 2019, Vol. 40
2019, Vol. 40文章信息
- 姜莹莹, 刘敏, 吉宁, 曾新颖, 董文兰, 毛凡, 刘世炜, 董建群, 周脉耕.
- Jiang Yingying, Liu Min, Ji Ning, Zeng Xinying, Dong Wenlan, Mao Fan, Liu Shiwei, Dong Jianqun, Zhou Maigeng.
- 1990-2016年中国高BMI导致的糖尿病疾病负担研究
- Disease burden of diabetes attributable to high body mass index in China, 1990-2016
- 中华流行病学杂志, 2019, 40(1): 46-51
- Chinese Journal of Epidemiology, 2019, 40(1): 46-51
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2019.01.010
-
文章历史
收稿日期: 2018-05-24




2. 中国疾病预防控制中心慢性非传染性疾病预防控制中心健康促进与行为干预室, 北京 100050;
3. 中国疾病预防控制中心慢性非传染性疾病预防控制中心生命登记及死因监测室, 北京 100050;
4. 中国疾病预防控制中心慢性非传染性疾病预防控制中心, 北京 100050
2. Department of Risk Factor Intervention and Health Promotion, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
3. Division of Vital Registry and Death Cause Surveillance, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
4. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
近年来,我国成年人糖尿病的患病率不断攀升,最新数据显示已经高达10.9%,糖尿病已成为影响我国居民健康的重大公共卫生问题[1]。超重和肥胖是造成糖尿病发生和发展的独立危险因子[2],会增加糖尿病患者FPG和餐后血糖的控制难度,并且增加糖尿病并发症如冠心病、心肌梗死、脑卒中等的发生风险,严重威胁糖尿病患者的生存质量[3-7]。本研究利用全球疾病负担研究(Global Burden of Disease,GBD)2016年数据,全面分析1990-2016年超重/肥胖导致中国糖尿病归因疾病负担和死亡情况及其变化,为评价和制定糖尿病防治策略和措施提供数据支持。
对象与方法1.资料来源:本研究数据来自于GBD2016。GBD2016利用统一、可比的方法全面分析和估计了1990-2016年195个国家或地区、分年龄、性别的328种疾病或伤害、2 982种疾病后遗症的患病数(率)和疾病负担指标,同时对84种危险因素的归因疾病负担进行了系统梳理,该研究的背景和方法见文献[8-10]。本研究从中选取归因于高BMI(≥25 kg/m2)的糖尿病死亡资料以及疾病负担,包括伤残调整寿命年(disability adjusted of life years,DALY)、过早死亡损失寿命年(years of life lost,YLL)和伤残损失寿命年(years lived with disability,YLD)资料进行分析。其中DALY=YLL+YLD,YLL和YLD的估计方式详见文献[9-11]。
2. GBD2016中国研究的资料来源:GBD2016中国研究采用全球疾病负担的方法,系统分析了所有可获取的中国省级水平的人口学和流行病学数据。
(1)与高BMI具有病因学联系糖尿病的死亡数据:1990年以来中国疾病监测点系统死因监测,中国妇幼卫生监测网,中国CDC死因登记报告信息系统,肿瘤登记数据,中国澳门地区和中国香港地区死因数据,以及其他已发表和未发表的研究和报告等,并采用贝叶斯Meta回归、时空高斯过程回归、模型寿命表等方法估计和填补不同时间、省份、性别和年龄的死亡数据。
(2)BMI数据来源:已经发表的文献和国家级调查,包括1992和2002年中国居民营养与健康调查,2004、2007、2010和2013年中国慢性病及其危险因素监测,1993、1998、2003、2008和2013年国家卫生服务调查,中国健康与养老追踪调查,并采用时空高斯过程回归模型估计中国不同时间、省份、性别、年龄的BMI水平[10-12]。
(3)BMI与糖尿病的关联强度数据:相关前瞻性队列研究、文献回顾、系统综述及Meta分析[10, 13-15]。
3.归因疾病负担的原理:
(1)人群归因分值(population attributable fraction,PAF):按照比较风险评估理论,计算糖尿病疾病负担归因于BMI的PAF,PAF的计算方法和公式具体见文献[16]。BMI的最小理论暴露分布均值为25 kg/m2,标准差为1 kg/m2,BMI在该分布时,导致人群发生糖尿病或死亡的风险最低。
