 2019, Vol. 40
2019, Vol. 40文章信息
- 吉宁, 王黎君, 刘世炜, 刘敏, 曾新颖, 周脉耕.
- Ji Ning, Wang Lijun, Liu Shiwei, Liu Min, Zeng Xinying, Zhou Maigeng.
- 1990年与2016年中国女性子宫纤维瘤的疾病负担研究
- Disease burden on uterine fibroids in China, 1990 and 2016
- 中华流行病学杂志, 2019, 40(2): 160-164
- Chinese Journal of Epidemiology, 2019, 40(2): 160-164
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.02.007
-
文章历史
收稿日期: 2018-09-02




2. 中国疾病预防控制中心慢性非传染性疾病预防控制中心生命登记与死因室, 北京 100050;
3. 中国疾病预防控制中心慢性非传染性疾病预防控制中心综合防控与评价室, 北京 100050;
4. 中国疾病预防控制中心慢性非传染性疾病预防控制中心, 北京 100050
2. Division of Vital Registry and Mortality Surveillance, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
3. Division of Comprehensive Prevention and Evaluation, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
4. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
疾病负担研究利用一系列统计指标反映疾病或伤残导致的失能或过早死亡对一个国家或地区所造成的社会负担[1]。全球疾病负担研究(GBD)利用伤残调整寿命年(disability-adjusted life year,DALY)等指标进行健康评价,是涵盖病种广泛、覆盖地区全面的流行病学研究之一[2]。子宫纤维瘤,又称子宫肌瘤或子宫平滑肌瘤,是源于子宫平滑肌的单细胞良性肿瘤,由于仅有15%~30%的女性会有严重的临床症状,因而相对于恶性肿瘤,对子宫纤维瘤的关注较少[3]。子宫纤维瘤非常高发,女性累积患病风险约为70%,15~54岁女性29%的住院,40%~60%的子宫切除是由子宫纤维瘤所致[4-5],美国每年因子宫纤维瘤导致的经济损失高达59亿~344亿美元[3]。目前中国关于子宫纤维瘤疾病负担研究较少,本研究应用GBD2016的结果,分析中国1990年和2016年子宫纤维瘤的患病情况和疾病负担。
资料与方法1.资料来源:数据均来自GBD2016,相关背景和概况参见文献[6-10]。GBD2016对中国子宫纤维瘤数据的估计,来源于中国医院住院患者登记数据和已发表的科学文献,主要步骤:①子宫纤维瘤诊断方式:包括盆腔检查、子宫切除、自我报告和超声检查。②估计子宫纤维瘤的伤残权重:GBD伤残权重系数的估计基于对后遗症的描述,强调主要功能后果和症状。子宫纤维瘤按严重程度分为轻度盆腹腔问题、轻度贫血、中度贫血、重度贫血;伴有轻度腹痛的贫血归因于纤维瘤,单独贫血不纳入;同时使用医疗费用专项调查的数据来确定分级。③估计子宫纤维瘤的疾病负担:采用DisMod MR 2.2软件进行数据处理建模。具体方法参见文献[5]。
2.疾病分类和编码:采用《疾病和有关健康问题的国际统计分类》第十次修订本,其中子宫纤维瘤的编码范围为D25~D28.2[5, 11]。
3.数据分析:分析2016年中国不同年龄、地区女性子宫纤维瘤的患病率及所致的DALY,并与1990年相比较。DALY是常用的疾病负担指标,综合性描述健康状况、生命质量和寿命年损失,是过早死亡损失寿命年(years of life lost due to premature mortality,YLL)和伤残损失寿命年(years lived with disability,YLD)的综合,其中YLL=标准期望寿命—死亡年龄,YLD=伤残年数×伤残权重,DALY=YLL+YLD;变化率=(2016年值—1990年值)/1990年值×100%;使用2010—2035年WHO的世界标准人口对不同省份、年份的数据进行标化比较。
结果1.中国女性子宫纤维瘤疾病负担情况:1990年和2016年中国≥15岁女性子宫纤维瘤的患病人数分别为13 695 567人和27 169 312人,患病率分别为2.48%和4.10%,标化患病率分别为2.97%和3.03%;DALY值分别为146 045.05人年和281 976.67人年,DALY率分别为26.40/10万和42.50/10万,标化DALY率分别为30.40/10万和32.20/10万;与1990年相比,2016年中国女性子宫纤维瘤患病人数增加13 473 745人,相对增长98.38%,标化患病率相对上升1.88%;DALY值增加135 931.62人年,相对上升93.08%,标化DALY值的变化率为5.92%。1990—2016年中国女性子宫纤维瘤的标化患病率平稳,标化DALY率呈上升趋势(图 1)。

|
| 图 1 1990—2016年中国女性子宫纤维瘤标化患病率和标化DALY率变化趋势 |
