 2019, Vol. 40
2019, Vol. 40文章信息
- 夏云婷, 闫慧敏, 王丽敏, 刘少博, 徐婷玲, 申涛, 张梅, 张笑, 李纯, 黄正京, 赵振平, 李剑虹.
- Xia Yunting, Yan Huimin, Wang Limin, Liu Shaobo, Xu Tingling, Shen Tao, Zhang Mei, Zhang Xiao, Li Chun, Huang Zhengjing, Zhao Zhenping, Li Jianhong.
- 2013年中国18岁及以上超重肥胖患者采取体重控制措施情况及影响因素分析
- A study regarding the control attempts on body weight and related factors among overweight and obese adults in China, 2013
- 中华流行病学杂志, 2019, 40(6): 621-626
- Chinese journal of Epidemiology, 2019, 40(6): 621-626
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.06.004
-
文章历史
收稿日期: 2018-11-12




2. 中国疾病预防控制中心中国现场流行病学培训项目, 北京 100050;
3. 中国疾病预防控制中心慢性非传染性疾病预防控制中心危险因素监测室, 北京 100050;
4. 中国疾病预防控制中心慢性非传染性疾病预防控制中心肥胖与代谢病防控室, 北京 100050
2. Chinese Field Epidemiology Training Program, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
3. Division of Non-communicable Disease Risk Factor Surveillance, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
4. Division of Obesity and Metabolic Diseases Control and Prevention, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
近年来,超重肥胖率在全球范围呈持续上升趋势[1],超重肥胖已成为全球关注的重大公共卫生问题[2]。超重和肥胖是多种慢性病的主要危险因素[3],相比于正常体重者,超重肥胖患者面临更大的患病风险。控制和降低超重肥胖患者的体重可以降低慢性病的发生[4],是提高全民健康水平的关键措施。由于体重控制工作具有长期性和渐进性[5],增加了社区干预的难度,所以超重肥胖患者体重的自我控制尤为重要。本研究利用2013年中国慢性病及其危险因素监测数据,分析比较超重肥胖患者采取体重控制措施情况及其影响因素,为制订超重肥胖患者干预策略提供依据。
对象与方法1.研究对象:2013年中国慢性病及其危险因素监测采用多阶段分层整群随机抽样方法[6],在中国31个省份的302个监测点,调查了≥18岁居民共计179 570人,经数据清理去除了抽样设计具有独立性的新疆生产建设兵团的4个监测点和1个数据质量较差的监测点,最终纳入297个监测点数据进行分析。以超重肥胖患者作为研究对象,剔除关键信息缺失者152人,最终对87 545名调查对象资料进行分析。本研究通过中国CDC慢性非传染性疾病预防控制中心伦理审查委员会的审查(审批号:201307),所有调查对象均签署了知情同意书。
