 2018, Vol. 39
2018, Vol. 39文章信息
- 申嘉欣, 郭玲玲, 汝首杭, 王颖, 李玫, 邬惟为, 冯永亮, 张萍, 杨海澜, 王素萍, 张亚玮.
- Shen Jiaxin, Guo Lingling, Ru Shouhang, Wang Ying, Li Mei, Wu Weiwei, Feng Yongliang, Zhang Ping, Yang Hailan, Wang Suping, Zhang Yawei.
- 膳食胆固醇摄入对妊娠期糖尿病的影响
- Interaction between dietary cholesterol intake and the risk of gestational diabetes mellitus
- 中华流行病学杂志, 2018, 39(6): 830-835
- Chinese Journal of Epidemiology, 2018, 39(6): 830-835
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.06.026
-
文章历史
收稿日期: 2017-11-03




2. 030001 太原, 山西医科大学附属第一医院妇产科;
3. 06520 美国康涅狄格州纽黑文市, 美国耶鲁大学公共卫生学院环境健康科学系
2. Obstetrics and Gynecology, First Affiliated Hospital of Shanxi Medical University, Taiyuan 030001, China;
3. Division of Environmental Health Sciences, School of Public Health, Yale University, New Haven, Connecticut 06520, USA
妊娠期糖尿病(gestational diabetes mellitus,GDM)指妊娠前糖代谢正常,妊娠期才出现的糖尿病,是由妊娠诱发的暂时性糖尿病[1]。国际糖尿病联合会(International Diabetes Federation,IDF)数据显示,2013年中国患GDM的孕妇超过100万,排名世界第二[2]。GDM可对孕妇及胎儿造成不同程度的不良影响[3-4],有研究认为,GDM的发生机制与2型糖尿病相似,主要表现为胰岛素抵抗[5],且已有大量研究证实,膳食高胆固醇摄入引起胰岛素抵抗会增加2型糖尿病的患病风险[6]。国外学者对孕妇孕前及孕期膳食胆固醇摄入进行分析后,认为胆固醇摄入也可能与GDM发生有关[7-8],但由于孕前及孕期各阶段孕妇体内胆固醇代谢机制不同[9],不同阶段胆固醇摄入量对GDM影响不一,但未有研究探讨各个阶段胆固醇摄入对GDM发生的影响。本研究将从孕妇孕前1年、孕早期、孕中期膳食胆固醇摄入量的角度,探讨胆固醇摄入与GDM的关系,为制定相应预防策略提供理论依据。
对象与方法1.研究对象:2012年3月至2016年9月在山西医科大学附属第一医院产科住院分娩的孕妇为研究对象。经山西医科大学伦理委员会审查批准,所有研究对象均签署知情同意书。纳入标准:知情同意、自愿参加。排除标准:死胎、死产、双胎、多胎及怀孕前被诊断为糖尿病的孕妇。
2.研究方法:
(1)问卷设计与现场调查:采用标准化的结构式孕期妇女健康调查问卷,由培训合格的调查人员对孕妇进行面对面调查,并查阅相关病历信息。问卷内容包括一般人口学特征、生活方式和可能的混杂因素(包括生育史、病史、围产期保健、职业、吸烟情况及体育活动情况)。
(2)评估胆固醇摄入:采用半定量食物频数表(FFQ)[10],于孕妇分娩后回顾性调查孕妇孕前1年及孕期的饮食情况(主要包括谷物类、肉类、蛋奶类、蔬菜、水果等中国人群日常33种食物),调查内容包括食用量及食用频率,并根据中国食品消费标准将膳食摄入转化为各种营养素的每天摄入量[11],来评估孕妇膳食胆固醇的摄入值,并根据对照组孕妇不同时期胆固醇摄入的P25、P50、P75将其分为Q1~Q4 4组[8, 12]。
(3)诊断标准:参照中国妊娠合并糖尿病防治指南(2014)标准[13]:孕妇于妊娠24~28周进行口服75 g葡萄糖筛查试验(oral glucose tolerance test,OGTT)。诊断标准为FPG≥5.1 mmol/L、餐后1 h≥10 mmol/L、餐后2 h≥8.5 mmol/L,血糖水平达到或超过某一个标准即可诊断为GDM。
(4)鉴于孕妇年龄是影响GDM发生的重要因素,进一步对年龄进行分层分析,分为<35岁和≥35岁[14]。