(2)归因于高BMI的糖尿病疾病负担计算:归因于高BMI的糖尿病疾病负担=PAF×M,M为糖尿病的总疾病负担。以2010-2035年世界人口的平均人口结构作为标准人口结构[8-9],对死亡率进行标化。
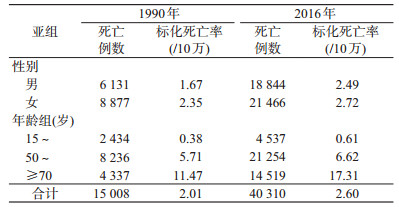
结果1.高BMI造成的糖尿病死亡数和标化死亡率:1990-2016年高BMI造成的糖尿病死亡数和标化死亡率见图 1。2016年归因于高BMI的糖尿病死亡数为40 310例,较1990年的15 008例有大幅攀升。归因于高BMI的糖尿病标化死亡率在1990年为2.01/10万,在1995年达到峰值,随后呈现波动下降的趋势,2016年的标化死亡率为2.60/10万。与女性相比,男性归因于高BMI的糖尿病死亡数和标化死亡率低,但标化死亡率的增幅高。高BMI导致的糖尿病死亡数和标化死亡率随年龄递增,其中15~岁组糖尿病患者归因于高BMI的标化死亡率增幅最大。见表 1。

|
| 图 1 1990-2016年高BMI造成的糖尿病死亡例数和标化死亡率的变化趋势 |
2.高BMI造成的糖尿病疾病负担:1990-2016年,高BMI导致的糖尿病的疾病负担呈现快速增长的趋势(图 2),DALY率、YLL率和YLD率的变化趋势见图 3。高BMI导致糖尿病的DALY从1990年的108.91万人年增长至2016年的330.02万人年,50~岁组的DALY和YLL的增长速度最快,15~岁组的YLD的增长速度最快。2016年高BMI导致的糖尿病DALY率为241.42/10万,比1990年的95.88/10万有明显增长,15~岁组的DALY率、YLL率和YLD率的增幅均较高。见表 2。

|
| 注:DALY:伤残调整寿命年;YLL:过早死亡损失寿命年;YLD:伤残损失寿命年 图 2 1990-2016年高BMI造成的糖尿病疾病负担的变化趋势 |

|
| 注:DALY:伤残调整寿命年;YLL:过早死亡损失寿命年;YLD:伤残损失寿命年 图 3 1990-2016年高BMI造成的糖尿病疾病负担率的变化趋势 |

3.高BMI导致糖尿病死亡和疾病负担的PAF:2016年高BMI导致糖尿病死亡数占糖尿病总死亡数的26.01%,较1990年的18.66%增长了39.39%;高BMI导致的糖尿病DALY占糖尿病总DALY的37.47%,较1990年的24.20%增长了54.83%;高BMI导致的糖尿病YLL和YLD也有明显增长,其中YLD的增长幅度更快(表 3)。

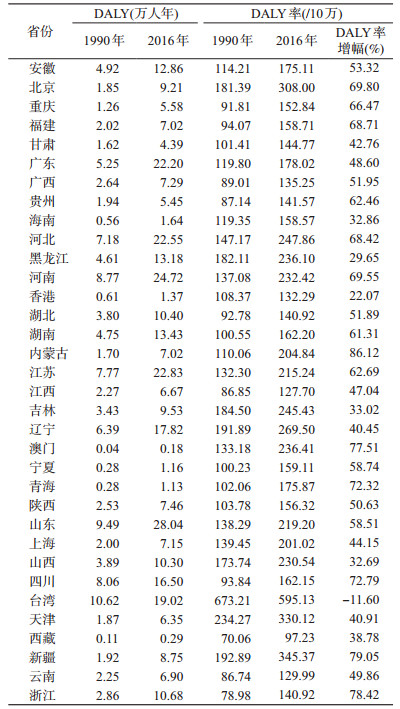
4.中国各省份高BMI造成的糖尿病疾病负担:与1990年相比,2016年中国所有省份高BMI造成的糖尿病DALY均呈大幅增长。2016年,山东省、河南省、江苏省、河北省、广东省高BMI造成的糖尿病DALY均>22.20万人年。与1990年相比,台湾地区、香港地区、黑龙江省、山西省、海南省的DALY率的增长相对较低,而内蒙古自治区、新疆维吾尔自治区、浙江省、澳门地区、四川省和青海省的DALY率增幅非常明显,内蒙古自治区的DALY率增幅达86.12%,新疆维吾尔自治区、浙江省、澳门地区、四川省和青海省的DALY率增幅均超过了70%。见表 4。
本研究利用GBD2016的中国数据分析了1990-2016年中国糖尿病高BMI归因死亡和疾病负担的情况及变化。2016年,26%的中国糖尿病死亡病例可归因于高BMI。仅20年,高BMI造成的糖尿病死亡人群PAF的增幅就高达39.39%,与过往研究一致。研究表明超重/肥胖是导致糖尿病的最重要的危险因素[17-19],超重/肥胖的亚洲地区人群的健康风险更高[20-25]。尽管中国的超重/肥胖率处于全球较低水平[12],但中国成年人超重/肥胖的比例一直呈增长的趋势[26-28],且30年间的增长幅度远高出全球平均水平[12]。作为糖尿病发生和死亡的主要危险因素,超重/肥胖的持续、快速增长使得中国的糖尿病防控工作面临着巨大的挑战。
中国幅员辽阔、各省人口数和经济发展水平差异较大,糖尿病的流行情况存在较大差异[29]。本研究表明,中国高BMI导致的糖尿病疾病负担差异也较大,人口大省如山东省、河南省、江苏省、河北省和广东省面临着最为沉重的糖尿病疾病负担。本研究结果显示,内蒙古自治区、新疆维吾尔自治区、浙江省、澳门地区、四川省和青海省由于高BMI造成的糖尿病DALY率的增幅均达到70%以上,与过往研究结果类似[30]。这一结果提示,即使是经济水平相对落后、人均期望寿命亦较低的省份[31],依然面临着高BMI导致的糖尿病疾病负担迅速增长的沉重压力。
本次研究发现1990年至今,与女性相比,高BMI导致的男性糖尿病死亡率的增幅更高,可能因为中国男性超重/肥胖的流行水平一直以来都明显高于女性[11-12],因此针对超重/肥胖的男性糖尿病患者开展积极减重的健康促进工作十分必要。在不同年龄组人群中,15~岁组归因于高BMI的糖尿病死亡率、YLD、DALY率的增幅最大,可能与中国的糖尿病防控广覆盖项目主要覆盖社区≥60岁的糖尿病患者有关[32],且15~岁组人群的糖尿病防控健康管理服务在中国鲜有提供和报道。美国内分泌医师协会和美国内分泌协会联合发布的超重/肥胖综合管理临床实践指南中明确指出减重对病程短的患者可以明显缓解糖尿病病情[33],因此建议应对中国的中青年糖尿病患者开展积极减重的健康促进工作,以期获得更大收益。
