 2018, Vol. 39
2018, Vol. 39文章信息
- 杨帆, 王双, 覃海, 谭柯, 孙倩倩, 王凌霄, 聂双双, 刘佳倪, 陈杨, 张敏, 陈燕语.
- Yang Fan, Wang Shuang, Qin Hai, Tan Ke, Sun Qianqian, Wang Lingxiao, Nie Shuangshuang, Liu Jiani, Chen Yang, Zhang Min, Chen Yanyu.
- 衰弱综合征对社区老年糖尿病患者跌倒影响的队列研究
- Effect of frailty syndrome on falls in Chinese elderly diabetics in the communities: a prospective cohort study
- 中华流行病学杂志, 2018, 39(6): 776-780
- Chinese Journal of Epidemiology, 2018, 39(6): 776-780
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.06.016
-
文章历史
收稿日期: 2017-12-10




2. 610000 成都, 都江堰市平义社区卫生服务中心;
3. 611130 成都市第五人民医院老年科;
4. 266071 青岛大学附属中心医院全科医学科;
5. 610041 成都, 四川大学华西第四医院姑息医学科;
6. 610072 成都, 四川省人民医院老年内分泌科
2. Internal Medicine Department, The Pingyi Community Health Service Center in Dujiangyan City, Chengdu 610000, China;
3. Geriatric Department, The Fifth People's Hospital of Chengdu, Chengdu 611130, China;
4. General Medicine Department, The Affiliated Central Hospital of Qingdao University, Qingdao 266071, China;
5. Department of Palliative Medicine, NO.4 West China Teaching Hospital, Sichuan University, Chengdu 610041, China;
6. Department of Elderly Endocrinology, Sichuan Provincial People's Hospital, Chengdu 610072, China
每年约有1/3的≥65岁社区老年人发生跌倒,其中约1/10的跌倒导致严重的软组织损伤、创伤性脑损伤或骨折[1]。同时,跌倒对心理健康也会造成不良影响,如恐惧跌倒、焦虑和抑郁[2]。糖尿病是一种严重危害人类健康的慢性非传染性疾病,我国≥70岁老年糖尿病患病率高达23.5%[3]。与同龄非糖尿病老年人相比,糖尿病患者的跌倒风险明显增加[1, 4-6]。衰弱综合征是一种常见的老年综合征,目前尚无统一的定义,但国际上基本达成共识,即衰弱综合征由多器官生理系统功能紊乱引起,导致生理储备下降,从而表现出对各种应激原脆弱性增加[7]。据报道,老年糖尿病患者衰弱的发生率约为32%~48%,显著高于非糖尿病老年人(5%~10%)[8]。鉴于糖尿病和衰弱常常并存,且衰弱能够简单量化老年人的整体健康状态,并对不良结局有很强的预测能力,本研究将主要探讨衰弱与老年糖尿病患者未来发生跌倒之间的关系。
