 2019, Vol. 40
2019, Vol. 40文章信息
- 李若曈, 宁佩珊, 李婕, 王万慧, 胡国清.
- Li Ruotong, Ning Peishan, Li Jie, Wang Wanhui, Hu Guoqing.
- 干预图方法研究进展
- Review on the progress regarding the intervention mapping protocol
- 中华流行病学杂志, 2019, 40(4): 488-492
- Chinese journal of Epidemiology, 2019, 40(4): 488-492
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.04.022
-
文章历史
收稿日期: 2018-12-20




健康促进干预通过强调疾病预防问题、促进健康生活方式、提高患者依从性和医疗服务可及性,帮助控制或降低整体医疗保健成本,实现改善个体的身体、心理、教育和工作状况的目的[1]。近几十年来,随着健康促进理论和实践研究的快速发展,社会行为科学理论被越来越多地用于设计健康干预措施,并取得了良好效果[2-3]。健康干预是健康促进的重要组成部分,也是一项复杂的健康行为改变技术[4]。Nation等[5]系统评估既往干预研究文献后发现,有效的干预方案应以干预理论为基础。然而,既往干预中有相当一部分缺乏理论支持,干预设计和效果评估中均缺乏理论基础[6-7]。为解决上述问题,20世纪90年代Bartholomew等[8]提出干预图方法(Intervention Mapping,IM)。这种方法为基于理论和研究证据设计最佳干预措施提供了参考,已在多个国家被应用于肥胖、吸烟、身体活动和癌症等问题干预研究[9]。鉴于国内学者和公共卫生工作人员对此种方法尚不熟悉,本文简要介绍干预图方法的基本概念、步骤、实施要求以及目前此方法研究及应用进展。
二、基本概念IM是以理论和证据为基础,采取社会生态学的方式来评估健康需求、干预健康问题并促进社区参与的健康促进规划方法[10]。具有的特点[11]:①将行为视作个体及个体生存的物质、社会和组织环境的功能;②将所有利益相关者都纳入研究过程;③运用理论和实证。
三、实施步骤及具体要求IM由6个步骤构成:评估健康问题和社区能力;确定项目目标;选择基于理论的干预策略和应用;设计和调整项目;完善和实施项目;实施评价(图 1)。

|
| 图 1 标准干预图方法实施流程 |
IM的每一步均由若干任务组成,前后关联,所有步骤构成了设计、实施和评估干预项目的基本框架。下文以设计医护人员接种流感疫苗干预为例[12]介绍IM的6个步骤和相关任务。
第一步:进行需求分析。研究人员首先对健康问题进行评估,寻找其环境、行为原因和决定因素,了解社区特征并探寻解决措施。流感是导致老年人死亡和住院的主要原因之一[13],而流感疫苗是流感的最有效预防措施。研究显示,给医护人员接种流感疫苗可以预防流感,减少传播和降低医护人员的疾病缺勤率[14-17]。但美国、新西兰等国医护人员流感疫苗覆盖率远低于预期。基于以上证据,Kok等[12]开展生态学分析,确定IM过程中的目标人群为医护人员,相关的环境条件是医院、养老院和卫生保健政策。
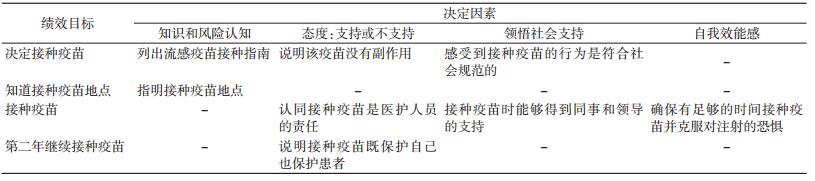
第二步:确定项目目标。研究人员基于对健康问题和相关因素的生态学分析,定义项目的绩效目标(风险人群特定期望行为或环境因素的特定期望情况)和改变目标(决定因素的变化)。该例中为了减少流感问题,预期目标是医护人员每年定期接种流感疫苗。Kok等[12]归纳了流感干预相关行为、环境因素和决定因素,构建目标矩阵(表 1)。