2.调查内容:包括问卷调查、体格检查和实验室检测。问卷调查由经过统一培训的调查员以面对面询问的方式进行调查,内容包括个人基本信息、体重控制措施、主要慢性病(高血压、糖尿病、血脂异常)患病等情况。体格检查包括身高、体重、腰围和血压。实验室检测包括FPG、餐后2 h血糖(OGTT-2 h)、TC、LDL-C、HDL-C和TG[6]。
3.分析指标及定义:①超重肥胖[3]:BMI(kg/m2)=体重(kg)/身高(m)2,以24.0~27.9 kg/m2为超重,≥28.0 kg/m2为肥胖。②中心性肥胖:男性腰围≥85 cm,女性腰围≥80 cm。③采取体重措施控制率:报告12个月内采取体重控制措施的人数占全部研究对象的比例。④高血压:SBP≥140 mmHg(1 mmHg=0.133 kPa)和(或)DBP≥90 mmHg者,或已被乡镇(社区)级或以上医院确诊为高血压且近2周服药者。⑤糖尿病:FPG≥7.0 mmol/L或OGTT-2 h≥11.1 mmol/L,或已被乡镇(社区)级或以上医院确诊为糖尿病。⑥血脂异常:TG≥2.26 mmol/L,或TC≥6.22 mmol/L,或HDL-C<1.04 mmol/L,或LDL-C≥4.14 mmol/L,或已被乡镇(社区)级或以上医院诊断为血脂异常。
4.统计学分析:采用SAS 9.4软件完成所有数据清理和分析,结果均采用复杂加权方法进行调整[6]。使用Survey means过程计算不同特征患者的构成比、采取体重控制措施率及其95%CI。加权率的比较采用Rao-Scott χ2检验,趋势性检验采用基于复杂抽样logistic回归系数的假设检验。采用Survey logistic过程对采取体重控制措施率进行多因素分析。以双侧检验P<0.05为差异有统计学意义。
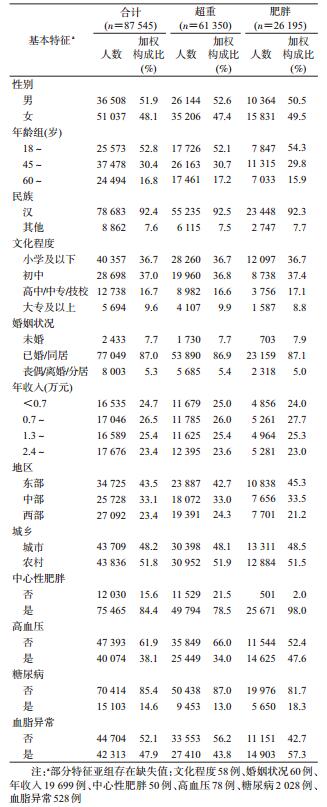
结果1.一般情况:超重肥胖患者有效样本87 545例,加权后男性占51.9%,女性占48.1%;18~岁组占52.8%,具有初中文化程度者占比最高(37.0%);城市占48.2%,农村占51.8%;东、中、西部所占比例依次为43.5%、33.1%和23.4%。超重者占69.7%,中心性肥胖者占84.4%,高血压患者占38.1%,糖尿病患者占14.6%,血脂异常者占47.9%。见表 1。
2.采取体重控制措施情况:我国≥18岁超重肥胖患者采取体重控制措施率16.3%(95%CI:14.9%~17.7%)。男性高于女性,汉族高于其他民族,未婚高于已婚/同居和丧偶/离婚/分居者,城市高于农村;肥胖、中心性肥胖和血脂异常患者高于未患有该疾病者,未患高血压者高于高血压患者,各亚组内差异均有统计学意义(P<0.05)。采取体重控制措施率随年龄降低、文化程度升高、收入水平增加而升高,趋势性检验均有统计学意义(P<0.05)。见表 2。

在所有采取体重控制措施的患者中,不同控制措施构成比例由高到低依次为:饮食(40.9%,95%CI:38.4%~43.3%)、饮食运动组合(31.5%,95%CI:28.9%~34.0%)、运动(22.8%,95%CI:21.0%~24.6%)、药物(1.3%,95%CI:1.0%~1.7%)和其他(3.5%,95%CI:2.9%~4.2%)。饮食运动组合控制比例城市高于农村,且随年龄增加、文化程度升高、收入水平增加而升高,趋势性检验均有统计学意义(P<0.05)。药物控制比例女性显著高于男性,农村显著高于城市,随文化水平升高而呈下降趋势(P<0.05)。见表 2。
