 2019, Vol. 40
2019, Vol. 40文章信息
- 徐晓慧, 曾新颖, 王黎君, 刘韫宁, 刘江美, 齐金蕾, 殷鹏, 周脉耕.
- Xu Xiaohui, Zeng Xinying, Wang Lijun, Liu Yunning, Liu Jiangmei, Qi Jinlei, Yin Peng, Zhou Maigeng.
- 1990年与2017年中国胰腺癌疾病负担分析
- The disease burden of pancreatic cancer in China in 1990 and 2017
- 中华流行病学杂志, 2019, 40(9): 1084-1088
- Chinese Journal of Epidemiology, 2019, 40(9): 1084-1088
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.09.012
-
文章历史
收稿日期: 2019-02-25




2. 中国疾病预防控制中心慢性非传染性疾病预防控制中心, 北京 100050
2. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
胰腺癌病死率较高,近年来全球总发病人数有不断增加的趋势[1-2]。据全球肿瘤统计数据结果显示,2012年胰腺癌造成约33万人死亡,占全球肿瘤死亡人数第7位[3]。有研究估计,2018年全球胰腺癌新发病例约45.89万人,死亡43.22万人[4]。有研究预测,胰腺癌在一些国家的死亡人数会超过乳腺癌位列恶性肿瘤第3位[5]。胰腺癌在发达国家发病率较高,在发展中国家较低[6-7]。胰腺癌预后极差,1年生存率约为18%左右[8],中位生存时间为6~9个月,5年生存率约为5%左右[9]。本研究利用2017年全球疾病负担研究(GBD2017)结果,分析我国胰腺癌发病、死亡情况并估算胰腺癌的疾病负担及其变化情况,为我国制定有效的胰腺癌防控策略、降低胰腺癌的疾病负担提供参考。
资料与方法1.资料来源:GBD2017在已有研究方法的基础上改进分析策略,增加高质量数据量,利用统一、可比的方法,量化估计、分析了全球195个国家和地区的354种疾病或伤害、3 484种疾病后遗症的疾病负担,同时在全球范围内通过问卷调查对3 484种后遗症的伤残权重进行估计。GBD2017对中国疾病负担的估计利用了多种来源的数据,死亡数据主要来自于全国疾病监测点系统死因监测、中国CDC死因登记报告信息系统、全国肿瘤登记数据、全国妇幼卫生监测网、中国香港地区和中国澳门地区的死因数据,以及一些已发表的文献或报告;胰腺癌发病数据来源于全国肿瘤登记系统、已发表文献和疾病监测系统等,其他数据来源及具体分析方法详见文献[10-12]。本研究采用GBD2017中国1990-2017年分省的数据。
2.疾病分类与编码:采用《国际疾病分类》第9版(ICD-9)和第10版(ICD-10)对死因数据进行编码,经垃圾编码再分配后重新分类映射到GBD死因分类中。本研究中胰腺癌的ICD-9编码范围为157~157.9、211.6~211.7;ICD-10编码范围为C25~C25.9、D13.6~D13.7。
3.分析方法和指标:GBD2017采用整体建模策略估计胰腺癌死亡数和死亡率,采用全国肿瘤登记系统报告的胰腺癌发病数和死亡数,计算监测地区人群的发病率和死亡率,用死亡率除以发病率估算不同年份分性别、年龄组的胰腺癌死亡发病比,以死亡发病比估算人群发病数据[10, 12]。采用伤残调整寿命年(DALY)作为疾病负担评价指标,DALY包括过早死亡损失寿命年(YLL)和伤残损失寿命年(YLD)。某年龄组寿命损失年的计算方法是将某年龄组胰腺癌死亡人数乘以该年龄组平均死亡年龄所对应的期望寿命,全人群的寿命损失年为各性别、年龄组的寿命损失年总和,其中DALY=YLL+YLD,YLL和YLD的估算方法见文献[10-11]。各年龄组YLL率、YLD率和DALY率为各年龄组寿命损失年数除以该年龄组人口数。以GBD2017世界标准人口计算标化死亡率、标化发病率、标化DALY率、标化YLL率和标化YLD率。
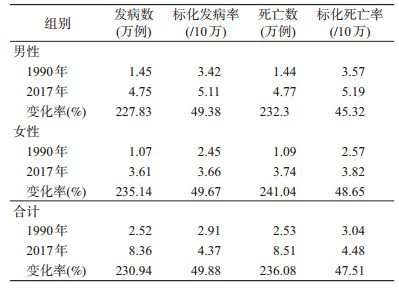
结果1.胰腺癌发病及死亡情况:与1990年相比,2017年我国胰腺癌发病、死亡人数均有所增加,发病率、死亡率也有所增加。2017年中国胰腺癌发病人数为8.36万,标化发病率为4.37/10万,较1990年分别增长230.94%和49.88%,其中男性发病人数为4.75万人,女性3.61万人,男性标化发病率大于女性。2017年死亡人数8.51万,标化死亡率为4.48/10万,较1990年分别上升236.08%和47.51%,其中男性死亡4.77万人,女性死亡3.74万人,男性标化死亡率大于女性。见表 1。
2.胰腺癌年龄别发病及死亡情况:无论1990年还是2017年,在50岁之前胰腺癌发病率较低,随着年龄增加而升高。2017年85~89岁年龄组出现发病率峰值,随后略有下降,1990年胰腺癌发病率90~94岁年龄组最高,在95岁以上出现下降。2017年15~49岁人群发病率水平接近1990年,但从55~59岁年龄组开始有大幅增加,80~84岁年龄组增幅最大,85~89岁年龄组发病率最高,见图 1。死亡情况和发病情况在各年龄组之间的变化模式大致相同,见图 2。

|
| 图 1 1990年与2017年中国各年龄组胰腺癌发病率 |