超重/肥胖是不良膳食习惯、身体活动不足、能量代谢失衡的后果之一。中国经济经过30余年的高速发展,带来了中国居民膳食结构和身体活动方式的巨大变化。谷类摄入减少、蔬菜水果摄入不足、肉类和食用油摄入快速增加,久坐少动生活方式日益普遍[34]。生活方式的改善是体重管理的最基本点[33],也是遏制高BMI导致的日益沉重的糖尿病疾病负担的首要策略和原则,亟需更多的健康教育引导。
本次研究存在局限性。PAF的计算假定糖尿病相关的各个危险因素是独立的,然而糖尿病各个危险因素之间可能存在着关联,如吸烟和超重/肥胖,需要进一步完善糖尿病PAF的估计方法。另外,GBD中糖尿病风险的估计研究还需要纳入更多的中国本土研究来增加疾病负担分析结果的可靠性。
总的说来,1990-2016年,中国高BMI导致的糖尿病死亡病例显著增加,高BMI造成的糖尿病死亡率增幅显著。目前糖尿病治疗领域以降糖为中心的理念正在改变,倡导血压、血糖、血脂及并发症的综合管理。结合本研究结果,除了上述危险因素外,为了使得糖尿病患者的血糖、血压、血脂得到更好的控制,体重管理也应被给予足够的重视。中国幅员辽阔,不同省份的高BMI导致的糖尿病疾病负担差异也很大,建议结合疾病负担的现状和增幅分析原因并循证地分配有限的卫生资源。此外,高BMI造成的糖尿病死亡和疾病负担在不同性别、不同年龄段人群中也存在明显差异。作为糖尿病防治相对空白的人群,男性和15~49岁糖尿病患者的健康体重管理需求应给予足够的重视和卫生资源分配的倾斜。
利益冲突 所有作者均声明不存在利益冲突
| [1] |
Wang LM, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013[J]. JAMA, 2017, 317(24): 2515-2523. DOI:10.1001/jama.2017.7596 |
| [2] |
Poirier P, Giles TD, Bray GA, et al. Obesity and cardiovascular disease:pathophysiology, evaluation, and effect of weight loss[J]. Circulation, 2006, 113(6): 898-918. DOI:10.1161/CIRCULATIONAHA.106.171016 |
| [3] |
周翔海. 肥胖合并2型糖尿病患者的特征分析——基于患者的临床研究[J]. 中国糖尿病杂志, 2013, 21(6): 575-576. Zhou XH. The characteristics of people with obesity and type 2 diabetes-clinical studies[J]. Chin J Diab, 2013, 21(6): 575-576. DOI:10.3969/j.issn.1006-6187.2013.06.031 |
| [4] |
Kenchaiah S, Evans JC, Levy D, et al. Obesity and the risk of heart failure[J]. N Engl J Med, 2002, 347(5): 305-313. DOI:10.1056/NEJMoa020245 |
| [5] |
Murphy NF, Macintyre K, Stewart S, et al. Long-term cardiovascular consequences of obesity:20-year follow-up of more than 15000 middle-aged men and women (the Renfrew-Paisley study)[J]. Eur Heart J, 2006, 27(1): 96-106. DOI:10.1093/eurheartj/ehi506 |
| [6] |
赵连成, 武阳丰, 周北凡, 等. 体质指数与冠心病、脑卒中发病的前瞻性研究[J]. 中华心血管病杂志, 2002, 30(7): 430-433. Zhao LC, Wu YF, Zhou BF, et al. A prospective study on the association of body mass index with incidence of coronary heart disease and stroke[J]. Chin J Cardiol, 2002, 30(7): 430-433. DOI:10.3760/j:issn:0253-3758.2002.07.014 |
| [7] |