第三步:理论方法转化为实际干预策略。即基于理论和方法设计适应目标人群和相应背景的具体干预策略。如van den Akker等[18]针对不同类型的决定因素,采用相应的干预策略。如针对提高意识,采用会议、传单和海报等实际干预策略;针对改变态度,采用解释说明,小组讨论和放映视频等;针对社会支持,采用寄送邀请卡片等。
第四步:调整初始干预方案,确定最终方案。IM的第四步中,根据上一步选择的干预策略,确定干预计划的主题、结构、方式和载体;结合文化背景,设计制作相关材料;进行预实验并调整,确定最终方案。Llupià等[19]报告了其干预设计方案:①机构支持,医院管理部门承诺接种疫苗。②基于网络,通过电子邮件推送每周的健康教育信息。③可及性,设置疫苗接种移动点,并提供电话咨询。
第五步:完善方案,执行方案。确定潜在的采纳者和实施者,重新评估绩效目标,采纳主要影响因素,设计实际的干预措施,形成执行方案。该例在医院或养老院内实施干预,一般由该院主管医护人员职业卫生相关科室实施,并得到管理层和传染科医生的支持。
第六步:制定用于效果评估和过程评估的计划。确定评价模型、评价指标、设计类型、过程评价问题和效果评价问题,形成评价方案。Riphagen-Dalhuisen等[20]编制相关量表来定量评估执行结果,并构建干预点联络员焦点小组,收集对干预方法和资料意见,用于定性评价干预效果。
四、研究进展 (一) 应用情况1.妇幼健康促进:
(1)儿童肥胖防治:儿童肥胖是21世纪全球公共卫生挑战之一。预防儿童肥胖已引起广泛关注[21]。Pittson和Wallace[22]对英国超重和肥胖儿童家庭进行体重控制干预,根据IM构建的6个步骤,基于行为的决定因素制定项目目标,选取相应干预策略,并评价效果。结果显示,儿童平均BMI指数由(28.48±4.44)kg/m2,下降至(27.48±4.45)kg/m2,P<0.001。
Taylor等[23]选取英国多种族社区的肥胖、超重孕妇,采用IM进行母婴多水平干预,填补了生命早期儿童肥胖干预项目的空白。研究人员认为尽管使用IM模式开发大规模的干预项目是一个耗时的过程,但IM能针对复杂的健康行为,在设计干预计划时有理可循,帮助有效建立干预方案。
de Lepeleere等[24]采用在线视频的方式对儿童饮食相关养育方式、身体活动和父母的自我效能进行干预。该项目中,IM用于构造干预开发过程框架,IM第六步评价结果证实该干预有效促进积极的养育方式[25],也肯定了IM对于推进健康促进项目的作用。
(2)普及性健康和生殖健康保健:性健康教育和生殖保健规划经常在不同文化背景、研究对象和环境中实施。IM能够帮助识别和保留与项目有效性密切相关的核心元素,并进行适当的调整,提高新的研究对象的接受度[26]。
美国的一项将证实有效的生殖健康干预应用于高危少数民族青少年研究中,利用IM筛选出了该群体中新的决定因素,并确定相应的有效干预[27]。Peskin等[28]的研究中,利用IM中的第三、四步,开发了学校性教育项目iCHAMPSS,帮助学校建立和维持在线决策支持的性健康干预系统,可能有利于推进性健康干预项目在学校的广泛实施。
2.慢性病管理:
(1)癌症:2014年世界癌症报告显示[29],每年有620万人因患恶性肿瘤死亡,早期发现癌症对有效治疗和治愈癌症至关重要[30]。子宫颈癌是女性生殖道发病率和死亡率最高的恶性肿瘤,近年来,进行早期筛检和健康教育成为了防治子宫颈癌的重点。Byrd等[31]对墨西哥裔美国女性宫颈癌筛查的干预中,通过IM确定和细化宫颈癌筛查的优先领域。Hou等[32]在提高中国台湾地区女性乳腺癌和子宫颈癌筛查率的研究中,基于IM的干预有效地提高了乳房造影筛查(P=0.002)和子宫颈涂片检查率(P=0.031)。Scarinci等[33]研究中,基于健康信念模型,采用IM开发了一级预防(性风险降低)和二级预防(子宫颈涂片)宫颈癌项目,促进了一项新的干预措施的发展。此外,McEwen等[34]在IM的指导下,在目标设定和自我管理的理论基础上,开发了头颈癌幸存者康复咨询。
