 2019, Vol. 40
2019, Vol. 40文章信息
- 雷园婷, 罗冬梅, 张京舒, 胡佩瑾, 张冰, 宋逸, 马军.
- Lei Yuanting, Luo Dongmei, Zhang Jingshu, Hu Peijin, Zhang Bing, Song Yi, Ma Jun.
- 中国26个少数民族7~18岁学生生长迟缓比较研究
- Comparative study on growth retardation prevalence in students aged 7-18 years from 26 minority ethnic groups in China
- 中华流行病学杂志, 2019, 40(3): 335-340
- Chinese Journal of Epidemiology, 2019, 40(3): 335-340
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.03.015
-
文章历史
收稿日期: 2018-09-07




生长迟缓是一种长期性营养不良的表现[1]。据WHO报告,2016年全球有22.9%(约1.55亿)的5岁以下儿童出现了生长迟缓[2]。生长迟缓不仅表现在儿童身高发育受限,还被认为是影响儿童早期发育的重要因素,但大多数研究仅重点关注5岁以下儿童生长迟缓的情况。学龄儿童生长迟缓不仅影响儿童认知和健康水平,还可能影响其成年期身高,甚至影响后代的发育水平[3-4]。本研究旨在对各少数民族学生身高进行比较研究,分析各少数民族学生成年身高和生长迟缓现况,为促进少数民族学生生长潜力提供依据。
对象与方法1.研究对象:来自2014年“全国学生体质与健康调研”中的少数民族学生,调研沿用“全国学生体质与健康调研”的方法选择样本,具体抽样方案见2014年全国学生体质与健康调研报告[5]。采用分层随机整群抽样法,在各少数民族聚集地选择中、小学校后,按年级分层,随机选择班级,整群抽取1~2个班级全体学生作为调研样本。本研究将26个少数民族7~18岁学生全部纳入分析,其中蒙古族、回族、维吾尔族、壮族、朝鲜族分为城、乡两类进行抽样,其余21个民族(土家族、瑶族、黎族、彝族、羌族、苗族、布依族、侗族、水族、白族、哈尼族、傣族、傈僳族、佤族、纳西族、藏族、东乡族、土族、撒拉族、哈萨克族、柯尔克孜族)不分城乡。选取民族、身高变量完整的数据,共80 795名学生纳入分析,其中男生40 303名(49.9%),女生40 492名(50.1%),见表 1。
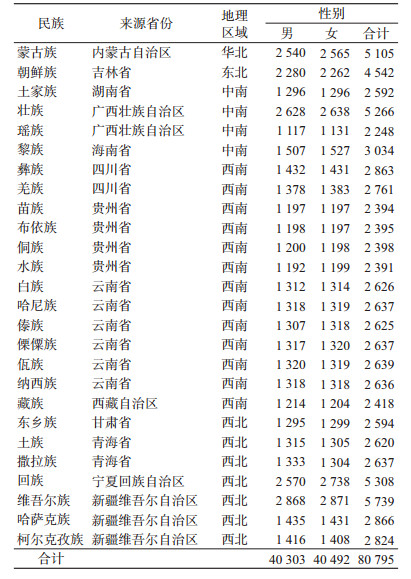
2.研究方法:身高由经培训合格的工作人员采用统一的方法和仪器进行测量,测量方法按“2014年全国学生体质与健康调研实施细则”进行[5]。根据《学龄儿童青少年营养不良筛查标准》(WS/T 456-2014)[1],以身高小于等于性别年龄别身高界值判断为生长迟缓,计算各民族、年龄段学生生长迟缓率。根据中华人民共和国行政区划方式[6],将各少数民族来源省进行区域划分为华北、东北、中南、西南和西北地区(表 1)。
3.统计学分析:均值检验采用t检验,率的检验采用χ2检验或logistic回归,少数民族生长迟缓率与当地人均GDP的关联采用Spearman相关分析,将18岁身高与7~17岁各年龄组学生生长迟缓率进行Spearman相关分析。P<0.05为差异有统计学意义,统计学分析采用SPSS 22.0软件。
结果1.一般情况:2014年我国26个少数民族学生中,18岁男生身高为(168.3±6.8)cm,女生为(156.2±5.9)cm。18岁男生平均身高超过170.0 cm的民族为蒙古族、朝鲜族、白族、纳西族、藏族、东乡族、撒拉族、回族、维吾尔族、哈萨克族和柯尔克孜族。平均身高最高的民族为回族[(174.5±5.5)cm],平均身高最低的为苗族[(162.1±5.3)cm],差异有统计学意义(t=-17.116,P<0.001)。18岁女生平均身高超过160.0 cm的民族为撒拉族和回族,平均身高最高的民族是撒拉族[(160.9±4.9)cm],最低的民族是佤族[(151.1±5.6)cm],差异有统计学意义(t=13.501,P<0.001),见表 2。
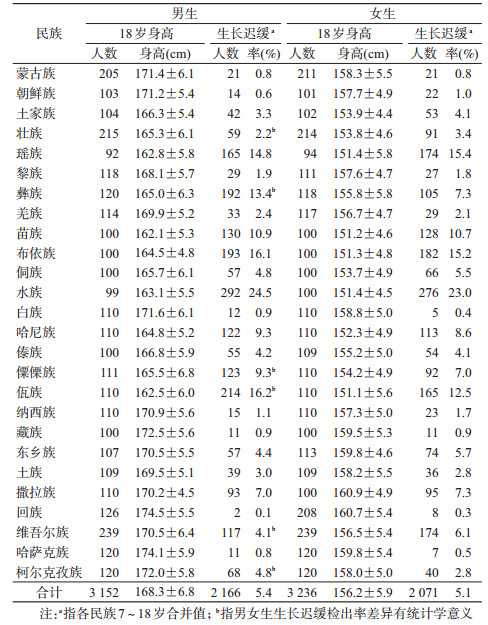
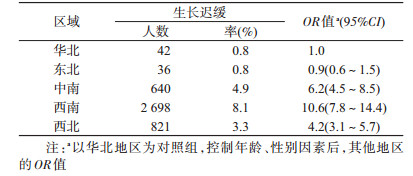
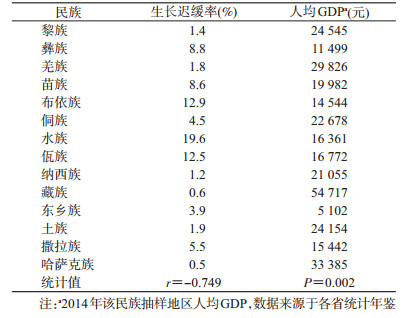
