 2018, Vol. 39
2018, Vol. 39文章信息
- 刘曙正, 郭兰伟, 曹小琴, 陈琼, 张韶凯, 张萌, 于达, 全培良, 孙喜斌, 陈万青.
- Liu Shuzheng, Guo Lanwei, Cao Xiaoqin, Chen Qiong, Zhang Shaokai, Zhang Meng, Yu Da, Quan Peiliang, Sun Xibin, Chen Wanqing.
- 中国2014年肾癌发病与死亡分析
- Estimation on the incidence and mortality of kidney cancer in China, in 2014
- 中华流行病学杂志, 2018, 39(10): 1346-1350
- Chinese Journal of Epidemiology, 2018, 39(10): 1346-1350
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.10.011
-
文章历史
收稿日期: 2018-04-19




2. 100021 北京, 国家癌症中心 中国医学科学院北京协和医学院肿瘤医院早诊早治办公室
2. Office of Cancer Screening, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union College, Beijing 100021, China
全国肿瘤登记中心每年收集居民恶性肿瘤发病、死亡情况和生存状态等信息,监测恶性肿瘤的时间变化趋势以及在不同地区和人群中的分布特征,为制订恶性肿瘤控制计划、评估防治效果、分配卫生资源以及临床、流行病学和卫生服务研究提供不可或缺的理论依据。本研究对中国2014年肾癌资料进行分析。
资料与方法1.资料来源:来自全国肿瘤登记中心449个肿瘤登记处上报的2014年肿瘤登记资料,登记处分布在31个省(自治区、直辖市),其中地级以上城市160个(城市地区),县和县级市289个(农村地区)。提取国际疾病分类(ICD)-10编码为C64的肾癌数据进行分析。人口数据资料参照文献[1]。质量评价:全国肿瘤登记中心根据《中国肿瘤登记工作指导手册》[2]以及国际癌症研究中心和国际癌症登记协会发布的《五大洲癌症发病率》第9卷[3]对登记质量的有关要求,对全国各登记处上报的数据进行审核与评价。通过病理诊断比例、只有死亡证明书比例、死亡发病比、不明诊断比例等主要指标,评价资料的可靠性、完整性、有效性和时效性。最终纳入339个肿瘤登记处的肾癌数据进行分析。
2.统计学分析:应用2014年全国人口数,结合2014年全国肿瘤登记地区分城乡和年龄别的肾癌发病率、死亡率,估计全国2014年肾癌发病和死亡情况。采用Excel 2010和SAS 9.3软件计算发病(死亡)率、年龄别发病(死亡)率、构成比、0~74岁累积率、35~64岁截缩率,并计算中国人口标化率(中标率)和世界人口标化率(世标率)等指标。中标率采用2000年全国普查标准人口年龄构成,世标率采用Segi’s世界标准人口年龄构成。
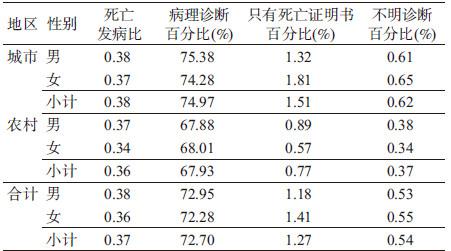
结果1.一般情况:339个登记处(包括地级以上城市129个,县和县级市210个)的数据符合入选标准,覆盖人口共288 243 347人,占全国2014年年末人口数的21.07%。其中城市人口144 061 915人(49.98%),农村144 181 432人(50.02%)。2014年全国肿瘤登记地区肾癌的病理诊断比例为72.70%,只有死亡证明书比例为1.27%,死亡发病比为0.37,不明诊断比例为0.54%(表 1)。
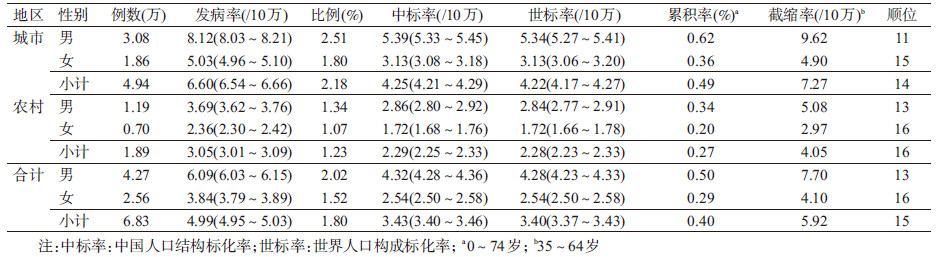