(2)中风:由于人口老龄化导致中风高发病率[35]和风险因素控制不佳导致的高复发率[36],突出了发展中风干预策略的重要性。一项对中风患者进行生活方式干预研究中[37],研究者应用IM基于理论、实验证据和临床经验,来设计、实施和评估实际干预措施,这在此前中风的二级预防干预项目中较为缺乏。
3.传染病防控:
艾滋病是一种危害性极大的传染病[38],艾滋病疫情的蔓延是一大公共卫生威胁。目前,IM已被应用于艾滋病干预计划的设计中,如:荷兰移民男性艾滋病预防项目[39]、降低荷兰吸毒人员艾滋病风险干预项目[40],美国高危人群艾滋病、性传播感染和怀孕预防项目等[22],IM能够系统地根据相应的文化背景来开发新的干预措施适应新的人群[22]。Corbie-Smith等[41]在美国偏远非洲裔黑人社区的艾滋病干预项目中利用IM能有效整合到社区参与式研究(Community Based Participatory Research,CBPR)过程的优点,帮助研究人员开发新的可接受方式来提高护理人员参与度,帮助减少青少年的性风险行为。
(二) 局限性和未来发展方向IM作为一种实用的健康促进规划工具,实际应用过程中也被发现存在一些不足。IM复杂的过程耗费研究人员大量的时间、精力和经济投入,所以在使用IM时需结合具体问题优化方法来提高效率[42]。此外,IM流程化的模式使得不能提前给出最终干预方案,在实施和评估时可能会影响工作经费的获取[32]。尽管如此,IM仍被认为优势大于劣势,其在提升干预质量中的作用得到了充分的肯定[43-44]。
目前,IM主要应用于各种健康行为,如饮食、身体活动和性行为等的干预,但IM不仅可用于健康领域,也可用于其他领域的行为改变,如节约能源、城市重建以及科学教育。IM应用研究首先开始于欧洲和北美,但其使用范围不断扩大,迄今为止已在46个国家得到应用[8]。
五、对我国健康促进的启示目前发表的研究仍以在欧洲地区和北美地区进行的为主,国内在应用IM开展干预项目研究的数量非常少[45-47]。
《“健康中国2030”规划纲要》[48]明确提出了“共建共享、全民健康”的建设健康中国的战略主题,未来5~10年,中国健康促进与教育事业发展将进入重要的战略机遇期[49]。干预图作为一项实用的健康促进规划工具,无疑对提高我国健康干预研究的质量大有裨益。建议国内公共卫生学者及实践者可利用干预图这一有效工具加强健康促进理论对干预的指导作用,建立概念清晰的健康促进模型,开展符合国情的健康干预,进一步提升我国的健康干预的研究水平及执行效果。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
Fertman CI, Allensworth DD. Health promotion programs:from theory to practice[M]. San Francisco: Jossey-Bass, 2010.
|
| [2] |
Glanz K, Lewis FM, Rimer BK. Health behavior and health education:theory, research, and practice[M]. San Francisco: Jossey-Bass, 1997.
|
| [3] |
Maibach E, Parrot RL. Designing health messages:approaches from communication theory and public health practice[M]. Thousand Oaks: SAGE Publication, 1995.