2.生长迟缓情况:2014年26个少数民族学生总体生长迟缓率为5.2%,其中男生为5.4%,女生为5.1%,男、女生之间差异无统计学意义(χ2=2.780,P=0.095)。26个少数民族中,男生生长迟缓率较高的前3个民族分别为水族(24.5%)、佤族(16.2%)和布依族(16.1%);女生生长迟缓率较高的前3个民族分别为水族(23.0%)、瑶族(15.4%)和布依族(15.2%);回族学生生长迟缓率最低(男生:0.1%,女生:0.3%)。彝族、傈僳族、佤族和柯尔克孜族男生生长迟缓率高于女生,壮族和维吾尔族女生生长迟缓率高于男生,其余少数民族学生生长迟缓率在性别上差异无统计学意义(表 2)。按照行政区划分区域后,以华北地区为参照,西南地区学生生长迟缓率较高(8.1%,OR=10.6,95%CI:7.8~14.4),其次为中南地区(4.9%,OR=6.2,95%CI:4.5~8.5)(表 3)。将抽样点仅为1个地区的14个少数民族学生的生长迟缓率与2014年当地人均GDP进行相关分析,结果显示,生长迟缓率与人均GDP呈明显负相关(r=-0.749,P=0.002),见表 4。
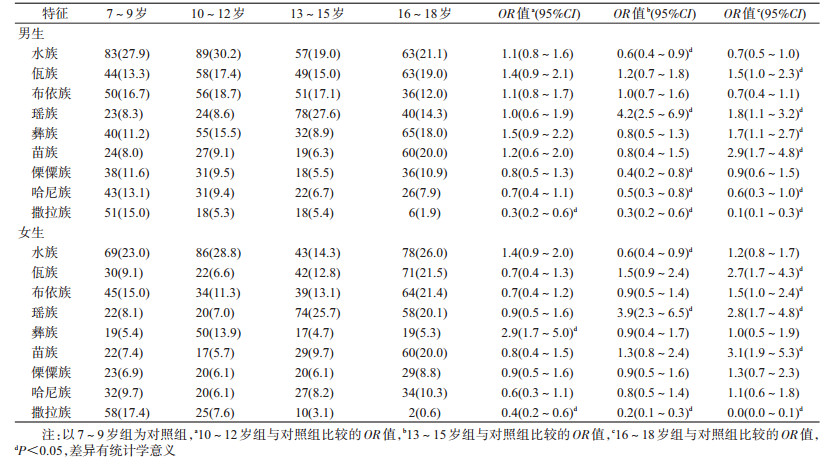
将男、女生生长迟缓率均超过少数民族平均水平的9个少数民族分7~9、10~12、13~15和16~18岁4个年龄组进行比较,以7~9岁组为参照。在男生中,布依族4个年龄组学生生长迟缓检出率差异无统计学意义;水族、傈僳族13~15岁组生长迟缓率最低,哈尼族13~15和16~18岁组生长迟缓率最低;撒拉族生长迟缓检出集中在7~9岁组;瑶族集中在13~15岁组;佤族、彝族和苗族集中在16~18岁组。在女生中,傈僳族、哈尼族4个年龄组学生生长迟缓检出率差异无统计学意义;水族13~15岁组生长迟缓率最低;撒拉族生长迟缓检出集中在7~9岁组,彝族集中在10~12岁组,瑶族集中在13~15和16~18岁组;佤族、布依族、苗族生长迟缓主要集中在16~18岁组,见表 5。
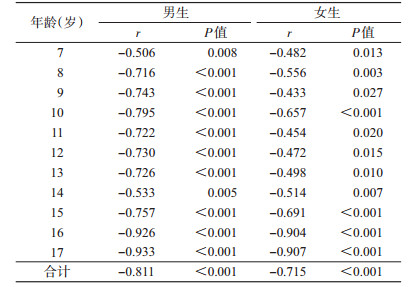
3.生长迟缓与18岁身高的关联:26个少数民族学生18岁平均身高与7~17岁组学生生长迟缓率呈显著负相关(男生:r=-0.811,P<0.001;女生:r=-0.715,P<0.001)。进一步分析结果显示,男、女生各个年龄组生长迟缓率与18岁身高均呈显著负相关,男生生长迟缓率与18岁身高的相关性比女生更强(表 6)。
据2017年《中国卫生和计划生育统计年鉴》报告,2012年我国城市男生18岁平均身高为169.5 cm,女生为159.9 cm;农村男生18岁平均身高为167.9 cm,女生为157.2 cm[7]。本研究中,有12个少数民族男生18岁身高低于2012年农村地区男生身高,有14个少数民族女生18岁身高低于2012年农村女生平均身高。男生以回族身高较高;女生以撒拉族、回族身高较高,佤族、苗族、布依族、侗族、水族身高较矮,与既往研究结果相似[8-9]。本研究结果显示,即使在同一省份,不同少数民族学生18岁身高也表现出了较大差距,例如白族18岁身高明显高于佤族,这一差别可能与遗传、饮食习惯等因素有关,迅猛发展的民族经济和旅游业为儿童营养健康发展提供了有力的经济保障,近年来大理地区白族学生的生长发育水平已与当地汉族相接近[10]。
2010年人口普查数据显示,我国少数民族共有113 792 211人,占我国总人口的8.49%[11],2014年我国26个少数民族生长迟缓率为5.2%,高于2014年我国7~18岁汉族儿童青少年生长迟缓检出率(2.3%)[12]。虽然整体上我国少数民族学生生长迟缓率不高,但我国人口基数大,生长迟缓的人口数量是一个不容忽视的大数字。此外,本研究结果还显示,各民族男、女生生长迟缓检出率比较接近,大部分民族男、女生生长迟缓检出率差异无统计学意义,提示在现阶段,性别因素对少数民族学生生长迟缓影响不明显。在分民族分析后发现,水族学生生长迟缓情况最为突出,男、女生检出率均>20.0%,佤族、布依族、瑶族和苗族生长迟缓率也均>10.0%,因此这些民族应该是未来进行生长迟缓预防和控制的重点民族。
在分地区进行比较后发现,生长迟缓的学生主要集中在西南地区,其次为中南和西北地区,华北、东北地区生长迟缓检出率最低,这与既往研究结果相似[13]。既往研究显示,中、低收入国家5岁以下儿童的生长迟缓与人均GDP增长存在关联[14],本研究结果与之相同,提示经济学因素可能是我国学龄期儿童生长迟缓的影响因素之一。但值得注意的是,生长迟缓率较高的水族人均GDP并非最低,而人均GDP最低的东乡族生长迟缓率也不高,既往研究曾报告水族因居住地的环境因素形成了以糯米为主食的饮食文化[15],而东乡族因为宗教信仰等原因,羊肉在其饮食文化中占重要地位[16]。因此在考虑少数民族生长迟缓问题时,还应该充分考虑民族特异性因素的影响。