2. 2014年全国肾癌发病情况估计:2014年全国肾癌新发病例数为6.83万例,占全部恶性肿瘤发病的1.80%,位居全部恶性肿瘤发病第15位。肾癌发病率为4.99/10万(95%CI:4.95/10万~5.03/10万),中标发病率为3.43/10万(95%CI:3.40/10万~3.46/10万),世标发病率为3.40/10万(95%CI:3.37/10万~3.43/10万),累积发病率(0~74岁)为0.40%,截缩发病率(35~64岁)为5.92/10万。男性肾癌发病率为6.09/10万(95%CI:6.03/10万~6.15/10万),中标发病率为4.32/10万(95%CI:4.28/10万~4.36/10万),世标发病率为4.28/10万(95%CI:4.23/10万~4.33/10万);女性肾癌发病率为3.84/10万(95%CI:3.79/10万~3.89/10万),中标发病率为2.54/10万(95%CI:2.50/10万~2.58/10万),世标发病率为2.54/10万(95%CI:2.50/10万~2.58/10万)。城市地区肾癌发病率为6.60/10万(95%CI:6.54/10万~6.66/10万),中标发病率为4.25/10万(95%CI:4.21/10万~4.29/10万),世标发病率为4.22/10万(95%CI:4.17/10万~4.27/10万);农村地区发病率为3.05/10万(95%CI:3.01/10万~3.09/10万),中标发病率为2.29/10万(95%CI:2.25/10万~2.33/10万),世标发病率为2.28/10万(95%CI:2.23/10万~2.33/10万)。男性和城市地区的发病率、中标发病率和世标发病率分别高于女性和农村地区(表 2)。
我国肾癌发病率在0~34岁处于较低水平,自35岁后开始上升,男性与女性、城市与农村地区的发病率变化趋势相近,75~79岁年龄组达到峰值,80岁以后开始下降(图 1)。30岁以后男性的年龄别发病率均高于女性,30岁男性年龄别发病率为1.31/10万(95%CI:1.21/10万~1.41/10万),女性为0.59/10万(95%CI:0.52/10万~0.66/10万)。25岁以后城市地区的年龄别发病率均高于农村,25岁城市年龄别发病率为0.45/10万(95%CI:0.40/10万~0.50/10万),农村为0.25/10万(95%CI:0.21/10万~0.29/10万)。

|
| 图 1 2014年中国肾癌的年龄别发病趋势 |
3. 2014年全国肾癌死亡情况估计:据估计,2014年全国肾癌死亡病例为2.56万例,肾癌占全部恶性肿瘤死亡的1.11%,位居全部恶性肿瘤死亡第15位。肾癌死亡率为1.87/10万(95%CI:1.85/10万~1.89/10万),中标死亡率为1.16/10万(95%CI:1.14/10~1.18/10万),世标死亡率为1.16/10万(95%CI:1.14/10万~1.18/10万),累积死亡率(0~74岁)为0.12%,截缩死亡率(35~64岁)为1.36/10万。男性肾癌死亡率为2.31/10万(95%CI:2.27/10万~2.35/10万),中标死亡率为1.52/10万(95%CI:1.50/10万~1.54/10万),世标死亡率为1.53/10万(95%CI:1.51/10万~1.55/10万);女性肾癌死亡率为1.41/10万(95%CI:1.38/10万~1.44/10万),中标死亡率为0.81/10万(95%CI:0.79/10万~0.83/10万),世标死亡率为0.81/10万(95%CI:0.79/10万~0.83/10万)。城市地区肾癌死亡率为2.49/10万(95%CI:2.45/10万~2.53/10万),中标死亡率为1.42/10万(95%CI:1.40/10万~1.44/10万),世标死亡率为1.42/10万(95%CI:1.40/10万~1.44/10万);农村地区死亡率为1.12/10万(95%CI:1.09/10万~1.15/10万),中标死亡率为0.78/10万(95%CI:0.76/10万~0.80/10万),世标死亡率为0.79/10万(95%CI:0.77/10万~0.81/10万)。男性和城市地区肾癌的死亡率、中标死亡率和世标死亡率分别高于女性和农村地区(表 3)。