|
| [4] |
Hagger MS, Luszczynska A. Implementation intention and action planning interventions in health contexts:state of the research and proposals for the way forward[J]. Appl Psychol:Health Well-Being, 2014, 6(1): 1-47. DOI:10.1111/aphw.12017 |
| [5] |
Nation M, Crusto C, Wandersman A, et al. What works in prevention:Principles of effective prevention programs[J]. Am Psychol, 2003, 58(6/7): 449-456. DOI:10.1037/0003-066X.58.6-7.449 |
| [6] |
Davies P, Walker AE, Grimshaw JM. A systematic review of the use of theory in the design of guideline dissemination and implementation strategies and interpretation of the results of rigorous evaluations[J]. Implement Sci, 2010, 5(1): 14. DOI:10.1186/1748-5908-5-14 |
| [7] |
Molloy GJ. Increasing influenza vaccination rates:where is the behaviour change theory?[J]. Vaccine, 2010, 28(21): 3632. DOI:10.1016/j.vaccine.2010.03.036 |
| [8] |
Bartholomew LK, Parcel GS, Kok G. Intervention mapping:a process for developing theory-and evidence-based health education programs[J]. Health Educ Behav, 1998, 25(5): 545-563. DOI:10.1177/109019819802500502 |
| [9] |
Fassier JB, Lamort-Bouché M, Sarnin P, et al. The intervention mapping protocol:A structured process to develop, implement and evaluate health promotion programs[J]. Revue d'épidémiol Santé Publiq, 2016, 64(1): 33-44. DOI:10.1016/j.respe.2015.10.002 |
| [10] |
Bartholomew LK, Parcel GS, Kok G, et al. Planning health promotion programs:an intervention mapping approach[M]. San Francisco: Jossy-Bass, 2011.
|
| [11] |
Kok G, Peters LWH, Ruiter RAC. Planning theory-and evidence-based behavior change interventions:a conceptual review of the intervention mapping protocol[J]. Psicol:Reflex Crít, 2017, 30(1): 19. DOI:10.1186/s41155-017-0072-x |
| [12] |
Kok G, van Essen GA, Wicker S, et al. Planning for influenza vaccination in health care workers:an intervention mapping approach[J]. Vaccine, 2011, 29(47): 8512-8519. DOI:10.1016/j.vaccine.2011.09.008 |
| [13] |
Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory syncytial virus in the United States[J]. JAMA, 2003, 289: 179-186. DOI:10.1001/jama.289.2.179 |
| [14] |
Hayward AC, Harling R, Wetten S, et al. Effectiveness of an influenza vaccine programme for care home staff to prevent death, morbidity, and health service use among residents:cluster randomised controlled trial[J]. BMJ, 2006, 333(7581): 1241-1244. DOI:10.1136/bmj.39010.581354.55 |
| [15] |
Fiore AE, Uyeki TM, Broder K, et al. Prevention and control of influenza with vaccines:recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010[J]. Mmwr Recomm Rep, 2010, 59(RR-8): 1-62. |
| [16] |
Nichol KL, Lind A, Margolis KL, et al. The effectiveness of vaccination against influenza in healthy, working adults[J]. N Engl J Med, 1995, 333(14): 889-893. DOI:10.1056/NEJM199510053331401 |
| [17] |
Nichol KL, D'Heilly SJD, Greenburg ME, et al. Burden of influenza-like illness and effectiveness of influenza vaccination among working adults aged 50-64 years[J]. Clin Infect Dis, 2009, 48(3): 292-298. DOI:10.1086/595842 |
| [18] |
van den Akker L, Hulscher ME, Verheij TJM, et al. How to develop a program to increase influenza vaccine uptake among workers in health care settings?[J]. Implement Sci, 2011, 6(1): 47. DOI:10.1186/1748-5908-6-47 |
| [19] |
Llupià A, García-Basteiro AL, Olivé V, et al. New interventions to increase influenza vaccination rates in health care workers[J]. Am J Inf Control, 2010, 38(6): 476-481. DOI:10.1016/j.ajic.2010.01.013 |
| [20] |
Riphagen-Dalhuisen J, Frijstein G, van der Geest-Blankert N, et al. Planning and process evaluation of a multi-faceted influenza vaccination implementation strategy for health care workers in acute health care settings[J]. BMC Inf Dis, 2013, 13(1): 235. DOI:10.1186/1471-2334-13-235 |
| [21] |
World Health Organization, UNICEF. Final report of the commission on ending childhood obesity[R]. Geneva: World Health Organization, 2016.
