 2018, Vol. 39
2018, Vol. 39文章信息
- 于佳, 张涛, 王胤, 高君玫, 华军, 田健美, 丁云芳, 张钧, 陈立凌, 李健琴, 赵根明.
- Yu Jia, Zhang Tao, Wang Yin, Gao Junmei, Hua Jun, Tian Jianmei, Ding Yunfang, Zhang Jun, Chen Liling, Li Jianqin, Zhao Genming.
- 苏州市2011-2017年5岁以下儿童流感门诊病例临床特征及疾病负担
- Clinical characteristics and economic burden of influenza among children under 5 years old, in Suzhou, 2011-2017
- 中华流行病学杂志, 2018, 39(6): 847-851
- Chinese Journal of Epidemiology, 2018, 39(6): 847-851
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.06.029
-
文章历史
收稿日期: 2017-10-09




2. 215003 苏州大学附属儿童医院;
3. 215000 苏州市疾病预防控制中心
2. Soochow University Affiliated Children's Hospital, Suzhou 215003, China;
3. Suzhou Center for Disease Control and Prevention, Suzhou 215000, China
流行性感冒(流感)病毒对全人群均有易感性,但<5岁儿童更是流感流行季节的主要易感人群和传播者。季节性流感除了会导致劳动力的损失,同时也对社会造成了巨大的经济负担。不同流感病毒亚型对于儿童可产生不同的临床症状,最终导致的疾病严重程度也不同。研究发现感染A型流感的儿童和感染B型流感的儿童的临床症状并无差异[1-5];但也有研究认为B型流感阳性者更有可能发生扁桃腺炎及严重的肺炎[6-7];而有研究发现,相比B型流感,A型流感阳性者的住院率及死亡率都更高[8]。尽管国内已有多项针对季节性流感疾病负担的研究[9-13],但鲜有针对儿童感染不同流感亚型造成的疾病负担分析。为此本研究在2011-2017年流感流行季节调查苏州儿童医院就诊的<5岁流感样病例(ILI)不同流感病毒亚型(A/H1N1、A/H3N2和B型)的临床症状和疾病负担。
对象与方法1.研究对象:2011年3月1日至2017年2月28日于苏州大学附属儿童医院门诊就诊的<5岁ILI。根据WHO定义[14],ILI是指发热(体温≥38 ℃),伴咳嗽或咽痛之一,且缺乏其他实验室确定诊断依据者。为此在获得知情同意后,选择发热<3 d的<5岁ILI儿童为研究对象,并采集咽拭子标本。
2.研究方法:利用自行设计的专业问卷收集研究对象的一般情况,包括性别、年龄、临床特征(发热时间、热峰值、咳嗽、流涕等),利用专业问卷询问临床信息包括喘息、腹泻、抽搐等全身症状以及其他并发症等,通过电话随访告知家长或儿童监护人其流感病毒检测结果。ILI就诊时采集咽拭子并放入含病毒采样液的采样管内,保存于4 ℃(不超过4 h)或-80 ℃的冰箱内,每周二和四将样本冷链送至苏州市CDC流感监测网络实验室,采用实时荧光定量RT-PCR进行流感病毒核酸检测。流感发病经济负担包括直接费用(挂号费、检验费、材料费、药费、治疗费、检查费等)和间接费用(就诊造成的交通费、医疗保健品等非医疗费用以及家长误工费),分别通过医院信息系统和电话随访调查患儿家长获得。
3.统计学分析:运用SPSS 22.0软件对相应资料进行统计描述。根据全国流感监测方案(2010年版),将流感监测结果分为阳性组和阴性组,并根据流感病毒亚型将流感阳性者分为H1N1组、H3N2组和B组,不包含其他亚型。计量资料以x±s(或95%CI)表示,计数资料以百分比以及95%CI表示。进行组间比较时,对于计量资料,采用独立样本t检验、Mann-Whitney U检验或Kruskal-Wallis检验;对于计数资料采用χ2检验或者Fisher确切概率法,P<0.05为差异有统计学意义。
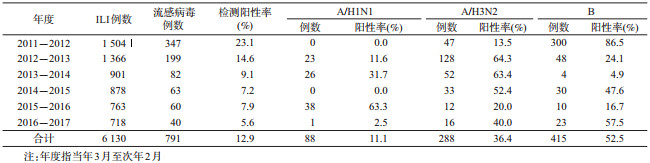
结果1.一般特征:纳入的6 130例ILI全部采样检测,其中791例(12.9%)流感病毒阳性[A/H1N1共88例(11.1%),A/H3N2共288例(36.4%),B型415例(52.5%)]。见表 1。ILI男性460例(58.2%),女性331例(41.8%),流感病毒阳性组的性别比例与阴性组的差异无统计学意义。男性感染不同流感病毒亚型的比例均高于女性,但差异并无统计学意义。<6月龄组感染A/H1N1亚型的比例(1.1%)在各年龄组中最低,而>2岁组的比例(59.1%)最高,其年龄构成大于感染另2种流感病毒亚型的儿童(χ2=10.332,P=0.035)。ILI以本地户籍儿童为主,尤其是流感病毒阳性组该比例更高(χ2=7.055,P=0.008),而对于不同流感病毒亚型,儿童户籍所在地的差异无统计学意义(表 2)。

2.临床特征:ILI中流感病毒阳性病例出现高热的比例高于阴性病例。此外常见的临床症状还有咽红、咳嗽、流涕、气促、喘息、呕吐、抽搐等,其中流感病毒阳性者发生咳嗽(χ2=41.213,P<0.001)、流涕(χ2=12.512,P<0.001)、喘息(χ2=7.579,P=0.006)、呕吐(χ2=4.102,P=0.045)、抽搐(χ2=10.165,P=0.001)的比例均高于阴性者。流感病毒3种亚型(A/H1N1、A/H3N2、B)的临床特征主要差异在于咳嗽(χ2=9.227,P=0.010)、喘息(χ2=7.273,P=0.026)和呕吐(χ2=8.163,P=0.017)的发生比例,其他临床症状在感染亚型间的差异无统计学意义。
