 2019, Vol. 40
2019, Vol. 40文章信息
- 林声, 潘浩, 肖文佳, 宫霄欢, 匡小舟, 滕峥, 张曦, 吴寰宇.
- Lin Sheng, Pan Hao, Xiao Wenjia, Gong Xiaohuan, Kuang Xiaozhou, Teng Zheng, Zhang Xi, Wu Huanyu.
- 上海市2013-2018年成年人诺如病毒引发感染性腹泻的流行特征研究
- Epidemiologic characteristics of Norovirus among adult patients with infectious diarrhea, in Shanghai, 2013-2018
- 中华流行病学杂志, 2019, 40(8): 883-888
- Chinese journal of Epidemiology, 2019, 40(8): 883-888
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.08.003
-
文章历史
收稿日期: 2019-03-11




感染性腹泻是由病毒、细菌、寄生虫等病原体感染引起,以排便次数增加及粪便性状改变为特征[1]。据WHO估计,全球每年因感染性腹泻死亡的人数高达160万人,全人群的损失生命年超过7 000万人年,死因顺位排在第五位,是全球重大公共卫生问题之一[2]。诺如病毒是导致成年人因腹泻就诊和住院最常见原因,也是5岁以下儿童因腹泻就诊和住院第二位原因(仅次于轮状病毒)[3-4]。由于缺乏快速、敏感和符合成本效益的临床诊断方法,诺如病毒对全人群健康的影响在很多地区和国家被严重低估[5-6]。诺如病毒每2~4年就会出现一种新的大流行毒株,给人类健康带来巨大影响[4, 7]。近年来国内外对儿童诺如病毒引发的感染性腹泻开展大量研究,但覆盖成年人的研究少有报告[8-11]。本研究根据上海市2013-2018年在22家监测点医院就诊人群中开展腹泻病症状监测的数据,对诺如病毒引发的感染性腹泻的临床症状、流行病学和病原学特征进行分析,了解上海市成年人感染性腹泻的年龄、季节性分布和流行基因型别的特征,为制定诺如病毒引发的感染性腹泻防控策略和开展疾病负担研究提供科学依据。
对象与方法1.监测点医院:采用概率比例抽样方法选择监测点医院,采用系统抽样方法选择采样病例。将上海市开设肠道门诊的医院按医院级别(一、二、三级)、郊区和市区共分成6个层级,根据各医院初诊感染性腹泻病例数和实际可承担工作量,确定各层级监测点医院数量和抽样采样比例。最终选定22家成年人感染性腹泻监测点医院,其中9家市区监测点医院(一、二、三级医院分别有2、3、4家)和13家郊区监测点医院(一、二、三级医院分别有7、4、2家);抽样采样比例为1 : 3至1 : 20不等。
2.监测对象:凡在监测点医院肠道门诊就诊,年龄≥15岁,24 h内腹泻≥3次,且伴有粪便性状改变(如水样便、稀软便等)[1]。