|
| [22] |
Pittson H, Wallace L. Using intervention mapping to develop a family-based childhood weight management programme[J]. J Health Serv Res Policy, 2011(Suppl 1): 2-7. DOI:10.1258/jhsrp.2010.010076 |
| [23] |
Taylor NJ, Sahota P, Sargent J, et al. Using intervention mapping to develop a culturally appropriate intervention to prevent childhood obesity:the HAPPY (Healthy and Active Parenting Programme for Early Years) study[J]. Int J Behav Nut Phys Act, 2013, 10(1): 142. DOI:10.1186/1479-5868-10-142 |
| [24] |
de Lepeleere S, Verloigne M, Brown HE, et al. Using the Intervention Mapping Protocol to develop an online video intervention for parents to prevent childhood obesity:Movie Models[J]. Glob Health Promot, 2018, 25(2): 56-66. DOI:10.1177/1757975916658603 |
| [25] |
de Lepeleere S, de Bourdeaudhuij I, Cardon G, et al. The effect of an online video intervention 'Movie Models' on specific parenting practices and parental self-efficacy related to children's physical activity, screen-time and healthy diet:a quasi experimental study[J]. BMC Public Health, 2017, 17: 366. DOI:10.1186/s12889-017-4264-1 |
| [26] |
Leerlooijer JN, Ruiter RAC, Reinders J, et al. The world starts with me:using intervention mapping for the systematic adaptation and transfer of school-based sexuality education from Uganda to Indonesia[J]. Trans Behav Med, 2011, 1(2): 331-340. DOI:10.1007/s13142-011-0041-3 |
| [27] |
Tortolero SR, Markham CM, Parcel GS, et al. Using intervention mapping to adapt an effective HIV, sexually transmitted disease, and pregnancy prevention program for high-risk minority youth[J]. Health Promot Pract, 2005, 6(3): 286-298. DOI:10.1177/1524839904266472 |
| [28] |
Peskin MF, Hernandez BF, Gabay EK, et al. Using intervention mapping for program design and production of iCHAMPSS:an online decision support system to increase adoption, implementation, and maintenance of evidence-based sexual health programs[J]. Front Public Health, 2017, 5: 203. DOI:10.3389/fpubh.2017.00203 |
| [29] |
World Health Organization, UNICEF. World cancer report 2014[R]. Geneva, World Health Organization, 2015.
|
| [30] |
Wulfkuhle JD, Liotta LA, Petricoin EF. Proteomic applications for the early detection of cancer[J]. Nat Rev Cancer, 2003, 3(4): 267. DOI:10.1038/nrc1043 |
| [31] |
Byrd TL, Wilson KM, Smith JL, et al. Using intervention mapping as a participatory strategy:development of a cervical cancer screening intervention for Hispanic women[J]. Health Educat Behav, 2012, 39(5): 603-611. DOI:10.1177/1090198111426452 |
| [32] |
Hou SI, Fernandez ME, Parcel GS. Development of a cervical cancer educational program for Chinese women using intervention mapping[J]. Health Promot Pract, 2004, 5(1): 80-87. DOI:10.1177/1524839903257311 |
| [33] |
Scarinci IC, Bandura L, Hidalgo B, et al. Development of a theory-based (PEN-3 and health belief model), culturally relevant intervention on cervical cancer prevention among Latina immigrants using intervention mapping[J]. Health Promot Pract, 2012, 13(1): 29-40. DOI:10.1177/1524839910366416 |
| [34] |
McEwen SE, Davis AM, Jones JM, et al. Development and preliminary evaluation of a rehabilitation consult for survivors of head and neck cancer:an intervention mapping protocol[J]. Implement Sci, 2015, 10: 6. DOI:10.1186/s13012-014-0191-z |
| [35] |
Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. Global and regional burden of stroke during 1990-2010:findings from the Global Burden of Disease Study 2010[J]. Lancet, 2014, 383(9913): 245-255. DOI:10.1016/S0140-6736(13)61953-4 |
| [36] |
Heuschmann PU, Kircher J, Nowe T, et al. Control of main risk factors after ischaemic stroke across Europe:data from the stroke-specific module of the EUROASPIRE Ⅲ survey[J]. Eur J Prev Cardiol, 2015, 22(10): 1354-1362. DOI:10.1177/2047487314546825 |
| [37] |
Sakakibara BM, Lear SA, Barr SI, et al. Development of a chronic disease management program for stroke survivors using intervention mapping:the stroke coach[J]. Arch Phys Med Rehab, 2017, 98(6): 1195-1202. DOI:10.1016/j.apmr.2017.01.019 |
| [38] |
Joint United Nations Programme on HIV/AIDS. Global AIDS update 2016[EB/OL]. (2016-05-31)[2018-10-02]. http://www.unaids.org/en/resources/documents/2016/Global-AIDS-update-2016.