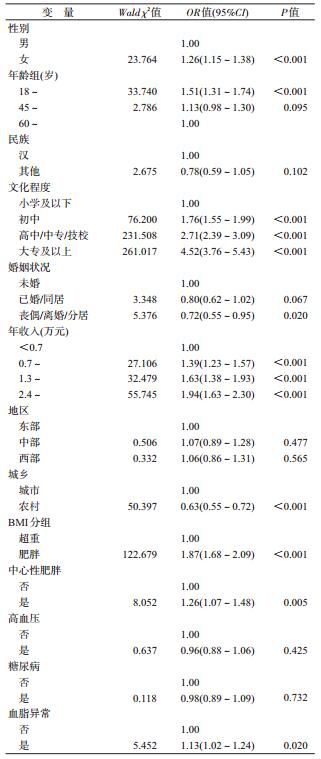
3.采取体重控制措施率多因素分析:复杂抽样设计的logistic回归模型结果显示,有利于采取体重控制措施的因素有女性、低年龄、较高文化程度、较高年收入、肥胖、中心性肥胖和血脂异常;不利于采取控制措施的因素有丧偶/离婚/分居和农村。见表 3。
超重肥胖是高血压、糖尿病、心脑血管疾病等慢性病的独立危险因素,维持健康体重是防控慢性病的关键措施。本研究结果显示,我国≥18岁超重肥胖患者采取体重控制措施率仅为16.3%。Santos等[7]对世界范围内72项研究的Meta分析结果显示,41.5%的普通成年人试图控制体重,其中有23%每年都进行体重控制。我国超重肥胖人群的采取体重控制措施率低,在一定程度上反映出该人群减重的意愿不强,其原因可能是对自身体重的感知不正确[8-10],而体重的感知直接影响减肥等体重控制行为[11]。对超重肥胖的危害认识不足[12]、不知道正确的体重控制方法等也可能是影响不进行体重控制行为的原因。
本研究结果显示,在实施体重控制的患者中,单纯饮食控制者比例最高,占40.9%,饮食运动相结合者占31.5%,单纯运动者占22.8%,药物控制者占1.3%。国内外相关指南均指出,限制热量摄入和定期锻炼相结合是保持健康体重的关键[3, 13-14]。研究也表明,多种控制措施同时使用的减重效果要优于单一措施[15],饮食和体育活动相结合在改善患者健康结果方面优于饮食或单独体育活动[16]。同时,3~6个月(短期)内,单纯控制饮食与饮食运动结合的减肥效果差异无统计学意义,但控制时间达到12~18个月(长期)时,饮食和运动结合的减肥效果会增加[17]。药物治疗仅适用于因肥胖而致疾病危险性增加的患者,对一般的超重肥胖患者,不提倡使用药物减肥[3]。美国内分泌学会(TES)发布的《肥胖药物治疗临床指南》指出[18],食品药品监督管理局(FDA)共批准了6种药物用于治疗肥胖,其使用条件均为BMI≥27 kg/m2,且有≥1项体重相关合并症(如糖尿病、高血压),或BMI≥30 kg/m2。本研究显示,我国超重肥胖患者中,女性、社会经济水平和文化程度低的患者采取药物控制措施比例相对较高。这可能与女性更注重形体有关,而社会经济水平和文化程度较低人群的健康意识也相对较低。
促进超重肥胖患者体重控制行为、提高正确的体重控制观念和技能是维持健康体重、预防相关慢性病的关键环节,也最符合成本效益。相关专业机构应加强对人群维持健康体重的宣传教育,积极创建支持性环境,如在工作场所、公共场所、医疗机构创建健康小屋,提供体重和体成分测量仪器、健身器材、膳食宝塔等;同时对超重肥胖人群开展体重控制技能指导,促进重点人群体重控制行为,从而提升体重控制效果。
本研究发现,城市人群采取体重控制措施率高于农村人群,且随着文化程度、收入水平的提高而升高,可能与文化程度和社会经济地位较高的人群,其健康素养、健康意识也较高有关。同时,肥胖者、中心性肥胖者、血脂异常者的采取体重控制措施率分别高于超重者、非中心性肥胖者和血脂正常者,提示专业机构应针对不同特征群体,开展针对性干预措施。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
WHO. Obesity and overweight. Fact sheet: World Health Organization, 2017[DB/OL]. (2018-01-16)[2018-08-15]. http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight.