3.统计学分析:采用EpiData 3.1软件建立数据库并录入问卷,应用SAS 9.3软件进行数据清理及分析。正态分布的计量资料以x±s表示,计数资料以百分比表示。GDM影响因素的单因素分析采用χ2检验,多因素采用非条件logistic回归分析,以P<0.05为差异有统计学意义。
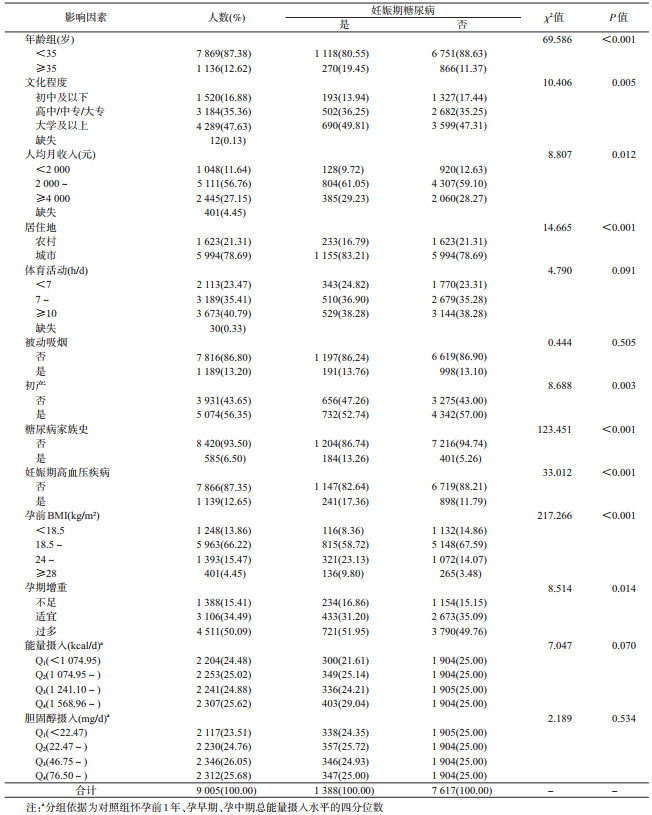
结果1.一般特征:本研究共调查孕妇9 005人,年龄(29.07±4.57)岁,82.99%的孕妇文化程度为高中及以上,家庭人均月收入集中在2 000~4 000元(56.76%)。孕前及孕期胆固醇摄入量为(60.07±52.34)mg/d,孕前1年胆固醇摄入量为(59.90±51.51)mg/d,孕早期胆固醇摄入量为(58.72±51.37)mg/d,孕中期胆固醇摄入量为(60.26±53.88)mg/d。
2. GDM情况及单因素分析:共1 388例孕妇被诊断出患GDM。单因素分析结果显示,孕妇年龄、文化程度、人均月收入、居住地、是否初产、糖尿病家族史、是否患有妊娠期高血压疾病、孕前BMI及孕期增重均与GDM有关,差异有统计学意义(P<0.05)(表 1)。
3.孕妇各阶段胆固醇摄入对GDM发生的多因素分析:单纯调整总能量摄入后未发现胆固醇摄入与GDM发生有关。调整相关混杂因素后,孕前1年、孕中期膳食胆固醇摄入为Q4水平,即胆固醇摄入量≥76.50 mg/d时,会增加孕妇妊娠期糖尿病的发生风险(表 2)。

4.孕前1年及孕中期胆固醇摄入对GDM发生的多因素分析:对孕前期及孕中期胆固醇摄入进行分析发现,以孕前1年及孕中期胆固醇摄入均最低作为对照组,孕前1年胆固醇摄入量≥76.50 mg/d且孕中期膳食胆固醇摄入量≥46.75 mg/d会增加孕妇GDM的患病风险(表 3)。

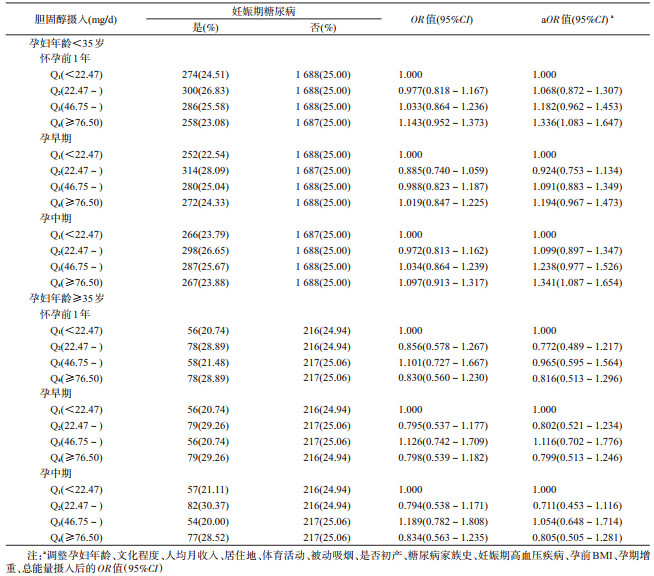
5.不同年龄孕妇各阶段胆固醇摄入对GDM发生的多因素分析:孕妇年龄<35岁时,孕前1年、孕中期胆固醇摄入量≥76.50 mg/d均是GDM的危险因素;孕妇年龄≥35岁组未发现膳食胆固醇摄入与GDM发生有关(表 4)。
已有大量研究证实膳食高胆固醇摄入引起胰岛素抵抗可能导致2型糖尿病的发生[6],GDM的发生机制与2型糖尿病相似,主要表现为胰岛素抵抗[5]。美国一项十年队列研究发现[7],长期的高胆固醇饮食习惯可能会增加怀孕后发生GDM的风险,且胆固醇摄入量与GDM发生风险呈正相关关系(趋势检验P=0.04)。Qiu等[8]将怀孕前3个月及孕早期的总胆固醇摄入量纳入病例对照研究,结果也表明,高胆固醇摄入是GDM发生的危险因素(OR=2.94,95%CI:1.14~7.60)。本研究更加全面、具体地分析了孕前1年、孕早期、孕中期膳食胆固醇摄入量与GDM的发生关系,根据对照组孕妇不同时期胆固醇摄入分组后发现,孕前1年、孕中期膳食胆固醇摄入量≥76.50 mg/d均为GDM的危险因素,未发现孕早期胆固醇摄入与GDM发生有关。这可能是由于怀孕前长期处于高水平胆固醇摄入状态会引起胰岛素抵抗,从而增加孕期患GDM的风险;而怀孕后孕妇新陈代谢加快,一定程度上可减少胰岛素抵抗[15],且随着孕中期孕妇及胎儿的营养需求不断增大,膳食摄入量快速增长,胆固醇摄入增多,发生GDM风险增加。
进一步对孕前1年及孕中期胆固醇摄入水平进行分析发现,孕前1年胆固醇摄入量≥76.50 mg/d且孕中期摄入量≥46.75 mg/d时,孕妇患GDM的风险增加,提示孕妇在孕前1年及孕中期均应减少胆固醇摄入量,降低GDM的发生风险。现有研究表明[16-17],膳食高胆固醇饮食可增加血清胆固醇水平,促进炎症反应,引起代谢紊乱,造成胰岛素抵抗等的发生,提示膳食高胆固醇摄入引起的慢性炎症反应造成的胰岛素抵抗可能是导致GDM的发生的重要机制。
鉴于孕妇年龄对GDM发生的影响较大,且高龄孕妇(孕妇年龄≥35岁)是GDM发生独立危险因素[18]。本研究发现,按年龄分组后,≥35岁组孕妇未发现膳食胆固醇摄入与GDM的发生有关,而<35岁组孕妇中,孕前1年、孕中期胆固醇摄入量≥76.50 mg/d均会增加GDM发生的风险,推测高龄孕妇GDM发生率较高的主要原因可能是年龄增长导致的胰岛素敏感性下降[19]。“二孩”政策调整后,高龄孕妇比例不断上升,其围产期保健与监护日益受到医护人员重视,而本研究结果表明,非高龄组孕妇膳食胆固醇摄入较高与GDM发生有关,提示在关注高龄孕妇膳食的同时,非高龄孕妇也应引起重视,进行合理饮食指导,减少胆固醇摄入量,降低GDM的发生风险。