3.监测方法:监测对象就诊时,医务人员除临床问诊和体格检查外,根据上海市CDC统一设计的调查问卷,通过访谈形式对监测对象开展包括人口学特征(性别、年龄、职业、住址等)、流行病学史(不洁饮食史、不洁饮水史、外出史、聚餐史等)、主要症状与体征(发热、呕吐、腹泻、腹痛等)、诊疗信息(发病日期、就诊日期、药物使用情况、实验室检查等)等内容调查,并由医务人员现场采集粪便标本,上述内容直接录入至上海市CDC设计的“上海市腹泻病综合监测信息系统”。
4.样本采集、运输及检测:将采集的5 g粪便标本置于清洁不加任何试剂的无菌采样杯。标本按规定保存(4 ℃短期保存或-20 ℃冰箱储存)并及时送至监测点医院所在区CDC检测。诺如病毒采用实时荧光定量反转录-聚合酶链式反应(real-time fluorescencequantitative reverse transcription polymerase chainreaction,rRT-PCR)进行核酸扩增检测,仪器为德国罗氏公司生产的实时荧光定量PCR仪,采用上海之江生物科技有限公司的相应商业化试剂盒,操作方法和结果判定均按说明书要求进行。
5.质量控制:市、区两级CDC定期对监测点医院的医务人员开展业务培训和现场质控督导。区CDC每月将阳性标本以及5%阴性标本送至市CDC复核,采用rRT-PCR进行质控检测,以保证现场调查与实验室检测的质量。如果区CDC检出阳性,市CDC检出阴性,判定结果为阳性;如果区CDC检出阴性,市CDC检出阳性,则进行第3次检测,结果若仍为阳性,则判定为阳性,结果为阴性,则判定为阴性。
6.统计学分析:采用SPSS 16.0和Excel 2016软件进行统计学分析和图表绘制。不同组别阳性率、构成比差异采用Pearson χ2检验,所有统计学检验均为双侧检验,以P<0.05为差异有统计学意义;多因素分析采用非条件logistic回归,回归模型拟采用Backward LR法,入选标准α1=0.05,排除标准α2=0.10,检验水准α=0.05。根据全球疾病负担和监测感染性腹泻病例的年龄分布,分为15~、30~、45~和≥60岁组[12]。
结果1.监测基本情况:2013年8月1日至2018年6月30日,22家成年人腹泻病监测点医院共登记初诊腹泻病例120 229例。男性58 103例(48.33%),女性62 126例(51.67%)。年龄最小15岁,最大105岁,M=42岁(IQR:29~59岁)。
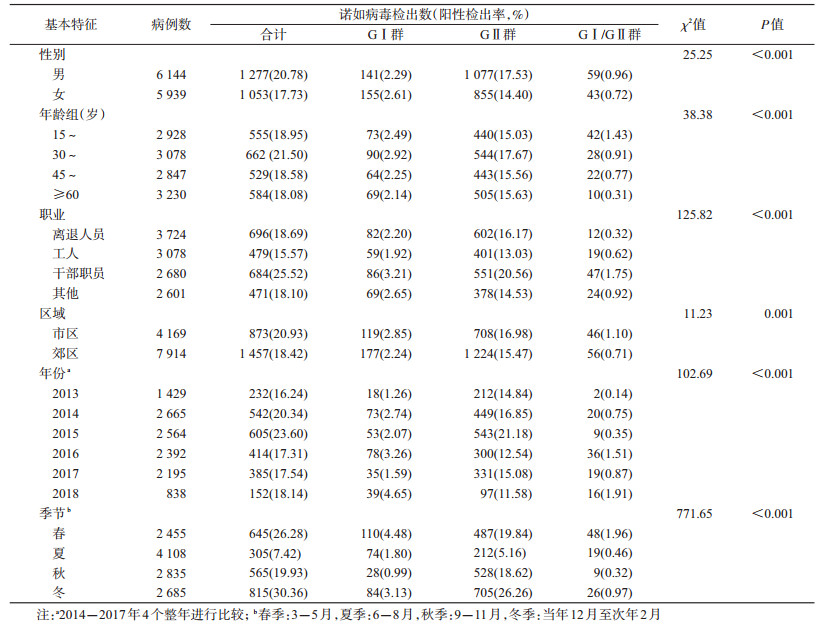
2.阳性检出情况:12 083例感染性腹泻病例采集了粪便标本,就诊采样比为9.95;诺如病毒阳性病例2 330例,阳性检出率为19.28%。其中男性检出率(20.78%)高于女性(17.73%),差异有统计学意义(χ2=25.25,P<0.001);30~岁组人群诺如病毒检出率最高(21.50%),≥60岁老年人群最低(18.08%);2015年检出率最高(23.60%),2016年最低(17.31%);市区医院检出率(20.93%)高于郊区医院(18.42%),上述差异均有统计学意义(P<0.05),见表 1。诺如病毒引起的感染性腹泻全年均可发生,但季节性发病特征明显,以10月至次年4月为高发季节,7-8月为低谷期(图 1)。