|
| 图 2 1990年与2017年中国各年龄组胰腺癌死亡率 |
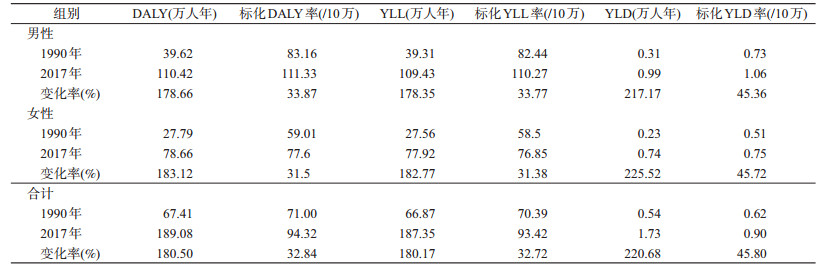
3.胰腺癌疾病负担及其变化情况:我国人群胰腺癌造成的DALY由1990年的67.41万人年增长到2017年的189.08万人年,增长180.50%;1990年及2017年,YLL和YLD均有不同程度的增长,其中YLD增长率更高。标化DALY率由71.00/10万增长到94.32/10万,增长率为32.84%。YLL率、标化YLL率、YLD率及标化YLD率均有大幅增长。1990年和2017年男性各项疾病负担指标均高于女性,变化率相差不大。见表 2。
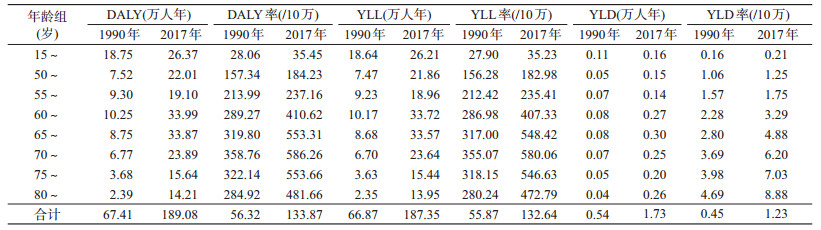
4.胰腺癌疾病负担的年龄分布:与1990年相比,2017年各年龄组的DALY、YLL和YLD均有较大幅度增长,60~79岁年龄组增量最大。2017年DALY、YLL在60~64岁达到最大值,分别为33.99万人年和33.72万人年,比1990年分别增长23.74万人年和23.55万人年,YLD在65~69岁年龄组中达到最大值0.30万人年。
2017年,在<75岁人群中胰腺癌DALY率、YLL率和YLD率随年龄增长呈上升趋势,DALY率和YLL率在70~74岁年龄组达到顶峰后逐渐下降。70~74岁年龄组DALY率在1990年和2017年分别为358.76/10万、586.26/10万。与1990年相比,DALY率、YLL率和YLD率均有大幅增长,以65~69岁年龄组最为显著,见表 3。
5.胰腺癌标化死亡率各省分布情况:2017年胰腺癌标化死亡率排名前6位的省份分别是江苏(7.61/10万)、上海(7.52/10万)、辽宁(6.84/10万)、黑龙江(6.48/10万)、天津(5.91/10万)和浙江(5.83/10万)。相比1990年,标化死亡率增长率最高的5个省份分别为河南(104.28%)、四川(94.02%)、河北(90.39%)、广西(88.56%)、陕西(83.72%)。33个省份中,有3个省份的胰腺癌标化死亡率出现下降,分别是香港地区(-11.28%)、北京(-7.56%)、澳门地区(-1.69%),见表 4。

本研究结果显示,2017年我国胰腺癌发病、死亡人数较1990年有所增加,标化发病率和标化死亡率有大幅升高,DALY、YLD和YLL及其标化率均有增加,疾病负担加重。男性胰腺癌各项疾病负担指标均高于女性,但女性增速略高于男性。胰腺癌在高年龄组发病较多,85~89岁年龄组胰腺癌发病率、死亡率最高,15~49岁年龄组发病罕见。
我国2017年胰腺癌标化发病率为4.37/10万,低于全球水平(5.69/10万)[10],且低于2012年亚洲发病率最高的东亚地区平均水平(4.5/10万)[13]。标化发病率和标化死亡率与1990年相比分别增加了49.88%和47.51%,上升速度高于全球(13.52%和10.28%[10, 12])。有研究表明,全球胰腺癌发病水平分布不均衡,人类发展指数(HDI)与胰腺癌发病和死亡有关,2012年胰腺癌在北美和西欧一些国家发病率和死亡率最高,在中非和亚洲中南部发病率最低[14]。
2017年我国胰腺癌标化死亡率在各省间有较大差异,东部经济较发达的地区较高,排名前6位的省份(江苏、上海、辽宁、黑龙江、天津和浙江)胰腺癌标化死亡率均超过全球平均水平。据国家癌症中心肿瘤登记结果显示,我国东部地区胰腺癌发病率最高,其次是中部和西部地区,呈现城乡及地域分布差异性[15-16],与本研究结果相近,可能与区域经济发展水平、医疗资源、危险因素分布不均有关。从标化死亡率变化情况来看,河南、四川、河北、广西、陕西等省份增长较快,也可能与诊断技术、报告水平提高有关。北京、香港和澳门地区的胰腺癌标化死亡率出现下降,其原因有待探究。东部地区应重视胰腺癌防控工作,中部、西部地区也需做好应对准备。
胰腺癌患者生存时间短,YLD远小于YLL,但标化YLD率的增长速度高于标化YLL率。表明胰腺癌造成的疾病负担主要来自早死所致寿命损失,但伤残负担加重。从疾病负担的年龄分布来看,DALY率、YLL率、YLD率均随年龄增加而增大,>60岁人群DALY率较高,70~74岁年龄组DALY率最高。各年龄组在1990-2017年间疾病负担均有所加重,55~64岁年龄组DALY率增幅最大,应引起重视。
本研究数据显示,1990年我国胰腺癌死亡人数仅占所有恶性肿瘤死亡人数的1.79%,位居第10位,但2017年上升到3.26%,位居第7位,且仍具有上升趋势。造成胰腺癌发病、死亡增多的原因:人群健康意识增强,体检率上升以及医疗技术手段的进步使得胰腺癌的临床检出和发现能力提高;人口老龄化、胰腺癌相关危险因素水平升高;肿瘤及死因登记等监测系统的完善;相较于其他恶性肿瘤更少的投入导致胰腺癌诊疗技术发展受限等[1]。目前,胰腺癌的发病机制尚不明确,但有文献表明,吸烟[17]、饮酒[18]、不良饮食习惯[19]等可能是胰腺癌发病的危险因素,饮酒可能通过增加糖尿病或慢性胰腺炎的风险来促进致癌作用[20]。近年来我国人群吸烟率和饮酒大幅增长[21-22],不良饮食习惯增多[23],提示胰腺癌发病风险增加。本研究结果发现男性发病率和死亡率高于女性,可能与男性吸烟、饮酒较多有关。因胰腺癌的疾病负担在高龄组高于低龄组,随着人口老龄化进程的加快,我国胰腺癌疾病负担可能会进一步加重,应引起重视并采取综合防控措施。迄今仍未找到有效的胰腺癌早期筛查及治疗手段,做好预防是最重要的防控策略,研究胰腺癌的发病机制以识别并降低危险因素水平是预防的关键。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