研究显示,生长迟缓学生很可能存在认知能力低下的情况,进而导致学业水平较低、成年期收入较低等不良后果,甚至影响下一代人的发育潜力[17]。本研究对生长迟缓检出率较高的9个少数民族学生分析显示,各少数民族生长迟缓率的年龄分布并不一致。但多个少数民族学生生长迟缓集中在较高年龄组。据此推测,在未来一段时间内,这些民族16~18岁年龄组的大部分生长迟缓学生将难以通过干预使其达到较高的成年身高。然而青春期将迎来身高发育的第二个高峰期[18],那些生长迟缓检出率在各个年龄组差别不大以及集中在低年龄组的少数民族,如水族、布依族、撒拉族,有很大机会可以通过积极的营养干预,以减少生长迟缓带来的不良后果。既往研究指出,我国学生成年身高增长潜力不足的原因,除个体生活水平的差异外,青少年整体上存在优质蛋白和钙的摄入不足,不能满足青春期生长的需求[13]。为改善农村地区学生营养状况,我国开展了农村义务教育学生营养改善计划[19],可能会改善农村地区学生的营养状况,但与此同时,也应该注意优质蛋白和钙的补充,加强营养健康教育,避免出现生长迟缓与肥胖共同出现的情况。
本研究发现我国少数民族学生18岁身高差异较大,约1/3少数民族学生的生长迟缓率仍处在较高水平,尤其是西南地区少数民族学生生长迟缓率较高。
本研究存在局限性。首先,本研究是横断面研究,不能获得一代人连续的身高生长趋势,难以区分遗传和环境因素的影响。其次,本研究只涉及了26个少数民族,还有很多少数民族的数据没有数据支持。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
国家卫生和计划生育委员会. WS/T 456-2014学龄儿童青少年营养不良筛查[S].北京: 中国标准出版社, 2014. National Health and Family Planning Commission of PRC. WS/T 456-2014 Screening standard for malnutrition of school-age children and adolescents[S]. Beijing: Standards Press of China, 2014. |
| [2] |
World Health Organization. Reducing stunting in children: equity considerations for achieving the global targets 2025[EB/OL].[2018-07-10]. http://www.who.int/nutrition/publications/severemalnutrition/reducing-stunting-children-equity/en/.
|
| [3] |
Victora CG, Adair L, Fall C, et al. Maternal and child undernutrition:consequences for adult health and human capital[J]. Lancet, 2008, 371(9609): 340-357. DOI:10.1016/S0140-6736(07)61692-4 |
| [4] |
Walker SP, Chang SM, Wright A, et al. Early childhood stunting is associated with lower developmental levels in the subsequent generation of children[J]. J Nutr, 2015, 145(4): 823-828. DOI:10.3945/jn.114.200261 |
| [5] |
中国学生体质与健康研究组. 2014年中国学生体质与健康调研报告[M]. 北京: 高等教育出版社, 2016. Chinese Students' Physique and Health Research Group. Reports on the Physical Fitness and Health Research of Chinese School Students[M]. Beijing: Higher Education Press, 2016. |
| [6] |