Guh DP, Zhang W, Bansback N, et al. The incidence of co-morbidities related to obesity and overweight:a systematic review and Meta-analysis[J]. BMC Public Health, 2009, 9: 88. DOI:10.1186/1471-2458-9-88 |
| [8] |
GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet, 2017, 390(10100): 1211-1259. DOI:10.1016/S0140-6736(17)32154-2 |
| [9] |
GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet, 2017, 390(10100): 1260-1344. DOI:10.1016/S0140-6736(17)32130-X |
| [10] |
GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet, 2017, 390(10100): 1345-1422. DOI:10.1016/S0140-6736(17)32366-8 |
| [11] |
Zhou MG, Wang HD, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990-2013:a systematic subnational analysis for the Global Burden of Disease Study 2013[J]. Lancet, 2016, 387(10015): 251-272. DOI:10.1016/S0140-6736(15)00551-6 |
| [12] |
Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013:a systematic analysis for the Global Burden of Disease Study 2013[J]. Lancet, 2014, 384(9945): 766-781. DOI:10.1016/S0140-6736(14)60460-8 |
| [13] |
Prospective Studies Collaboration. Body-mass index and cause-specific mortality in 900000 adults:collaborative analyses of 57 prospective studies[J]. Lancet, 2009, 373(9669): 1083-1096. DOI:10.1016/S0140-6736(09)60318-4 |
| [14] |
The Emerging Risk Factors Collaboration. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease:collaborative analysis of 58 prospective studies[J]. Lancet, 2011, 377(9771): 1085-1095. DOI:10.1016/S0140-6736(11)60105-0 |
| [15] |
Bhaskaran K, Douglas I, Forbes H, et al. Body-mass index and risk of 22 specific cancers:a population-based cohort study of 5.24 million UK adults[J]. Lancet, 2014, 384(9945): 755-765. DOI:10.1016/S0140-6736(14)60892-8 |
| [16] |
Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet, 2012, 380(9859): 2224-2260. DOI:10.1016/S0140-6736(12)61766-8 |
| [17] |
Li YP, Wang DD, Ley SH, et al. Time trends of dietary and lifestyle factors and their potential impact on diabetes burden in China[J]. Diabetes Care, 2017, 40(12): 1685-1694. DOI:10.2337/dc17-0571 |
| [18] |
Laaksonen MA, Knekt P, Rissanen H, et al. The relative importance of modifiable potential risk factors of type 2 diabetes:a Meta-analysis of two cohorts[J]. Eur J Epidemiol, 2010, 25(2): 115-124. DOI:10.1007/s10654-009-9405-0 |