|
| 图 1 2013-2018年上海市22家监测点医院诺如病毒感染病例阳性检出率分布 |
3.诺如病毒基因分群:2 330例诺如病毒检测阳性病例,其中诺如病毒GⅠ群296例,阳性检出率为2.45%;诺如病毒GⅡ群1 932例,阳性检出率为15.99%;诺如病毒GⅠ群与诺如病毒GⅡ群混合感染为102例,阳性检出率为0.84%。不同诺如病毒基因群别的构成比在不同性别、年龄组、职业、年份、季节的差异均有统计学意义,但不同区域的差异无统计学意义,见表 1。
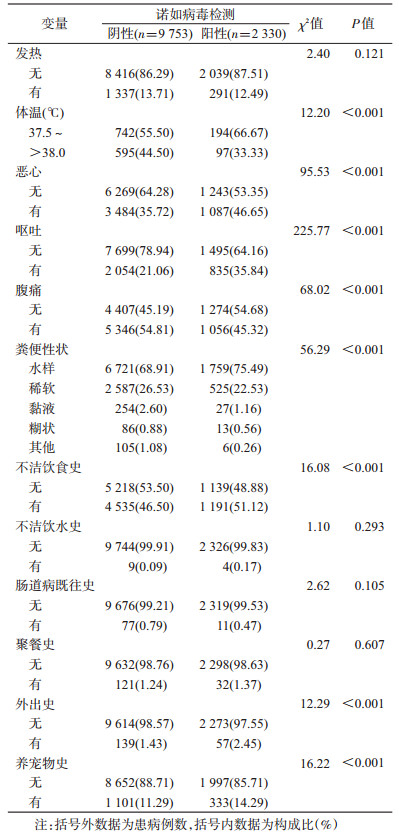
4.诺如病毒引发的感染性腹泻病例主要临床表现和流行病学史:2 330例诺如病毒检测阳性病例中,粪便性状以水样便居多(1 759例,75.49%),其次为稀软便(525例,22.53%);有腹痛者1 056例(45.32%),主要为阵发性腹痛(1 024例);有呕吐者835例(35.84%),呕吐频率以1~3次/d居多(642例,76.89%)。有不洁饮食史者1 191例(51.12%),主要为食用不洁肉与肉制品(486例,32.96%)、海水产品(401例,27.17%)和果蔬类(178例,12.10%)。诺如病毒检测阳性病例组水样便及呕吐的构成比高于诺如病毒检测阴性组,差异有统计学意义,见表 2。
5.诺如病毒引发的感染性腹泻发生的多因素分析:女性感染性腹泻诺如病毒检出率低于男性(OR=0.839,95%CI:0.759~0.919,P<0.001);30~岁组人群感染性腹泻诺如病毒检出率高于≥60岁老年人群(OR=1.258,95%CI:1.043~1.518,P=0.016);干部职员人群感染性腹泻诺如病毒检出率高于其他人群(OR=1.372,95%CI:1.194~1.577,P<0.001);发病前1周内有外出史感染性腹泻患者诺如病毒检出率高于无外出史人群(OR=1.479,95%CI:1.068~2.048,P=0.018);冬季诺如病毒引发的感染性腹泻发生率高于春、夏、秋季,见表 3。

诺如病毒理化抵抗力强、变异快、感染剂量低,感染后排毒时间长、免疫保护周期短、缺乏交叉保护,且传播途径多样,全人群普遍易感[4]。过往研究主要集中于儿童诺如病毒引发的感染性腹泻[5, 8],且研究数据主要来源于暴发疫情[6, 13]。本研究基于上海市建立的腹泻病综合监测体系,在全市范围采用概率比例抽样方法选择监测点医院,并采用系统抽样选择采样病例,开展长时间、系统、连续的主动监测,对上海市成年人中诺如病毒的散发感染进行研究。与其他研究相比[14-15],本研究有更好的代表性和外推性。
本研究发现,上海市成年人群感染性腹泻病例中,诺如病毒检出率为19.28%,提示诺如病毒对上海市成年人群健康的影响不容忽视。本研究结果与Ahmed等[5]结果(18%,95%CI:17%~20%)接近,高于全国平均检出率(11.6%)[10, 16-18],但与发达国家(地区)诺如病毒平均检出率(20%,95%CI:17%~22%)接近[5]。可能原因是低收入国家(地区)由于细菌和寄生虫的多样性,导致感染性腹泻总体发病率增加,因此,在感染性腹泻患者中,诺如病毒可能不那么普遍;同时,2012年出现了新的诺如病毒变异株Sydney_2012[19-20],导致多个地区和国家的诺如病毒阳性检出率普遍升高。