2.不同年龄女性子宫纤维瘤所致疾病负担:1990年和2016年≥15岁女性子宫纤维瘤的患病率和DALY率,从15岁开始随年龄增加而增加,45~49岁达顶峰,之后随年龄增加而降低。40~54岁年龄段女性子宫纤维瘤的患病数占总人数的55.60%(1990年)和66.74%(2016年);该年龄段DALY值占总量的48.37%(1990年)和60.65%(2016年)。中国女性子宫纤维瘤疾病负担随年龄变化趋势,1990年与2016年趋于一致(图 2)。

|
| 图 2 1990年和2016年中国不同年龄女性子宫纤维瘤的患病率和DALY率 |
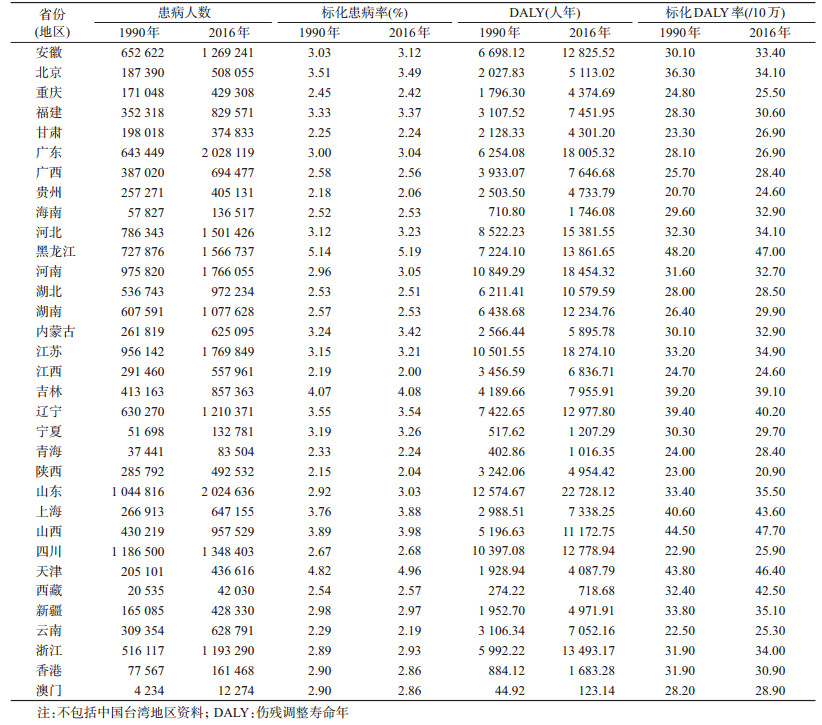
3.中国不同省份女性子宫纤维瘤所致疾病负担:1990年中国女性子宫纤维瘤患病人数前3位的省份为四川(1 186 500)、山东(1 044 816)和河南(975 820),2016年为广东(2 028 119)、山东(2 024 636)和江苏(1 769 849);1990年和2016年标化患病率最高的3个省份均为黑龙江(1990年:5.14%;2016年:5.19%)、天津(1990年:4.82%;2016年:4.96%)和吉林(1990年:4.07%;2016年:4.08%)。1990年和2016年DALY值较高的3个省份均为山东(1990年:12 574.67人年;2016年:22 728.12人年)、河南(1990年:10 849.29人年;2016年:18 454.32人年)和江苏(1990年:10 501.55人年;2016年:18 274.10人年),标化DALY率较高的3个省份在1990年和2016年均为黑龙江(1990年:48.20/10万;2016年:47.00/10万)、山西(1990年:44.50/10万;2016年:47.70/10万)和天津(1990年:43.80/10万;2016年:46.40/10万)。1990年和2016年中国女性子宫纤维瘤所致疾病负担变化:所有省份的患病人数均升高,标化患病率18个省份上升,15个省份下降;所有省份的DALY值均升高,标化DALY率25个省份上升,8个省份下降(表 1)。
DALY是由疾病或死亡所引起的健康损失。2016年中国女性子宫纤维瘤导致的DALY占全球的19.28%(全球1 462 537.27人年),平均每10万人损失42.50个寿命年,略高于全球水平(39.89年/10万);子宫纤维瘤在中国是疾病负担位居第二的妇科疾病[12]。
据文献报道,子宫纤维瘤常与不孕症同时存在,扰乱子宫的功能,造成过度出血、贫血、胚胎植入缺陷、重复流产、早产、盆腔不适、尿失禁等,并可能发生恶变,严重威胁女性健康。子宫纤维瘤是卵巢激素依赖性肿瘤,青春期前罕见,好发于育龄期女性,病理诊断在50岁达到最高峰[4, 13]。本研究结果显示,子宫纤维瘤的患病率和DALY率与年龄均呈“∧”形关系,45~49岁达到顶峰,且超过50%的患者集中在40~54岁,因此需特别注重绝经期前后女性子宫纤维瘤的防治工作。
分省份分析结果显示,2016年DALY值前3位的省份分别为山东、河南和江苏,这可能与该3个省份均为人口大省有关[14]。从标化DALY率来看,中部地区相对较低,东部和西部省份相对较高;与1990年相比,DALY标化率的变化最快的3个省份为西藏、贵州和青海,具体原因不明,可能与当地医疗水平提高,健康体检的普及率增加有关,尚待进一步研究。本研究结果提示,人口大省应重视女性子宫纤维瘤防治工作;尽管西藏、贵州和青海等西部地区的总DALY值和标化DALY率不在全国前列,但标化DALY率的增长速度快,应引起重视。
与1990年相比,2016年中国女性子宫纤维瘤的患病人数、患病率、标化患病率、DALY值、DALY率和标化DALY率均上升。肥胖尤其是中心性肥胖和生活方式,包括膳食、咖啡因、吸烟、饮酒、身体活动、压力等均与子宫纤维瘤的发生密切相关[15-16]。1990—2016年,中国子宫纤维瘤的标化患病率均高于全球平均水平[17],这可能与中国肥胖严重有关,《中国慢性病及危险因素监测报告2013》指出[18],中国成年人女性超重和肥胖率为31.0%和14.1%,中心性肥胖率为51.4%,也就是说约每2名成年女性中就有1人是超重或肥胖的。此外,人工流产是子宫纤维瘤的重要风险因素,中国约1/3的女性至少经历过1次以上人工流产,是流产严重国家[19],这可能是中国子宫纤维瘤患病较全球高的原因之一。与全球平均水平相比,中国子宫纤维瘤的标化DALY率相对较低[17],这可能与随着中国医疗均等化的发展,中国女性子宫纤维瘤患者可相对较早发现及诊断治疗。子宫纤维瘤导致的DALY值在26年间增长了98.38%,即总的疾病负担增长迅猛,这期间中国总人口的增加和生活方式发生巨大变化,可能是其主要原因[20-21]。如不采取有效措施,子宫纤维瘤的疾病负担将会进一步增加。
本研究存在局限性。研究数据来自GBD2016中国部分的疾病负担研究,GBD对子宫纤维瘤疾病负担的估计方法不足之处在本研究中也同样存在。研究数据与全球存在可比性,但与真实水平存在一定差异[22]。
综上所述,子宫纤维瘤主要困扰绝经期女性,中国女性子宫纤维瘤导致的DALY值在过去26年约增长了一倍,应引起关注。中国子宫纤维瘤的患病率、标化患病率、DALY率和标化DALY率均有增长趋势,如不加以控制,疾病负担会进一步增加。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