| [19] |
Huerta JM, Tormo MJ, Chirlaque MD, et al. Risk of type 2 diabetes according to traditional and emerging anthropometric indices in Spain, a Mediterranean country with high prevalence of obesity:results from a large-scale prospective cohort study[J]. BMC Endocr Disord, 2013, 13: 7. DOI:10.1186/1472-6823-13-7 |
| [20] |
Lee CM, Huxley RR, Lam TH, et al. Prevalence of diabetes mellitus and population attributable fractions for coronary heart disease and stroke mortality in the WHO South-East Asia and Western Pacific regions[J]. Asia Pac J Clin Nutr, 2007, 16(1): 187-192. |
| [21] |
Chan JCN, Malik V, Jia WP, et al. Diabetes in Asia:epidemiology, risk factors, and pathophysiology[J]. JAMA, 2009, 301(20): 2129-2140. DOI:10.1001/jama.2009.726 |
| [22] |
Huxley RR, James WPT, Barzi F, et al. Ethnic comparisons of the cross-sectional relationships between measures of body size with diabetes and hypertension[J]. Obes Rev, 2008, 9(S1): 53-61. DOI:10.1111/j.1467-789X.2007.00439.x |
| [23] |
Bell AC, Adair LS, Popkin BM. Ethnic differences in the association between body mass index and hypertension[J]. Am J Epidemiol, 2002, 155(4): 346-353. DOI:10.1093/aje/155.4.346 |
| [24] |
Pan WH, Flegal KM, Chang HY, et al. Body mass index and obesity-related metabolic disorders in Taiwanese and US whites and blacks:implications for definitions of overweight and obesity for Asians[J]. Am J Clin Nutr, 2004, 79(1): 31-39. DOI:10.1093/ajcn/79.1.31 |
| [25] |
Chen Y, CoDeland WK, Vedanthan R, et al. Association between body mass index and cardiovascular disease mortality in east Asians and south Asians:pooled analysis of prospective data from the Asia Cohort Consortium[J]. BMJ, 2013, 347(3): f5446. DOI:10.1136/bmj.f5446 |
| [26] |
马冠生, 李艳平, 武阳丰, 等. 1992至2002年间中国居民超重率和肥胖率的变化[J]. 中华预防医学杂志, 2005, 39(5): 311-315. Ma GS, Li YP, Wu YF, et al. The prevalence of body overweight and obesity and its changes among Chinese people during 1992 to 2002[J]. Chin J Prev Med, 2005, 39(5): 311-315. DOI:10.3760/j:issn:0253-9624.2005.05.005 |
| [27] |