对象与方法1.研究对象及队列建立:本研究数据来自“都江堰地区社区老年人口疾病、心理、社会需求状况调查”。研究对象为四川省都江堰市平义社区卫生服务中心管辖小区内≥65岁老年人。排除标准:①任意疾病急性期,如急性心、肝、肾及呼吸衰竭等;②严重视、听力障碍及重度痴呆;③不愿接受调查。从60个小区中随机抽取20个,再采用方便抽样方法抽取调查对象。在与社区居委会协商后,调查员在小区入口处设调查点,进行面对面问卷调查。对于不能来到调查现场的老年人,统一安排调查员入户调查。调查过程中老年人不能理解或表述不清的客观问题,由家属或照料者代为作答。问卷的内容主要包括社会人口特征、工作经验和收入、健康状况、人体测量、危险因素、慢性病患病情况、医疗服务,以及个人幸福和生活质量。2014年1月完成基线调查,共纳入653人有效样本。根据基线记录的联系方式和家庭住址,2017年1月,排除死亡34人、拒访26人、搬家17人、变更联系方式54人及其他(旅游、走亲戚等)49人,共有473名老年人完成第二次评估。
40名统一培训的调查员由四川大学华西临床医学院学工部协助招募。每2名调查员一组对同一对象进行调查。本研究已经通过四川大学伦理委员会的审查,所有受试者均签署了知情同意书。
2.研究内容和方法:
(1)糖尿病:患者报告曾经确诊过糖尿病,或正在使用降糖药物或胰岛素治疗,或正在进行特殊饮食、运动疗法、体重控制等来治疗糖尿病。过往研究显示老年人自报糖尿病能适当估计糖尿病的患病情况[9]。
(2)衰弱综合征:本研究使用的FRAIL量表由国际老年营养学会制定,包含疲劳感、阻力感、自由活动能力下降、多种疾病共存和体重减轻5项,每项1分,累计0分为健壮,1~2分为衰弱前期,3~5分为衰弱[10]。FRAIL量表在中国社区老年人群中有较好的的集合效度(Kappa系数为0.209~0.401,P<0.001)和7~15 d重测信度(相关系数为0.708)[11]。在美国、欧洲、中国香港地区和澳大利亚,该量表被证实是不良健康结局的有效预测因子[12-15]。
(3)跌倒:患者或照料者报告过去3年受试者的跌倒情况。多次跌倒或至少1次受伤性跌倒划分为跌倒组,未曾经历过跌倒或1次未受伤性跌倒划分为无跌倒组。
(4)其他:社会人口学信息包括年龄、性别、文化程度、婚姻状况、烟酒史;老年综合征包括衰弱综合征、视力障碍、认知功能障碍和营养不良;慢性疾病定义为受试者自述曾经诊断过该疾病或正在接受相应治疗,主要包括关节炎、中风、心绞痛、糖尿病、慢性肺病、哮喘、高血压病和口腔疾病。身体测量包括身高和体重,并计算BMI(kg/m2);根据中国肥胖问题工作组(WGOC)建议,将BMI<18.5、18.5~23.9、24.0~27.9和≥28.0分别定义为体重过低、体重正常、超重和肥胖[16]。小学及以下文化程度定义为文盲;已婚或同居定义为有伴侣,未婚、离异或丧偶定义为无伴侣。曾经吸烟或现在吸烟定义为有吸烟史。曾经饮酒或现在饮酒定义为有饮酒史。患者自述视力问题或需要佩戴眼镜定义为视力障碍。采用简易智能量表(mini-mental state examination,MMSE)来评估认知功能。中国版MMSE量表能够有效的调查社区老年人的认知功能状态,并将认知功能障碍定义为初中及以上学历者<24分(灵敏度为100.0%、特异度为71.4%)或小学文化程度者≤20分(灵敏度为75.0%、特异度为74.45)或文盲≤17分(灵敏度为68.9%、特异度为86.6%)[17]。采用简易微型营养评价量表(mini-nutritional assessment short-form,MNA-SF)来评估营养状况,≤12分视为营养不良。MNA-SF的敏感性为85.7%、特异性为96.0%、准确性为87.5%、阳性预测值为99.0%、阴性预测值为58.5% [18]。
3.统计学方法:采用EpiData软件建立数据库并双人背对背录入原始数据。采用SPSS 22.0软件进行统计分析。定量资料采用x±s表示,定性资料采用频数和百分比描述。跌倒组和无跌倒组间基线资料的比较采用t检验或χ2检验。在整体人群、无糖尿病人群和糖尿病人群中,以跌倒为因变量,以年龄、性别、文化程度、婚姻状况、吸烟史、饮酒史、视力障碍、认知功能障碍、营养不良、衰弱状态和口腔疾病为自变量,采用向后逐步法进行logistic回归分析(α入<0.05,α出>0.10),筛选跌倒的独立危险因素;再将有意义的变量纳入多因素logistic回归模型,分析在三组人群中衰弱与跌倒的关系。双侧P<0.05为差异有统计学意义。