何亚楠, 王霞, 伍晓玲, 等. 疾病负担统计的数据模型与统计元数据[J]. 中国卫生统计, 2016, 33(1): 12-15. He YN, Wang X, Wu XL, et al. Data model and statistical metadata in the statistical measurement on the burden of disease[J]. Chin J Health Stat, 2016, 33(1): 12-15. |
| [2] |
宇传华, 崔芳芳. 全球疾病负担研究及其对我国的启示[J]. 公共卫生与预防医学, 2014, 25(2): 1-5. Yu CH, Cui FF. Global disease burden study and its enlightenment to China[J]. J Public Health and Prev Med, 2014, 25(2): 1-5. |
| [3] |
Bulun SE. Uterine fibroids[J]. N Engl J Med, 2018, 369(14): 1344-1355. DOI:10.1056/NEJMra1209993 |
| [4] |
Whiteman MK, Kuklina E, Jamieson DJ, et al. Inpatient hospitalization for gynecologic disorders in the United States[J]. Am J Obstet Gynecol, 2010, 202(6): 541.e1-541.e6. DOI:10.1016/j.ajog.2009.12.013 |
| [5] |
Merrill RM. Hysterectomy surveillance in the United States, 1997 through 2005[J]. Med Sci Monit, 2008, 14(1): CR24-31. |
| [6] |
GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet, 2017, 390(10100): 1345-1422. DOI:10.1016/S0140-6736(17)32366-8 |
| [7] |
GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet, 2017, 390(10100): 1260-1344. DOI:10.1016/S0140-6736(17)32130-X |
| [8] |
刘韫宁, 齐金蕾, 刘江美, 等. 1990年与2013年中国人群肺癌疾病负担分析[J]. 中华流行病学杂志, 2016, 37(6): 752-757. Liu YN, Qi JL, Liu JM, et al. Disease burden of lung cancer in the Chinese population, in 1990 and 2013[J]. Chin J Epidemiol, 2016, 37(6): 752-757. DOI:10.3760/cma.j.issn.0254-6450.2016.06.002 |
| [9] |
王黎君, 殷鹏, 刘韫宁, 等. 1990年与2013年中国人群肝癌疾病负担研究[J]. 中华流行病学杂志, 2016, 37(6): 758-762. Wang LJ, Yin P, Liu YN, et al. Disease burden of liver cancer in the Chinese population, in 1990 and 2013[J]. Chin J Epidemiol, 2016, 37(6): 758-762. DOI:10.3760/cma.j.issn.0254-6450.2016.06.003 |
| [10] |
Zhang GS, Yu CH, Zhou MG, et al. Burden of Ischaemic heart disease and attributable risk factors in China from 1990 to 2015:findings from the global burden of disease 2015 study[J]. BMC Cardiovasc Disord, 2018, 18: 18. DOI:10.1186/s12872-018-0761-0 |
| [11] |
WHO. ICD-10 Version: 2016[EB/OL].[2018-08-08]. http://apps.who.int/classifications/icd10/browse/2016/en.
|
| [12] |
吉宁, 刘世炜, 曾新颖, 等. 2016年中国妇科疾病的疾病负担研究[J]. 中华妇产科杂志, 2018, 53(5): 313-318. Ji N, Liu SW, Zeng XY, et al. Disease burden for gynecological disease in China, 2016[J]. Chin J Obstet Gynecol, 2018, 53(5): 313-318. DOI:10.3760/cma.j.issn.0529-567x.2018.05.006 |