|
| [2] |
Hruby A, Hu FB. The epidemiology of obesity:a big picture[J]. Pharmacoeconomics, 2015, 33(7): 673-689. DOI:10.1007/s40273-014-0243-x |
| [3] |
陈春明, 孔灵芝. 中国成人超重和肥胖症预防控制指南[M]. 北京: 人民卫生出版社, 2006. Chen CM, Kong LZ. The guideline for prevention and control of overweight and obesity in Chinese adults[M]. Beijing: People's Medical Publishing House, 2006. |
| [4] |
US Preventive Services Task Force. Behavioral weight loss interventions to prevent obesity-related morbidity and mortality in adults:US preventive services task force recommendation statement[J]. JAMA, 2018, 320(11): 1163-1171. DOI:10.1001/jama.2018.13022 |
| [5] |
杨正雄, 王卉呈, 冯雅靖, 等. 社区超重与肥胖人群体重管理效果的研究[J]. 中华健康管理学杂志, 2010, 4(3): 149-152. Yang ZX, Wang HC, Feng YJ, et al. Effect of body weight management on community residents with over-weight or obesity[J]. Chin J Health Manag, 2010, 4(3): 149-152. DOI:10.3760/cma.j.issn.1674-0815.2010.03.008 |
| [6] |
中国疾病预防控制中心, 中国疾病预防控制中心慢性非传染性疾病预防控制中心. 中国慢性病及其危险因素监测报告(2013)[M]. 北京: 军事医学科学出版社, 2016. National Center for Chronic and Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention. Report on chronic disease risk factor surveillance in China (2013)[M]. Beijing: Military Medical Science Press, 2016. |
| [7] |
Santos I, Sniehotta FF, Marques MM, et al. Prevalence of personal weight control attempts in adults:a systematic review and Meta-analysis[J]. Obes Rev, 2017, 18(1): 32-50. DOI:10.1111/obr.12466 |
| [8] |
Duncan DT, Wolin KY, Scharoun-Lee M, et al. Does perception equal reality? Weight misperception in relation to weight-related attitudes and behaviors among overweight and obese US adults[J]. Int J Behav Nutr Phys Act, 2011, 8: 20. DOI:10.1186/1479-5868-8-20 |
| [9] |
Bhanji S, Khuwaja AK, Siddiqui F, et al. Underestimation of weight and its associated factors among overweight and obese adults in Pakistan:a cross sectional study[J]. BMC Public Health, 2011, 11: 363. DOI:10.1186/1471-2458-11-363 |
| [10] |
姜勇, 张梅, 李镒冲, 等. 2010年我国成人体重自测及体重知晓情况分析[J]. 中国健康教育, 2013, 29(6): 485-488. Jiang Y, Zhang M, Li YC, et al. Investigation on self-measurement and awareness of body weight among Chinese adults in 2010[J]. Chin J Health Educat, 2013, 29(6): 485-488. |
| [11] |
Yost J, Krainovich-Miller B, Budin W, et al. Assessing weight perception accuracy to promote weight loss among U.S. female adolescents:a secondary analysis[J]. BMC Public Health, 2010, 10: 465. DOI:10.1186/1471-2458-10-465 |
| [12] |
Haynes A, Kersbergen I, Sutin A, et al. A systematic review of the relationship between weight status perceptions and weight loss attempts, strategies, behaviours and outcomes[J]. Obes Rev, 2018, 19(3): 347-363. DOI:10.1111/obr.12634 |
| [13] |
Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults:a report of the American college of cardiology/American heart association task force on practice guidelines and the obesity society[J]. Circulation, 2014, 129(25 Suppl 2): S102-138. DOI:10.1161/01.cir.0000437739.71477.ee |
| [14] |
中国营养学会. 中国居民膳食指南(2016)[M]. 北京: 人民卫生出版社, 2016. Chinese Society of Nutrition. The Dietary Guidelines for Chinese Residents (2016)[M]. Beijing: People's Medical Publishing House, 2016. |
| [15] |
Kang LL, Kim HN, Jung YA, et al. The effects of weight control behaviors among Korean obese adults[J]. Korean J Fam Med, 2018, 39(4): 247-252. DOI:10.4082/kjfm.17.0021 |
| [16] |
Elliot CA, Hamlin MJ. Combined diet and physical activity is better than diet or physical activity alone at improving health outcomes for patients in New Zealand's primary care intervention[J]. BMC Public Health, 2018, 18: 230. DOI:10.1186/s12889-018-5152-z |
| [17] |
Johns DJ, Hartmann BJ, Jebb SA, et al. Diet or exercise interventions vs combined behavioral weight management programs:a systematic review and Meta-analysis of direct comparisons[J]. J Acad Nutr Diet, 2014, 114(10): 1557-1568. DOI:10.1016/j.jand.2014.07.005 |
| [18] |
Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacological management of obesity:an endocrine society clinical practice guideline[J]. J Clin Endocrinol Metab, 2015, 100(2): 342-362. DOI:10.1210/jc.2014-3415 |