Wu WR, He XK, Yang LY, et al. Rising trends in pancreatic cancer incidence and mortality in 2000-2014[J]. Clin Epidemiol, 2018, 10: 789-797. DOI:10.2147/CLEP.S160018 |
| [2] |
Are C, Chowdhury S, Ahmad H, et al. Predictive global trends in the incidence and mortality of pancreatic cancer based on geographic location, socio-economic status, and demographic shift[J]. J Surg Oncol, 2016, 114(6): 736-742. DOI:10.1002/jso.24410 |
| [3] |
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide:sources, methods and major patterns in GLOBOCAN 2012[J]. Int J Cancer, 2015, 136(5): E359-386. DOI:10.1002/ijc.29210 |
| [4] |
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA:A Cancer J Clin, 2018, 68(6): 394-424. DOI:10.3322/caac.21492 |
| [5] |
Ferlay J, Partensky C, Bray F. More deaths from pancreatic cancer than breast cancer in the EU by 2017[J]. Acta Oncol, 2016, 55(9/10): 1158-1160. DOI:10.1080/0284186X.2016.1197419 |
| [6] |
Ilic M, Ilic I. Epidemiology of pancreatic cancer[J]. World J Gastroenterol, 2016, 22(44): 9694-9705. DOI:10.3748/wjg.v22.i44.9694 |
| [7] |
Lin QJ, Yang F, Jin C, et al. Current status and progress of pancreatic cancer in China[J]. World J Gastroenterol, 2015, 21(26): 7988-8003. DOI:10.3748/wjg.v21.i26.7988 |
| [8] |
Hidalgo M, Cascinu S, Kleeff J, et al. Addressing the challenges of pancreatic cancer:future directions for improving outcomes[J]. Pancreatology, 2015, 15(1): 8-18. DOI:10.1016/j.pan.2014.10.001 |
| [9] |
中国临床肿瘤学会胰腺癌专家委员会. 胰腺癌综合诊治中国专家共识(2014年版)[J]. 临床肿瘤学杂志, 2014, 19(4): 358-370. The Chinese Society of Clinical Oncology Pancreatic Cancer Expert Committee. Chinese consensus on pancreatic cancer diagnosis and treatment (2014 version)[J]. Chin Clin Oncol, 2014, 19(4): 358-370. DOI:10.3969/j.issn.1001-5256.2014.10.002 |
| [10] |
James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1789-1858. DOI:10.1016/S0140-6736(18)32279-7 |
| [11] |
Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1859-1922. DOI:10.1016/S0140-6736(18)32335-3 |
| [12] |
Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1736-1788. DOI:10.1016/S0140-6736(18)32203-7 |
| [13] |