|
| [39] |
Wolfers MEG, van den Hoek C, Brug J, et al. Using Intervention Mapping to develop a programme to prevent sexually transmittable infections, including HIV, among heterosexual migrant men[J]. BMC Public Health, 2007, 7: 141. DOI:10.1186/1471-2458-7-141 |
| [40] |
van Empelen P, Kok G, Schaalma HP, et al. An AIDS risk reduction program for Dutch drug users:an intervention mapping approach to planning[J]. Health Promot Pract, 2003, 4(4): 402-412. DOI:10.1177/1524839903255421 |
| [41] |
Corbie-Smith G, Akers A, Blumenthal C, et al. Intervention mapping as a participatory approach to developing an HIV prevention intervention in rural African American communities[J]. AIDS Educ Prev, 2010, 22(3): 184-202. DOI:10.1521/aeap.2010.22.3.184 |
| [42] |
Garba RM, Gadanya MA. The role of intervention mapping in designing disease prevention interventions:A systematic review of the literature[J]. PLoS One, 2017, 12(3): e0174438. DOI:10.1371/journal.pone.0174438 |
| [43] |
Belansky ES, Cutforth N, Chavez RA, et al. An adapted version of Intervention Mapping (AIM) is a tool for conducting community-based participatory research[J]. Health Promot Pract, 2011, 12(3): 440-455. DOI:10.1177/1524839909334620 |
| [44] |
Aro AR, Absetz P. Guidance for professionals in health promotion:Keeping it simple-but not too simple[J]. Psychol Health, 2009, 24(2): 125-129. DOI:10.1080/08870440802642973 |
| [45] |
汪春华, 黄艳, 臧晓鹭. 干预映射用于老年患者预防跌倒自我管理的效果评价[J]. 护理学杂志, 2017, 32(21): 5-8. Wang CH, Huang Y, Zang XL. Effect of intervention mapping on self-management of fall prevention for elderly patients[J]. J Nurs Sci, 2017, 32(21): 5-8. DOI:10.3870/j.issn.1001-4152.2017.21.005 |
| [46] |
郭新红, 李彦华, 李欣. 基于干预映像协议六步法的住院医师医患沟通技巧培训评估体系的构建[J]. 中国高等医学教育, 2015(1): 20-21. Guo XH, Li YH, Li X. Construction of doctor-patient communication skills training evaluation system in resident doctors using intervention mapping[J]. China Higher Med Educ, 2015(1): 20-21. DOI:10.3969/j.issn.1002-1701.2015.01.011 |
| [47] |
蒋莹, 常春, 王燕玲. 健康促进需求评估模型[J]. 中国公共卫生, 2016, 32(8): 1129-1132. Jiang Y, Chang C, Wang YL. Application of health promotion need assessment model:a review[J]. Chin J Public Health, 2016, 32(8): 1129-1132. DOI:10.11847/zgggws2016-32-08-31 |
| [48] |
国务院印发《"健康中国2030"规划纲要》[EB/OL]. (2017-02-15)[2017-03-17]. http://www.mofCom.gov.cn/article/b/g/201702/20170202516062.shtml. State Council issued the outline for the "Healthy China 2030" plan[EB/OL]. (2017-02-15)[2017-03-17]. http://www.mofcom.gov.cn/article/b/g/201702/20170202516062.shtml. |
| [49] |
李晋芬, 任学锋. 中国健康教育与健康促进的挑战机遇与展望[J]. 中国预防医学杂志, 2018, 19(2): 156-158. Li JF, Ren XF. Challenges and prospects of China's health education and health promotion[J]. Chin Prev Med, 2018, 19(2): 156-158. DOI:10.16506/j.1009-6639.2018.02.018 |