cma.j.issn.0253-9624.2012.08.003 |
| [2] |
张娟, 施小明, 梁晓峰. 2010年中国城乡居民超重和肥胖的直接经济负担分析[J]. 中华流行病学杂志, 2013, 34(6): 598-600. Zhang J, Shi XM, Liang XF. Economic costs of both overweight and obesity among Chinese urban and rural residents, in 2010[J]. Chin J Epidemiol, 2013, 34(6): 598-600. DOI:10.3760/cma.j.issn.0254-6450.2013.06.014 |
| [3] |
Gross LS, Li L, Ford ES, et al. Increased consumption of refined carbohydrates and the epidemic of type 2 diabetes in the United States:an ecological assessment[J]. Am J Clin Nutr, 2004, 79(5): 774-779. DOI:10.1093/ajcn/79.5.774 |
| [4] |
徐海泉, 孙君茂, 马冠生. 合理膳食、适量运动维持健康体重[J]. 中国食物与营养, 2018, 24(1): 5-9. Xu HQ, Sun JM, Ma GS. Healthy diet and moderate exercise to maintain healthy body weight[J]. Food Nutr China, 2018, 24(1): 5-9. DOI:10.3969/j.issn.1006-9577.2018.01.001 |
| [5] |
Steinberg DM, Tate DF, Bennett GG, et al. The efficacy of a daily self-weighing weight loss intervention using smart scales and e-mail[J]. Obesity, 2013, 21(9): 1789-1797. DOI:10.1002/oby.20396 |
| [6] |
Pacanowski CR, Levitsky DA. Frequent self-weighing and visual feedback for weight loss in overweight adults[J]. J Obes, 2015, 2015: 763680. DOI:10.1155/2015/763680 |
| [7] |
王丽敏, 张梅, 李镒冲, 等. 2013年中国慢性病及其危险因素监测总体方案[J]. 中华预防医学杂志, 2018, 52(2): 191-194. Wang LM, Zhang M, Li YC, et al. Scheme of the Chinese chronic non-communicable disease and risk factor surveillance[J]. Chin J Prev Med, 2018, 52(2): 191-194. DOI:10.3760/cma.j.issn.0253-9624.2018.02.015 |
| [8] |
中国疾病预防控制中心, 中国疾病预防控制中心慢性非传染性疾病预防控制中心. 中国慢性病及其危险因素检测报告2013[M]. 北京: 军事医学出版社, 2015. China CDC, National Center for Chronic and Non-communicable Disease Control and Prevention. Report on chronic disease risk factor surveillance in China 2013[M]. Beijing: Military Medical Science Press, 2015. |
| [9] |
Wang LM, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013[J]. JAMA, 2017, 317(24): 2515-2523. DOI:10.1001/jama.2017.7596 |
| [10] |
刘勇, 王丽敏, 彭永祥, 等. 多中心血糖检测电子化质量监控系统的建立与实施[J]. 中华流行病学杂志, 2015, 36(5): 506-509. Liu Y, Wang LM, Peng YX, et al. Designing and implementation of a web-based quality monitoring system for plasma glucose measurement in multicenter population study[J]. Chin J Epidemiol, 2015, 36(5): 506-509. DOI:10.3760/cma.j.issn.0254-6450.2015.05.020 |
| [11] |
陈春明, 孔灵芝. 中国成人超重和肥胖症预防控制指南[M]. 北京: 人民卫生出版社, 2006. Chen CM, Kong LZ. The guideline for prevention and control of overweight and obesity in Chinese adults[M]. Beijing: People's Medical Publishing House, 2006. |
| [12] |
缪凡, 童峰. 复杂抽样数据的logistic回归分析方法及其应用[J]. 中国卫生统计, 2008, 25(6): 577-579. Miao F, Tong F. The Application of logistic regression in complex sample survey data[J]. Chin J Health Statist, 2008, 25(6): 577-579. DOI:10.3969/j.issn.1002-3674.2008.06.005 |
| [13] |
Mcguire MT, Wing RR, Klem M, et al. Behavioral strategies of individuals who have maintained long-term weight losses[J]. Obesity research, 1999, 7(4). |
| [14] |
姜勇, 张梅, 李镒冲, 等. 2010年我国成人体重自测及体重知晓情况分析[J]. 中国健康教育, 2013, 29(6): 485-488. Jiang Y, Zhang M, Li YC, et al. Investigation on self-measurement and awareness of body weight among Chinese adults in 2010[J]. Chin J Health Educ, 2013, 29(6): 485-488. DOI:10.16168/j.cnki.issn.1002-9982.2013.06.011 |
| [15] |
马冠生, 郝利楠, 胡小琪, 等. 我国成年居民测量体重、血压、血糖和血脂行为情况分析[J]. 中国健康教育, 2009, 25(1): 5-7. Ma GS, Hao LN, Hu XQ, et al. Analysis on the behavior of measuring the weight, blood pressure, blood glucose and blood lipids among Chinese adults[J]. Chin J Health Educ, 2009, 25(1): 5-7. DOI:10.16168/j.cnki.issn.1002-9982.2009.01.001 |
| [16] |
王卓群, 姜勇, 李镒冲. 成人体重测量情况分析[J]. 中华健康管理学杂志, 2010, 4(5): 319-320. Wang ZQ, Jiang Y, Li YC. Analysis on weight measurement among Chinese adults[J]. Chin J Health Manage, 2010, 4(5): 319-320. DOI:10.3760/cma.j.issn.1674-0815.2010.05.026 |
| [17] |
中国疾病预防控制中心, 中国疾病预防控制中心慢性非传染性疾病预防控制中心. 中国慢性病及其危险因素监测报告2010[M]. 北京: 军事医学科学出版社, 2012. China CDC, National Center for Chronic and Non-communicable Disease Control and Prevention. Report on chronic disease risk factor surveillance in China 2010[M]. Beijing: Military Medical Science Press, 2012. |
| [18] |
Guh DP, Zhang W, Bansback N, et al. The incidence of co-morbidities related to obesity and overweight:a systematic review and Meta-analysis[J]. BMC Public Health, 2009, 9: 88. DOI:10.1186/1471-2458-9-88 |
| [19] |
National Institute of Health. National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. The evidence report[J]. Obes Res 1998, 6: 51S-209S.
|
| [20] |
Linde JA, Jeffery RW, French SA, et al. Self-weighing in weight gain prevention and weight loss trials[J]. Ann Behav Med, 2005, 30(3): 210-216. DOI:10.1207/s15324796abm3003_5 |
| [21] |
Shieh C, Knisely MR, Clark D, et al. Self-weighing in weight management interventions:a systematic review of literature[J]. Obes Res Clin Pract, 2016, 10(5): 493-519. DOI:10.1016/j.orcp.2016.01.004 |
| [22] |
Bramante CT, Clark JM, Gudzune KA. Access to a scale and self-weighing habits among public housing residents[J]. Clin Obes, 2018, 8(4): 258-264. |
| [23] |
Steinberg DM, Bennett GG, Askew S, et al. Weighing every day matters:daily weighing improves weight loss and adoption of weight control behaviors[J]. J Acad Nutr Dietet, 2015, 115(4): 511-518. DOI:10.1016/j.jand.2014.12.011 |
| [24] |
Jensen MD, Ryan DH, Donato KA, et al. Guidelines (2013) for managing overweight and obesity in adults[J]. Obesity, 2014, 22(Suppl 2): S1-410. DOI:10.1002/oby.20818 |