Pourhoseingholi MA, Ashtari S, Hajizadeh N, et al. Systematic review of pancreatic cancer epidemiology in Asia-Pacific Region:major patterns in GLOBACON 2012[J]. Gastroenterol Hepatol Bed Bench, 2017, 10(4): 245-257. DOI:10.22037/ghfbb.voio.1160 |
| [14] |
Veisani Y, Jenabi E, Khazaei S, et al. Global incidence and mortality rates in pancreatic cancer and the association with the Human Development Index:decomposition approach[J]. Publ Health, 2018, 156: 87-91. DOI:10.1016/j.puhe.2017.12.015 |
| [15] |
陈万青, 孙可欣, 郑荣寿, 等. 2014年中国分地区恶性肿瘤发病和死亡分析[J]. 中国肿瘤, 2018, 27(1): 1-14. Chen WQ, Sun KX, Zheng RS, et al. Report of cancer incidence and mortality in different areas of China, 2014[J]. China Cancer, 2018, 27(1): 1-14. DOI:10.11735/j.issn.1004-0242.2018.01.A001 |
| [16] |
孙可欣, 郑荣寿, 张思维, 等. 2015年中国分地区恶性肿瘤发病和死亡分析[J]. 中国肿瘤, 2019, 28(1): 1-11. Sun KX, Zheng RS, Zhang SW, et al. Report of cancer incidence and mortality in different areas of China, 2015[J]. China Cancer, 2019, 28(1): 1-11. DOI:10.11735/j.issn.1004-0242.2019.01.A001 |
| [17] |
Vrieling A, Bueno-de-Mesquita HB, Boshuizen HC, et al. Cigarette smoking, environmental tobacco smoke exposure and pancreatic cancer risk in the European Prospective Investigation into Cancer and Nutrition[J]. Int J Cancer, 2010, 126(10): 2394-2403. DOI:10.1002/ijc.24907 |
| [18] |
Jarosz M, Sekula W, Rychlik E. Influence of diet and tobacco smoking on pancreatic cancer incidence in Poland in 1960-2008[J]. Gastroenterol Res Pract, 2012, 2012: 682156. DOI:10.1155/2012/682156 |
| [19] |
Welsch T, Kleeff J, Seitz HK, et al. Update on pancreatic cancer and alcohol-associated risk[J]. J Gastroenterol Hepatol, 2006, 21(Suppl 3): S69-75. DOI:10.1111/j.1440-1746.2006.04574.x |
| [20] |
Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma[J]. N Engl J Med, 2014, 371(11): 1039-1049. DOI:10.1056/NEJMra1404198 |
| [21] |
Wang MH, Luo X, Xu SB, et al. Trends in smoking prevalence and implication for chronic diseases in China:serial national cross-sectional surveys from 2003 to 2013[J]. Lancet Respir Med, 2019, 7: 35-45. DOI:10.1016/S2213-2600(18)30432-6 |
| [22] |
World Health Organization. Global status report on alcohol and health 2018[R]. Geneva, Switzerland: WHO, 2018.
|
| [23] |
Zhai FY, Du SF, Wang ZH, et al. Dynamics of the Chinese diet and the role of urbanicity, 1991-2011[J]. Obes Rev, 2014, 15(Suppl 1): 16-26. DOI:10.1111/obr.12124 |