流感病毒阳性病例发生早产的比例略低于阴性病例(χ2=4.701,P=0.030)。流感病毒A/H1N1阳性的病例其婴儿湿疹病史(χ2=11.056,P=0.004)、应用免疫抑制药物史(χ2=23.385,P<0.001)和过去1个月前呼吸道疾病史(χ2=9.576,P=0.008)的比例均明显高于其他两组亚型,差异有统计学意义(表 2)。
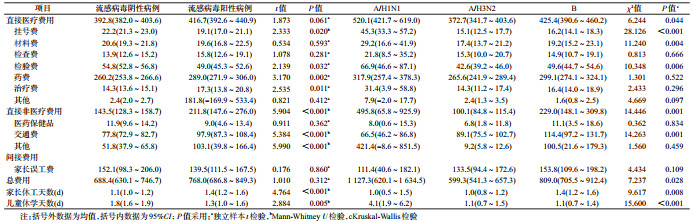
3.疾病负担:流感病毒阴性病例平均总费用为688.4(95%CI:630.1~746.7)元,阳性病例为768.0(95%CI:686.8~849.3)元。流感病毒阳性病例中,A/H1N1亚型感染者平均费用为1 127.3(95%CI:620.1~1 634.5)元,A/H3N2亚型感染者平均费用为599.3(95%CI:541.3~657.3)元,B型感染者平均费用为809.0(95%CI:705.5~912.4)元。A/H1N1亚型阳性者的总费用明显高于其他两型(χ2=7.237,P=0.028)。在直接医疗费用中,流感病毒阳性病例的药费(t=3.170,P=0.002)、治疗费(t=2.535,P=0.011)明显高于阴性病例,但后者在挂号费(t=2.333,P=0.020)、检验费(t=2.139,P=0.032)却略高。A/H1N1亚型阳性病例的挂号费(χ2=28.126,P<0.001)、材料费(χ2=11.240,P=0.004)、检验费(χ2=10.348,P=0.006)平均费用明显高于另两亚型阳性病例。流感病毒阳性病例在医药保健品、交通等直接非医疗费用的支出,明显高于流感病毒阴性病例(χ2=5.904,P<0.001),其中A/H1N1亚型阳性病例的直接非医疗平均费用则是另两亚型病例的2~4倍。流感病毒阳性儿童导致家长误工天数明显多于阴性儿童(χ2=4.764,P<0.001),差异无统计学意义。其中感染流感B亚型的儿童家长因本次疾病导致休工的天数长于另两亚型(χ2=9.617,P=0.008)。流感病毒阳性儿童休学天数少于阴性儿童(χ2=2.844,P=0.005),其中A/H1N1阳性者休学天数平均为4.1 d,而感染另两亚型者则为1.1 d,差异有统计学意义(χ2=15.600,P<0.001)。见表 3。
本研究显示,ILI中流感病毒阳性病例出现高热(体温>39 ℃)的比例明显高于阴性者,与文献报道一致[15]。且这些病例发生咳嗽、流涕、喘息、呕吐、抽搐的比例均高。在芬兰、美国等研究显示,感染不同亚型流感病毒的儿童其临床症状并无明显差异[3, 16],但本研究中,相比A/H3N2和B亚型病例,感染A/H1N1亚型者更易发生咳嗽,而感染B型流感者更多发生喘息症状,同时发生呕吐的比例高于其他亚型病例,与以往研究发现流感B型感染者比A型感染者更容易发生消化道症状的结果相似[4, 17]。本研究还发现A/H1N1阳性儿童存在婴儿湿疹史、免疫抑制药物使用史和1个月前呼吸道疾病史的比例明显高于其他流感亚型阳性者。
已有研究发现,<5岁儿童感染流感病毒后会对其家庭和社会造成严重的经济负担[18]。2011-2012年一项针对苏州市<5岁ILI的调查发现,流感病毒阳性、阴性儿童因疾病产生的平均总费用分别为127.2元和128.1元[13];而上海市一项针对确诊流感病例的研究发现[19],每例流感患儿总平均费用为999.90元,均略高于本研究所得的总费用。流感病毒阳性儿童的直接医疗费用和直接非医疗费用明显高于流感病毒阴性儿童,其中感染A/H1N1亚型者的费用更高。本研究中流感病毒阳性儿童的家长误工时间明显长于阴性者,与国外同类研究结果一致[20]。但本研究的间接医疗费用远低于直接费用,而国外研究的间接医疗费用在总费用中占据相当大的比例[20-22]。而儿童医疗保险覆盖情况、家长就业、家庭中是否有祖辈或全职家长照顾儿童等因素可能造成费用构成上的差异。研究中发现,感染A/H1N1亚型的儿童因流感平均缺课达到4.1 d,是A/H3N2和B亚型阳性儿童的4倍。我国一项10省(市)流感监测发现[23],<6月龄是流感病毒感染的保护因素,年龄越小感染流感病毒的风险越小。本研究也发现>2岁儿童流感病毒阳性的比例明显高于<2岁儿童。
本研究存在局限性。如分析的ILI监测资料只来自一家医院,不能代表整个苏州市;随访调查是通过电话询问由家长自报,可能存在回忆偏倚;调查中缺少与ILI相关其他呼吸道病毒检测结果以及抗生素治疗等相关信息。
利益冲突: 无
| [1] | Mancinelli L, Onori M, Concato C, et al. Clinical features of children hospitalized with influenza A and B infections during the 2012-2013 influenza season in Italy[J]. BMC Infect Dis, 2016, 16: 6. DOI:10.1186/s12879-015-1333-x |
| [2] | Gubbels S, Krause TG, Bragstad K, et al. Burden and characteristics of influenza A and B in Danish intensive care units during the 2009/10 and 2010/11 influenza seasons[J]. Epidemiol Infect, 2013, 141(4): 767–775. DOI:10.1017/S0950268812001471 |