翟屹, 房红芸, 于文涛, 等. 2010-2012年中国成年人腰围水平与中心型肥胖流行特征[J]. 中华预防医学杂志, 2017, 51(6): 506-512. Zhai Y, Fang HY, Yu WT, et al. Epidemiological characteristics of waist circumference and abdominal obesity among Chinese adults in 2010-2012[J]. Chin J Prev Med, 2017, 51(6): 506-512. DOI:10.3760/cma.j.issn.0253-9624.2017.06.010 |
| [28] |
李晓燕, 姜勇, 胡楠, 等. 2010年我国成年人超重及肥胖流行特征[J]. 中华预防医学杂志, 2012, 46(8): 683-686. Li XY, Jiang Y, Hu N, et al. Prevalence and characteristic of overweight and obesity among adults in China, 2010[J]. Chin J Prev Med, 2012, 46(8): 683-686. DOI:10.3760/cma.j.issn.0253-9624.2012.08.003 |
| [29] |
Zhou MG, Thomas AB, Bi YF, et al. Geographical variation in diabetes prevalence and detection in China:Multilevel spatial analysis of 98, 058 adults[J]. Diab Care, 2015, 38(1): 72-81. DOI:10.2337/dc14-1100 |
| [30] |
曾新颖, 李镒冲, 刘世炜, 等. 1990与2013年中国15岁以上人群归因于高BMI的死亡分析[J]. 中华预防医学杂志, 2016, 50(9): 776-781. Zeng XY, Li YC, Liu SW, et al. Mortality attributable to high body mass index in Chinese people aged 15 or over, in 1990 and 2013[J]. Chin J Prev Med, 2016, 50(9): 776-781. DOI:10.3760/cma.j.issn.0253-9624.2016.09.006 |
| [31] |
周脉耕, 李镒冲, 王海东, 等. 1990-2015年中国分省期望寿命和健康期望寿命分析[J]. 中华流行病学杂志, 2016, 37(11): 1439-1443. Zhou MG, Li YC, Wang HD, et al. Analysis on life expectancy and healthy life expectancy in China, 1990-2015[J]. Chin J Epidemiol, 2016, 37(11): 1439-1443. DOI:10.3760/cma.j.issn.0254-6450.2016.11.001 |
| [32] |
邓茜, 张梅, 黄正京, 等. 全国疾病监测点35岁及以上糖尿病患者管理现状研究[J]. 中华流行病学杂志, 2016, 37(9): 1191-1195. Deng Q, Zhang M, Huang ZJ, et al. Management of diabetes patients aged ≥ 35 years in disease surveillance areas in China[J]. Chin J Epidemiol, 2016, 37(9): 1191-1195. DOI:10.3760/cma.j.issn.0254-6450.2016.09.002 |
| [33] |
赵宇星, 朱惠娟, 王林杰. 2016年美国临床内分泌医师学会/美国内分泌学会肥胖症综合管理临床实践指南解读[J]. 中国糖尿病杂志, 2017, 25(1): 10-13. Zhao YX, Zhu HJ, Wang LJ. Interpretation of 2016 American Association of Clinical Endocrinologists(AACE) and American College of Endocrinology(ACE) clinical practice guidelines for comprehensive medical care of patients with obesity[J]. Chin J Diab, 2017, 25(1): 10-13. DOI:10.3969/j.issn.1006-6187.2017.01.003 |
| [34] |
Yang GH, Kong LZ, Zhao WH, et al. Emergence of chronic non-communicable diseases in China[J]. Lancet, 2008, 372(9650): 1697-1705. DOI:10.1016/S0140-6736(08)61366-5 |