本研究发现,上海市诺如病毒引发的感染性腹泻以10月至次年4月为高发季节,符合其全年均可发生,但在温带气候地区有明显的冬、春季季节性高峰的特点[21-22]。寒冷干燥的冬、春季更适合病毒生存,社会行为的变革也可能增加人与人之间及食源性传播的可能性。本研究结果显示,30~岁组人群的检出率(21.50%)最高,≥60岁老年人群的检出率(18.08%)最低,30~岁组人群感染风险(OR=1.258,95%CI:1.043~1.518)高于≥60岁老年人群,与过往研究发现的老年人群比其他年龄组更容易感染诺如病毒结果不一致[23-24],提示该人群可能是诺如病毒感染高危人群,可能与其接触诺如病毒感染的食品、物品等机会较多有关。干部职员和男性也是诺如病毒感染的危险因素。
本研究显示,诺如病毒引发的感染性腹泻临床表现以水样便(75.49%)为主,发热以37.5~℃(66.67%)为主;诺如病毒引发的感染性腹泻腹痛比例(45.32%)明显低于非诺如病毒引发的感染性腹泻(54.81%),但其恶心(46.65%)、呕吐(35.84%)等症状的比例明显高于非诺如病毒引发的感染性腹泻,也增加了诺如病毒人传人概率[4],同时提示诺如病毒感染多伴有水样便、恶心、呕吐等症状,对临床诊疗有一定的指导作用。发病期5 d有不洁饮食史(OR=1.074,95%CI:0.973~1.184)、外出史(OR=1.479,95%CI:1.068~2.048)均增加感染诺如病毒的风险。因此,应大力开展饮食卫生督导、普及健康教育、提高居民的卫生意识、加强呕吐物消毒等。
本研究发现,诺如病毒GⅡ群始终是上海市诺如病毒引发感染性腹泻的主要基因型(12.70%GⅠ群、82.92%GⅡ群、4.38%GⅠ/GⅡ群)。虽然GⅠ群和GⅡ群同样存在多种型别,但从20世纪90年代起,GⅡ.4基因型即为造成全球急性胃肠炎暴发的主要毒株。不同诺如病毒基因群别的构成比在不同性别、年龄组、职业、年份、季节的差异均有统计学意义。国外研究认为,诺如病毒基本上每隔2~4年就发生1次变异并产生新的变异株流行株,导致诺如病毒感染暴发或流行[4]。因此,新变异株的出现和流行可能是导致上海市诺如病毒在成年人群和时间季节上分布差异的重要原因。
综上所述,上海市成年人腹泻患者诺如病毒感染率高,诺如病毒引起的感染性腹泻全年均可发生,但发病有明显的冬、春季节性,在诺如病毒引发的感染性腹泻的防控工作中应针对不同年龄、性别、不同季节采取特异性防控措施。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
World Health Organization. Diarrhoea[EB/OL].[2018-12-25]. https://www.who.int/topics/diarrhoea/en/.