中华人民共和国民政部. 2018年中华人民共和国行政区划代码[EB/OL]. (2018-06-28)[2018-07-11]. http://www.mca.gov.cn/article/sj/xzqh/2018/. Ministry of Civil Affairs of the People's Republic of China. Administrative division code of the People's Republic of China, 2018[EB/OL]. (2018-06-28)[2018-07-11].http://www.mca.gov.cn/article/sj/xzqh/2018/. |
| [7] |
国家卫生和计划生育委员会. 中国卫生和计划生育统计年鉴[M]. 北京: 中国协和医科大学出版社, 2017. National Health and Family Planning Commission of the People's Republic of China. Health and Family Planning Statistical Yearbook of China[M]. Beijing: Peking Union Medical College Press, 2017. |
| [8] |
宋逸, 胡佩瑾, 张冰, 等. 1985年至2010年中国18个少数民族17岁学生身高趋势分析[J]. 北京大学学报:医学版, 2015, 47(3): 414-419. Song Y, Hu PJ, Zhang B, et al. Secular trends of height among Chinese students aged 17 in 18 ethnic minorities from 1985 to 2010[J]. J Peking Univ:Health Sci, 2015, 47(3): 414-419. DOI:10.3969/j.issn.1671-167X.2015.03.010 |
| [9] |
宋逸, 胡佩瑾, 张冰, 等. 中国部分少数民族17岁女学生生长长期变化分析[J]. 中华流行病学杂志, 2012, 33(2): 192-196. Song Y, Hu PJ, Zhang B, et al. Changes on secular growth among minority girls in China from 1985 to 2005[J]. Chin J Epidemiol, 2012, 33(2): 192-196. DOI:10.3760/cma.j.issn.0254-6450.2012.02.015 |
| [10] |
刘春艳, 黄达峰, 韦蝶心, 等. 2000-2014年大理汉族、白族学生形态发育动态分析[J]. 预防医学情报杂志, 2016, 32(7): 727-731. Liu CY, Huang DF, Wei DX, et al. A dynamic analysis of morphological development of the Han and Bai students in Dali, 2000-2014[J]. J Prev Med Inf, 2016, 32(7): 727-731. |
| [11] |
国家统计局. 2010年第六次全国人口普查主要数据公报(第1号)[EB/OL]. (2011-04-28)[2018-07-11]. http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/qgrkpcgb/201104/t20110428_30327.html. National Bureau of Statistics. Bulletin on main data of the sixth national population census in 2010[EB/OL]. (2011-04-28)[2018-07-11]. http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/qgrkpcgb/201104/t20110428_30327.html. |
| [12] |
Song Y, Agardh A, Ma J, et al. National trends in stunting, thinness and overweight among Chinese school-aged children, 1985-2014[J]. Int J Obes, 2018. DOI:10.1038/s41366-018-0129-7.[Epubahead of print].
|
| [13] |