本研究存在一定局限性。首先,胆固醇摄入量是在孕妇分娩后面对面访谈回顾性调查的,存在潜在的回忆偏倚,可能会低估与GDM发生之间的关联。其次,研究对象均来自医院,研究结果不具有普遍性。
综上所述,孕前1年及孕中期膳食胆固醇摄入量高均可能增加孕期患GDM的风险,提示应在备孕期及孕中期对孕妇进行饮食干预,减少膳食胆固醇摄入量,预防GDM的发生。
利益冲突: 无
| [1] | Diagnostic criteria and classification of hyperglycemia first detected in pregnancy:a World Health Organization guideline[J]. Diabetes Res Clin Pract, 2014, 103(3): 341–363. DOI:10.1016/j.diabres.2013.10.012 |
| [2] | Guariguata L, Linnenkamp U, Beagley J, et al. Global estimates of the prevalence of hyperglycemia in pregnancy[J]. Diabetes Res Clin Pract, 2014, 103(2): 176–185. DOI:10.1016/j.diabres.2013.11.003 |
| [3] | Malcolm J. Through the looking glass:gestational diabetes as a predictor of maternal and offspring long-term health[J]. Diabetes Metab Res Rev, 2012, 28(4): 307–311. DOI:10.1002/dmrr.2275 |
| [4] | Herath H, Herath R, Wickremasinghe R. Gestational diabetes mellitus and risk of type 2 diabetes 10 years after the index pregnancy in Sri Lankan women-a community based retrospective cohort study[J]. PLoS One, 2017, 12(6): e0179647. DOI:10.1371/journal.pone.0179647 |
| [5] | American Diabetes Association. Diagnosis and classification of diabetes mellitus[J]. Diabetes Care, 2013, 36(Suppl 1): S67–74. DOI:10.2337/dc13-s067 |
| [6] | Tajima R, Kodama S, Hirata M, et al. High cholesterol intake is associated with elevated risk of type 2 diabetes mellitus-A Meta-analysis[J]. Clin Nutr, 2014, 33(6): 946–950. DOI:10.1016/j.clnu.2014.03.001 |
| [7] | Bowers K, Tobias DK, Yeung E, et al. A prospective study of pre-pregnancy dietary fat intake and risk of gestational diabetes[J]. Am J Clin Nutr, 2012, 95(2): 446–453. DOI:10.3945/ajcn.111.026294 |
| [8] | Qiu CF, Frederick IO, Zhang CL, et al. Risk of gestational diabetes mellitus in relation to maternal egg and cholesterol intake[J]. Am J Epidemiol, 2011, 173(6): 649–658. DOI:10.1093/aje/kwq425 |
| [9] |
姜殿林, 董桂虎, 徐霞. 正常妊娠妇女血脂及载脂蛋白水平的变化[J]. 实用临床医学, 2006, 7(4): 16–17.