|
| [2] |
GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017:a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1736-1788. DOI:10.1016/S0140-6736(18)32203-7 |
| [3] |
Lopman B, Vennema H, Kohli E, et al. Increase in viral gastroenteritis outbreaks in Europe and epidemic spread of new Norovirus variant[J]. Lancet, 2004, 363(9410): 682-688. DOI:10.1016/S0140-6736(04)15641-9 |
| [4] |
Glass RI, Parashar UD, Estes MK. Norovirus gastroenteritis[J]. N Engl J Med, 2009, 361(18): 1776-1785. DOI:10.1056/NEJMra0804575 |
| [5] |
Ahmed SM, Hall AJ, Robinson AE, et al. Global prevalence of Norovirus in cases of gastroenteritis:a systematic review and Meta-analysis[J]. Lancet Infect Dis, 2014, 14(8): 725-730. DOI:10.1016/S1473-3099(14)70767-4 |
| [6] |
Lu J, Sun L, Fang L, et al. Gastroenteritis Outbreaks Caused by Norovirus GⅡ.17, Guangdong province, China, 2014-2015[J]. Emerg Infect Dis, 2015, 21(7): 1240-1242. DOI:10.3201/eid2107.150226 |
| [7] |
Hall AJ, Rosenthal M, Gregoricus N, et al. Incidence of acute gastroenteritis and role of Norovirus, Georgia, USA, 2004-2005[J]. Emerg Infect Dis, 2011, 17(8): 1381-1388. DOI:10.3201/eid1708.101533 |
| [8] |
Walker CLF, Rudan I, Liu L, et al. Global burden of childhood pneumonia and diarrhoea[J]. Lancet, 2013, 381(9875): 1405-1416. DOI:10.1016/S0140-6736(13)60222-6 |
| [9] |
Zeng M, Xu XH, Zhu CM, et al. Clinical and molecular epidemiology of Norovirus infection in childhood diarrhea in China[J]. J Med Virol, 2012, 84(1): 145-151. DOI:10.1002/jmv.22248 |
| [10] |
郑书发, 余斐, 陈晓, 等. 2009-2014年浙江省哨点医院急性腹泻患者病原监测研究[J]. 中华预防医学杂志, 2016, 50(12): 1084-1090. Zheng SF, Yu F, Chen X, et al. Monitoring and research on pathogen spectrum in patients with acute diarrhea from sentinel hospital of Zhejiang province during 2009 to 2014[J]. Chin J Prev Med, 2016, 50(12): 1084-1090. DOI:10.3760/cma.j.issn.0253-9624.2016.12.012 |
| [11] |
孙立梅, 李晖, 谭小华, 等. 2012年广东省5岁以下儿童腹泻病流行特征及重点病原监测[J]. 中华流行病学杂志, 2013, 34(10): 989-992. Sun LM, Li H, Tan XH, et al. Epidemiological and etiological characteristics of diarrheal disease among children under 5 years of age in Guangdong province, in 2012[J]. Chin J Epidemiol, 2013, 34(10): 989-992. DOI:10.3760/cma.j.issn.0254-6450.2013.10.011 |
| [12] |
World Health Organization. Global burden of disease 2000: Version 2 methods and results[EB/OL].[2018-12-25]. https://www.who.int/healthinfo/paper50.pdf?ua=1.