季成叶. 中国青少儿生长长期变化和干预建议[J]. 中国公共卫生, 2002, 18(6): 641-642. Ji CY. Secular growth changes of Chinese youth and intervene suggestions[J]. Chin J Public Health, 2002, 18(6): 641-642. DOI:10.11847/zgggws2002-18-06-01 |
| [14] |
Vollmer S, Harttgen K, Subramanyam MA, et al. Association between economic growth and early childhood undernutrition:evidence from 121 Demographic and Health Surveys from 36 low-income and middle-income countries[J]. Lancet Global Health, 2014, 2(4): e225-234. DOI:10.1016/S2214-109X(14)70025-7 |
| [15] |
蒙祥忠. 饮食里的象征、社会与生态——对贵州水族九阡酒的人类学考察[J]. 西南民族大学学报:人文社科版, 2018, 39(3): 22-29. Meng XZ. The symbolic society and ecology in the diet:an anthropological study of the Guizhou wine of Shui nationality[J]. J Southwest Univ Natl:Humanities and Social Sciences Edition, 2018, 39(3): 22-29. DOI:10.3969/j.issn.1004-3926.2018.03.004 |
| [16] |
张正红.甘肃省东乡族民俗活动中的养生健身价值研究[C]//2014第二届海峡两岸体育运动史学术研讨会.成都: 中国体育科学学会体育史分会, 2014. Zhang ZH. Study on the value of health preservation and fitness in the folk activities of Dongxiang nationality in Gansu province[C]//2014 Cross-Strait Academic Seminar on Sports History. Chengdu: Sports History Branch of China Sports Science Society, 2014. |
| [17] |
Kuruvilla S, Bustreo F, Kuo T, et al. The Global strategy for women's, children's and adolescents' health (2016-2030):a roadmap based on evidence and country experience[J]. Bull World Health Organ, 2016, 94(5): 398-400. DOI:10.2471/BLT.16.170431 |
| [18] |
季成叶. 儿童少年卫生学[M]. 北京: 北京大学医学出版社, 2006. Ji CY. Child and adolescent health[M]. Beijing: Peking University Medical Press, 2006. |
| [19] |
中华人民共和国教育部等十五部门.农村义务教育学生营养改善计划实施细则[EB/OL]. (2012-06-14)[2018-07-11]. http://www.gov.cn/zwgk/2012-06/14/content_2160689.htm. The ministry of education and the other fourteen departments of the People's Republic of China. The enforcement regulation of the nutrition improvement program for rural compulsory education students in China[EB/OL]. (2012-06-14)[2018-07-11]. http://www.gov.cn/zwgk/2012-06/14/content_2160689.htm. |