肾癌年龄别死亡率在40岁以前处于较低水平,40~44岁年龄组开始随年龄增加而增加,除农村女性在80~84岁年龄组达到峰值外,城市地区和农村男性均在85岁以上年龄组达到峰值(图 2)。35岁以后男性的年龄别死亡率均高于女性,35岁男性年龄别死亡率为0.29/10万(95%CI:0.24/10万~0.34/10万),女性为0.18/10万(95%CI:0.14/10万~0.22/10万)。45岁以后城市地区的年龄别死亡率均高于农村,45岁城市年龄别死亡率为0.87/10万(95%CI:0.80/10万~0.94/10万),农村为0.56/10万(95%CI:0.50/10万~0.62/10万)。

|
| 图 2 2014年中国肾癌的年龄别死亡趋势 |
与其他国家和地区相比,我国肾癌发病率高于发展中国家,低于全球和发达国家平均水平。北美地区、澳大利亚/新西兰和欧洲地区有全球最高的肾癌发病率(男性发病率>10/10万,女性>5/10万),而在非洲地区、大平洋岛国肾癌发病率最低(<1.5/10万)[4]。
近年来我国泌尿系统癌症发病率呈现上升趋势,城市地区更加明显[5]。肾癌是泌尿系统中最常见的恶性肿瘤,占全部泌尿系统恶性肿瘤的77.24%[5]。与1998-2002年相比,2014年全国肾癌发病率上升了62.7%[6]。1973-1999年上海市肾癌男性发病率年均变化率为5.30%、女性为4.58%[7]。近年来,随着影像学检查如超声、CT和核磁共振的普及,肾癌诊断水平得到了提高,更多的早期肾癌被发现[8]。但这只是肾癌发病率上升的部分原因,人群中肾癌危险因素暴露水平的改变也对肾癌发病率产生巨大影响[9-10]。
肾癌病因十分复杂,相关文献表明,吸烟、高血压和肥胖是最重要的三大危险因素[11]。曾经吸烟者发生肾癌的风险是非吸烟者的1.38倍[12]。挪威18年随访队列表明SBP在130~、150~和≥170 mmHg(1 mmHg=0.133 kPa)发生肾癌的风险是<130 mmHg基线人群的1.7、2.0和2.0倍[13]。有研究表明BMI每增加1个单位,肾癌的风险增加1.07倍[14]。随着社会经济的发展、城市化、工业化进程的加剧以及饮食习惯及生活方式的改变,我国人群的肾癌危险因素暴露水平逐年上升。1980-2000年全球烟草消费量除美洲地区和欧洲地区下降了27%和2%以外,其他地区均呈上升趋势,其中以我国的烟草消费上升最快[15]。1958-1959、1979-1980、1991和2002年4次全国高血压抽样调查得到的≥15岁人群高血压患病率依次为5.1%、7.7%、13.6%和17.6%,在进行必要的调查和标化处理后,升高趋势依然存在[16]。1982年我国人群中的超重和肥胖还很罕见,分别为6%和0.6%,而2014年人群中超重率达到34.26%,肥胖率为10.98%[16]。上述因素可能与肾癌发病率升高有关。
综上所述,我国肾癌发病死亡水平较低,但较以往有巨大上升,城市男性为重点防控对象。全国范围高质量的肿瘤登记数据为肾癌防控策略的制订提供了数据支持。
利益冲突: 无
| [1] |
Chen WQ, Sun KX, Zheng RS, et al. Cancer incidence and mortality in China, 2014[J]. Chin J Cancer Res, 2018, 30(1): 1-12. DOI:10.21147/j.issn.1000-9604.2018.01.01 |
| [2] |
国家癌症中心. 中国肿瘤登记工作指导手册(2016)[M]. 北京: 人民卫生出版社, 2016: 1-482. National Cancer Center. Chinese guideline for cancer registration (2016)[M]. Beijing: People's Medical Publishing House, 2016: 1-482. |
| [3] |
Curado MJP, Edwards BJ, Shin HR, et al. Cancer incidence in five continents. Volume Ⅸ[R]. IARC Scientific Publication NO. 160. Lyon: IARC Scientific Publication, 2008: 1-837.