|
| [13] |
Fu J, Ai J, Jin M, et al. Emergence of a new GⅡ.17 Norovirus variant in patients with acute gastroenteritis in Jiangsu, China, September 2014 to March 2015[J]. Eurosurveillance, 2015, 20(24): 21157. DOI:10.2807/1560-7917.ES2015.20.24.21157 |
| [14] |
Liu LJ, Liu W, Liu YX, et al. Identification of Norovirus as the top enteric viruses detected in adult cases with acute gastroenteritis[J]. Am J Trop Med Hyg, 2010, 82(4): 717-722. DOI:10.4269/ajtmh.2010.09-0491 |
| [15] |
Yen C, Wikswo ME, Lopman BA, et al. Impact of an Emergent Norovirus variant in 2009 on Norovirus outbreak activity in the United States[J]. Clin Infect Dis, 2011, 53(6): 568-571. DOI:10.1093/cid/cir478 |
| [16] |
余建兴, 赖圣杰, 王鑫, 等. 中国27省(市、自治区)2009-2013年门诊腹泻病例诺如病毒流行特征分析[J]. 中华流行病学杂志, 2015, 36(3): 199-204. Yu JX, Lai SJ, Wang X, et al. Analysis of epidemiology characteristics of Norovirus among diarrheal outpatients in 27 provinces in China, 2009-2013[J]. Chin J Epidemiol, 2015, 36(3): 199-204. DOI:10.3760/cma.j.issn.0254-6450.2015.03.003 |
| [17] |
安淑一, 赵卓, 郭军巧, 等. 辽宁省2009年至2011年病毒性腹泻流行病学研究[J]. 中华传染病杂志, 2013, 31(3): 166-169. An SY, Zhao Z, Guo JQ, et al. Epidemiological study on viral diarrhea during 2009-2011 in Liaoning province[J]. Chin J Infect Dis, 2013, 31(3): 166-169. DOI:10.3760/cma.j.issn.1000-6680.2013.03.007 |
| [18] |
刘白薇, 高志勇, 王全意, 等. 北京市2013-2014年肠道门诊腹泻患者中诺如病毒感染的流行病学及临床特征分析[J]. 中华流行病学杂志, 2015, 36(4): 383-386. Liu BW, Gao ZY, Wang QY, et al. Epidemiological and clinical features of Norovirus infection among diarrhea patients from the enteric clinics in Beijing, 2013-2014[J]. Chin J Epidemiol, 2015, 36(4): 383-386. DOI:10.3760/cma.j.issn.0254-6450.2015.04.019 |
| [19] |
van Beek J, Ambert-Balay K, Botteldoorn N, et al. Indications for worldwide increased Norovirus activity associated with emergence of a new variant of genotype Ⅱ.4, late 2012[J]. Euro Surveill, 2013, 18(1): 8-9. |
| [20] |
沈震, 王刚, 宰淑蓓, 等. 诺如病毒新型GⅡ.4流行株Sydney_2012在上海地区的检出和鉴定[J]. 病毒学报, 2013, 29(6): 608-613. Shen Z, Wang G, Zai SB, et al. Detection and identification of Norovirus new GⅡ.4 strain Sydney_2012 in Shanghai[J]. Chin J Virol, 2013, 29(6): 608-613. |
| [21] |
Naumova EN, Jagai JS, Matyas B, et al. Seasonality in six enterically transmitted diseases and ambient temperature[J]. Epidemiol Infect, 2007, 135(2): 281-292. DOI:10.1017/S0950268806006698 |
| [22] |
Nguyen GT, Phan K, Teng I, et al. A systematic review and Meta-analysis of the prevalence of Norovirus in cases of gastroenteritis in developing countries[J]. Medicine, 2017, 96(40): e8139. DOI:10.1097/MD.0000000000008139 |
| [23] |
Patel MM, Widdowson MA, Glass RI, et al. Systematic literature review of role of Noroviruses in sporadic gastroenteritis[J]. Emerg Infect Dis, 2008, 14(8): 1224-1231. DOI:10.3201/eid1408.071114 |
| [24] |
Tang MB, Chen CH, Chen SC, et al. Epidemiological and molecular analysis of human Norovirus infections in Taiwan during 2011 and 2012[J]. BMC Infect Dis, 2013, 13: 338. DOI:10.1186/1471-2334-13-338 |