| [13] |
Marshall LM, Spiegelman D, Barbieri RL, et al. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race[J]. Obstet Gynecol, 1997, 90(6): 967-973. DOI:10.1016/S0029-7844(97)00534-6 |
| [14] |
国务院人口普查办公室.中国第六次人口普查资料[EB/OL].[2018-08-08]. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm. Office of Population Census of the State Council. The sixth national population census[EB/OL].[2018-08-08]. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm. |
| [15] |
Yang Y, He Y, Zeng Q, et al. Association of body size and body fat distribution with uterine fibroids among Chinese women[J]. J Womens Health (Larchmt), 2014, 23(7): 619-626. DOI:10.1089/jwh.2013.4690 |
| [16] |
Pavone D, Clemenza S, Sorbi F, et al. Epidemiology and Risk Factors of Uterine Fibroids[J]. Best Pract Res Clin Obstet Gynaecol, 2018, 46: 3-11. DOI:10.1016/j.bpobgyn.2017.09.004 |
| [17] |
Institute for Health Metrics and Evaluation. Global Health Data Exchange[EB/OL].[2018-08-08]. http://ghdx.healthdata.org/about-ghdx.
|
| [18] |
中国疾病预防控制中心, 中国疾病预防控制中心慢性非传染性疾病预防控制中心编. 中国慢性病及危险因素监测报告2013[M]. 北京: 军事医学出版社, 2016: 4. Chinese Center for Disease Control and Prevention, National Center for Chronic and Noncommunicable Disease Control and Prevention of Chinese Center for Disease Control and Prevention. Report on Chronic Disease Risk Factor Surveillance in China 2013[M]. Beijing: Military Medical Science Press, 2016: 4. |
| [19] |
Wang CT. Induced abortion patterns and determinants among married women in China:1979 to 2010[J]. Reprod Health Matters, 2014, 22(43): 159-168. DOI:10.1016/S0968-8080(14)43753-4 |
| [20] |
He Y, Zeng Q, Dong SY, et al. Associations between uterine fibroids and lifestyles including diet, physical activity and stress:a case-control study in China[J]. Asia Pac J Clin Nutr, 2013, 22(1): 109-117. DOI:10.6133/apjcn.2013.22.1.07 |
| [21] |
Yang GH, Wang Y, Zeng YX, et al. Rapid health transition in China, 1990-2010:findings from the Global Burden of Disease Study 2010[J]. Lancet, 2013, 381(9882): 1987-2015. DOI:10.1016/S0140-6736(13)61097-1 |
| [22] |
Murray CJL, Lopez AD. Measuring global health:motivation and evolution of the Global Burden of Disease Study[J]. Lancet, 2017, 390(10100): 1460-1464. DOI:10.1016/S0140-6736(17)32367-X |