|
| [4] |
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide:sources, methods and major patterns in GLOBOCAN 2012[J]. Int J Cancer, 2015, 136(5): E359-386. DOI:10.1002/ijc.29210 |
| [5] |
张永贞, 杨国庆, 王新正, 等. 2003-2007年中国肾及泌尿系统其他癌发病分析[J]. 中国肿瘤, 2012, 21(8): 561-565. Zhang YZ, Yang GQ, Wang XZ, et al. An analysis of incidence of kidney cancer and unspecified urinary organs cancer in China, 2003-2007[J]. China Cancer, 2012, 21(8): 561-565. |
| [6] |
马建辉, 李鸣, 张思维, 等. 中国部分市县肾癌及泌尿系统其他恶性肿瘤发病趋势比较研究[J]. 中华泌尿外科杂志, 2009, 30(8): 511-514. Ma JH, Li M, Zhang SW, et al. Renal cancer incidence trends of cities and counties in China[J]. Chin J Urol, 2009, 30(8): 511-514. DOI:10.3760/cma.j.issn.1000-6702.2009.08.002 |
| [7] |
张薇, 项永兵, 刘振伟, 等. 上海市区老年人泌尿系统常见恶性肿瘤发病趋势分析(1973-1999)[J]. 癌症, 2004, 23(5): 555-558. Zhang W, Xiang YB, Liu ZW, et al. Trends analysis of common urologic neoplasm incidence of elderly people in Shanghai, 1973-1999[J]. Chin J Cancer, 2004, 23(5): 555-558. DOI:10.3969/j.issn.1000-467X.2004.05.015 |
| [8] |
Bai T, Wang L, Wang DW, et al. Clinicopathologica epidemiological characteristics and change tendencies of renal cell carcinoma in Shanxi Province of China from 2005 to 2014[J]. PLoS One, 2015, 10(12): e0144246. DOI:10.1371/journal.pone.0144246 |
| [9] |
de P, Otterstatter MC, Semenciw R, et al. Trends in incidence, mortality, and survival for kidney cancer in Canada, 1986-2007[J]. Cancer Causes Control, 2014, 25(10): 1271-1281. DOI:10.1007/s10552-014-0427-x |
| [10] |
Chow WH, Devesa SS, Warren JL, et al. Rising incidence of renal cell cancer in the United States[J]. JAMA, 1999, 281(17): 1628-1631. DOI:10.1001/jama.281.17.1628 |
| [11] |
Kabaria R, Klaassen Z, Terris MK. Renal cell carcinoma:links and risks[J]. Int J Nephrol Renovasc Dis, 2016, 9: 45-52. DOI:10.2147/IJNRD.S75916 |
| [12] |
Hunt JD, van der Hel OL, McMillan GP, et al. Renal cell carcinoma in relation to cigarette smoking:meta-analysis of 24 studies[J]. Int J Cancer, 2005, 114(1): 101-108. DOI:10.1002/ijc.20618 |
| [13] |
Vatten LJ, Trichopoulos D, Holmen J, et al. Blood pressure and renal cancer risk:the HUNT study in Norway[J]. Br J Cancer, 2007, 97(1): 112-114. DOI:10.1038/sj.bjc.6603823 |
| [14] |
Bergström A, Hsieh CC, Lindblad P, et al. Obesity and renal cell cancer-a quantitative review[J]. Br J Cancer, 2001, 85(7): 984-990. DOI:10.1054/bjoc.2001.2040 |
| [15] |
杨功焕, 马杰民, 刘娜, 等. 中国人群2002年吸烟和被动吸烟的现状调查[J]. 中华流行病学杂志, 2005, 26(2): 77-83. Yang GH, Ma JM, Liu N, et al. Smoking and passive smoking in Chinese, 2002[J]. Chin J Epidemiol, 2005, 26(2): 77-83. DOI:10.3760/j.issn:0254-6450.2005.02.001 |
| [16] |
李立明, 饶克勤, 孔灵芝, 等. 中国居民2002年营养与健康状况调查[J]. 中华流行病学杂志, 2005, 26(7): 478-484. Li LM, Rao KQ, Kong LZ, et al. A description on the Chinese national nutrition and health survey in 2002[J]. Chin J Epidemiol, 2005, 26(7): 478-484. DOI:10.3760/j.issn:0254-6450.2005.07.004 |