| [3] | Silvennoinen H, Peltola V, Lehtinen P, et al. Clinical presentation of influenza in unselected children treated as outpatients[J]. Pediatr Infect Dis J, 2009, 28(5): 372–375. DOI:10.1097/INF.0b013e318191eef7 |
| [4] | Hong KW, Cheong HJ, Song JY, et al. Clinical manifestations of influenza A and B in children and adults at a tertiary hospital in Korea during the 2011-2012 season[J]. Jpn J Infect Dis, 2015, 68(1): 20–26. DOI:10.7883/yoken.JJID.2013.466 |
| [5] | Guan WD, Gong XY, Mok CKP, et al. Surveillance for seasonal influenza virus prevalence in hospitalized children with lower respiratory tract infection in Guangzhou, China during the post-pandemic era[J]. PLoS One, 2015, 10(4): e0120983. DOI:10.1371/journal.pone.0120983 |
| [6] | Chi CY, Wang SM, Lin CC, et al. Clinical features of children infected with different strains of influenza B in southern Taiwan[J]. Pediatr Infect Dis J, 2008, 27(7): 640–645. DOI:10.1097/INF.0b013e31816be008 |
| [7] | Esposito S, Molteni CG, Daleno C, et al. Clinical and socioeconomic impact of different types and subtypes of seasonal influenza viruses in children during influenza seasons 2007/2008 and 2008/2009[J]. BMC Infect Dis, 2011, 11(1): 271. DOI:10.1186/1471-2334-11-271 |
| [8] | Chiu SS, Chan KH, So LY, et al. The population based socioeconomic burden of pediatric influenza-associated hospitalization in Hong Kong[J]. Vaccine, 2012, 30(10): 1895–1900. DOI:10.1016/j.vaccine.2011.12.027 |
| [9] | Guo RN, Zheng HZ, Huang LQ, et al. Epidemiologic and economic burden of influenza in the outpatient setting:a prospective study in a subtropical area of China[J]. PLoS One, 2012, 7(7): e41403. DOI:10.1371/journal.pone.0041403 |
| [10] | Guo RN, Zheng HZ, Li JS, et al. A population-based study on incidence and economic burden of influenza-like illness in south China, 2007[J]. Public Health, 2011, 125(6): 389–395. DOI:10.1016/j.puhe.2011.03.004 |
| [11] | Zhou L, Situ S, Huang T, et al. Direct medical cost of influenza-related hospitalizations among severe acute respiratory infections cases in three provinces in China[J]. PLoS One, 2013, 8(5): e63788. DOI:10.1371/journal.pone.0063788 |
| [12] | Yang J, Jit M, Leung KS, et al. The economic burden of influenza-associated outpatient visits and hospitalizations in China:a retrospective survey[J]. Infect Dis Poverty, 2015, 4(1): 44. DOI:10.1186/s40249-015-0077-6 |
| [13] | Wang D, Zhang T, Wu J, et al. Socio-economic burden of influenza among children younger than 5 years in the outpatient setting in Suzhou, China[J]. PLoS One, 2013, 8(8): e69035. DOI:10.1371/journal.pone.0069035 |