Jiang DL, Dong GH, Xu X. Changes in blood lipid and apolipoprotein levels in normal pregnant women[J]. Pract Clin Med, 2006, 7(4): 16–17. DOI:10.3969/j.issn.1009-8194.2006.04.006 |
| [10] | Wang Y, Zhao N, Qiu J, et al. Folic acid supplementation and dietary folate intake, and risk of preeclampsia[J]. Eur J Clin Nutr, 2015, 69(10): 1145–1150. DOI:10.1038/ejcn.2014.295 |
| [11] |
杨月欣, 王光亚, 潘兴昌. 中国食物成分表 2002[M]. 北京: 北京大学医学出版社, 2002.
Yang YX, Wang GY, Pan XC.China Food Composition 2002[M]. Beijing: Peking University Medical Press, 2002. |
| [12] | Kurotani K, Nanri A, Goto A, et al. Cholesterol and egg intakes and the risk of type 2 diabetes:the Japan Public Health Center-based Prospective Study[J]. Br J Nutr, 2014, 112(10): 1636–1643. DOI:10.1017/s000711451400258x |
| [13] |
中华医学会妇产科学分会产科学组, 中华医学会围产医学分会妊娠合并糖尿病协作组. 妊娠合并糖尿病诊治指南(2014)[J]. 中华妇产科杂志, 2014, 49(8): 561–569.
Obstetrics Department of the Chinese Medical Association of Obstetrics and Gynecology, Chinese Medical Association Perinatal Medical Association, Gestational Diabetes Cooperation Group. The guideline for diagnosis and management of diabetes and pregnancy[J]. Chin J Obstet Gynecol, 2014, 49(8): 561–569. DOI:10.3760/cma.j.issn.0529-567x.2014.08.001 |
| [14] | Lamminpää R, Vehviläinen-Julkunen K, Gissler M, et al. Pregnancy outcomes in women aged 35 years or older with gestational diabetes-a registry-based study in Finland[J]. J Matern Fetal Neonatal Med, 2016, 29(1): 55–59. DOI:10.3109/14767058.2014.986450 |
| [15] | Radesky JS, Oken E, Rifas-Shiman SL, et al. Diet during early pregnancy and development of gestational diabetes[J]. Padiatr Perinat Epidemiol, 2008, 22(1): 47–59. DOI:10.1111/j.1365-3016.2007.00899.x |
| [16] | Khayyatzadeh SS, Kazemi-Bajestani SMR, Bagherniya M, et al. Serum high C reactive protein concentrations are related to the intake of dietary macronutrients and fiber:findings from a large representative Persian population sample[J]. Clin Biochem, 2017, 50(13/14): 750–755. DOI:10.1016/j.clinbiochem.2017.03.016 |
| [17] | Tall AR, Yvan-Charvet L. Cholesterol, inflammation and innate immunity[J]. Nat Rev Immunol, 2015, 15(2): 104–116. DOI:10.1038/nri3793 |
| [18] |
毛雷婧, 葛星, 徐叶清, 等. 孕前体重指数和孕中期体重增加对妊娠期糖尿病发病影响的队列研究[J]. 中华流行病学杂志, 2015, 36(5): 416–420.
Mao LJ, Ge X, Xu YQ, et al. Pregestational body mass index, weight gain during first half of pregnancy and gestational diabetes mellitus:a prospective cohort study[J]. Chin J Epidemiol, 2015, 36(5): 416–420. DOI:10.3760/cma.j.issn.0254-6450.2015.05.002 |
| [19] | Fulop T, Larbi A, Douziech N. Insulin receptor and ageing[J]. Pathol Biol, 2003, 51(10): 574–580. DOI:10.1016/j.patbio.2003.09.007 |