| [14] | World Health Organization. WHO surveillance case definitions for ILI and SARI[EB/OL]. (2014-01)[2017-03]. http://www.who.int/influenza/surveillance_monitoring/ili_sari_surveillance_case_definition/en/. |
| [15] | Fu Y, Pan L, Sun Q, et al. The clinical and etiological characteristics of influenza-like illness (ILI) in outpatients in Shanghai, China, 2011 to 2013[J]. PLoS One, 2015, 10(3): e0119513. DOI:10.1371/journal.pone.0119513 |
| [16] | Irving SA, Patel DC, Kieke BA, et al. Comparison of clinical features and outcomes of medically attended influenza A and influenza B in a defined population over four seasons:2004-2005 through 2007-2008[J]. Influenza Other Respir Viruses, 2012, 6(1): 37–43. DOI:10.1111/j.1750-2659.2011.00263.x |
| [17] | Kaji M, Watanabe A, Aizawa H. Differences in clinical features between influenza A H1N1, A H3N2, and B in adult patients[J]. Respirology, 2003, 8(2): 231–233. DOI:10.1046/j.1440-1843.2003.00457.x |
| [18] | Antonova EN, Rycroft CE, Ambrose CS, et al. Burden of paediatric influenza in Western Europe:a systematic review[J]. BMC Public Health, 2012, 12(1): 968–983. DOI:10.1186/1471-2458-12-968 |
| [19] |
王相诗, 蔡洁皓, 姚玮蕾, 等. 上海地区某医院门诊儿童流感社会经济负担调查[J]. 中华流行病学杂志, 2015, 36(1): 27–30.
Wang XS, Cai JH, Yao WL, et al. Socio-economic impact of influenza in children:a single-centered hospital study in Shanghai[J]. Chin J Epidemiol, 2015, 36(1): 27–30. DOI:10.3760/cma.j.issn.0254-6450.2015.01.007 |
| [20] | Esposito S, Cantarutti L, Molteni CG, et al. Clinical manifestations and socio-economic impact of influenza among healthy children in the community[J]. J Infect, 2011, 62(5): 379–387. DOI:10.1016/j.jinf.2011.02.015 |
| [21] | Li S, Leader S. Economic burden and absenteeism from influenza-like illness in healthy households with children (5-17 years) in the US[J]. Respir Med, 2007, 101(6): 1244–1250. DOI:10.1016/j.rmed.2006.10.022 |
| [22] | Keech M, Beardsworth P. The impact of influenza on working days lost:a review of the literature[J]. Pharmaco Economics, 2008, 26(11): 911–924. DOI:10.2165/00019053-200826110-00004 |
| [23] |
彭质斌, 许军, 余昭, 等. 中国10省(市)2009-2014年15岁以下儿童流感确诊住院病例严重急性呼吸道感染临床特征及其危险因素分析[J]. 中华流行病学杂志, 2015, 36(3): 210–215.
Peng ZB, Xu J, Yu Z, et al. Clinical characteristics of hospitalized cases of severe acute respiratory infection with laboratory-confirmed influenza and the risk factors analysis of influenza infection for children under 15 years old in ten provinces in China during 2009-2014[J]. Chin J Epidemiol, 2015, 36(3): 210–215. DOI:10.3760/cma.j.issn.0254-6450.2015.03.005 |