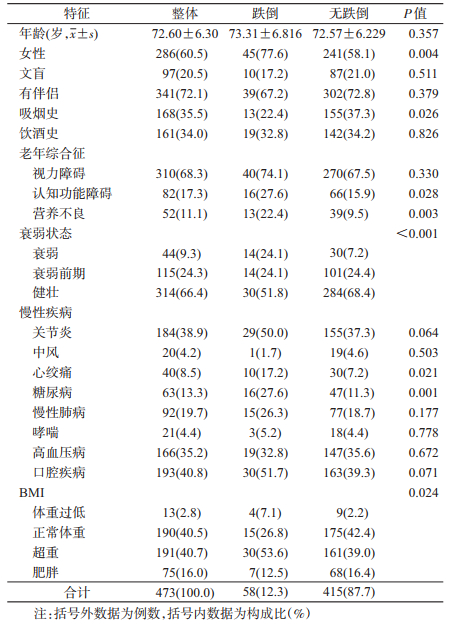
结果1.基本信息:本研究最终纳入473例有效样本,年龄65~98岁,女性占60.5%,9.3%有衰弱,24.3%处于衰弱前期,13.3%有糖尿病。跌倒组女性、有吸烟史的人数以及认知功能障碍、营养不良、心绞痛和糖尿病的患病率明显高于无跌倒组。另外,跌倒组和非跌倒组的衰弱状态、BMI概率分布也明显不同(表 1)。
2.糖尿病和非糖尿病人群中不同衰弱状态下跌倒的发生率:3年间共58人(12.3%)发生跌倒。不同基线衰弱状态和不同糖代谢状态下跌倒发生率有明显差异。在糖尿病人群中,衰弱、衰弱前期和健壮组中跌倒的发生率,差异有统计学意义;在非糖尿病人群中,不同衰弱状态组的跌倒发生率也明显不同(表 2)。

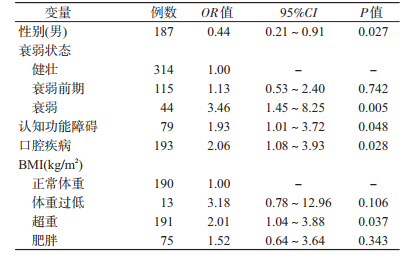
3.跌倒危险因素的多因素logistic回归分析:女性、衰弱、认知功能障碍、口腔疾病和超重是跌倒的独立危险因素(表 3)。
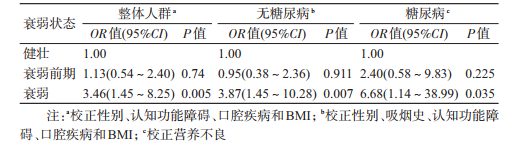
4.不同糖代谢状态下衰弱状态与跌倒的关系:在整体人群中,衰弱组跌倒发生风险是健壮组的3.46倍(95%CI:1.45~8.25)。在非糖尿病人群中,衰弱组跌倒发生风险是健壮组的3.87倍(95%CI:1.45~10.28)。在糖尿病人群中,衰弱组跌倒发生风险是健壮组的6.68倍(95%CI:1.14~38.99)。在3种人群中,衰弱前期都与跌倒发生风险无关(表 4)。
本研究显示都江堰市平义社区老年人3年内跌倒发生率为12.3%,低于北京市农村社区老年人过去1年内跌倒发生率(14.5%)[19]。目前调查糖尿病人群在不同衰弱状态下跌倒发生率的研究很少。本研究发现,无论在糖尿病还是非糖尿病人群中,随着衰弱水平的增加,跌倒发生率都呈上升趋势,且该趋势在糖尿病老年人中更加明显,与一项覆盖10个国家的观察性研究结果类似[20]。
文献报道过的跌倒相关危险因素有100多种。本研究发现的女性、衰弱、口腔疾病、认知功能障碍和超重都是跌倒的独立危险因素,这与许多研究结果基本一致,此外跌倒史、平衡功能受损、步速减慢和下肢疼痛等也可能是跌倒的独立危险因素[6, 21]。BMI与跌倒的关系尚存在争议,可能因为校正的混杂因素、BMI分组标准、样本量和研究对象等不同导致研究结果不一致。本研究显示超重是跌倒的危险因素,而低体重和肥胖与跌倒风险不相关,而Sheehan等[22]研究发现BMI越高未来跌倒发生概率越低(P=0.03)。Himes和Reynolds[23]的研究结果恰好相反,即肥胖程度越高,跌倒风险越高。另一项多中心队列研究则发现,低体重、超重和肥胖都与未来5年跌倒发生风险不相关[24]。
老年糖尿病患者发生跌倒和反复跌倒的风险更高,因此发生骨折和死亡的风险也明显增高[1, 4-5]。本研究发现糖尿病患者未来3年内跌倒发生率明显增加(25.4% vs. 10.2%,P<0.001),研究发现2型糖尿病患者未来1年跌倒风险是非糖尿病老年人的2.25倍(95%CI:1.21~4.15)[5]。英国一项包括1 145名社区老年人(≥65岁)的前瞻性研究发现,糖尿病患者在未来6个月内跌倒(≥2次)的风险明显高于非糖尿病患者(HR=1.63,95%CI:1.06~2.52)[1]。目前,糖尿病患者跌倒风险增加的具体机制尚不明确,但大多数学者认为,糖尿病相关并发症可能是主要原因[4]。例如,周围神经病变会引起平衡功能障碍和步态模式改变,如步速降低、步长缩短和脚踝运动减少,最终导致跌倒风险增加[6]。另外,共病、多药、低血糖等也可能是导致跌倒发生的关键因素。
衰弱与跌倒关系的既往研究结果并不一致。本研究显示,在三组人群中,衰弱都与未来3年内跌倒风险增加显著相关,且衰弱对糖尿病人群发生跌倒的预测能力更强。但过往研究发现,衰弱显著增加未来1年内跌倒风险[25-26],但与未来2年跌倒发生风险的关系无统计学意义[22, 27]。根据FRAIL定义,衰弱的主要特点是疲乏、抗阻力下降、移动能力下降、多共病和体重减轻,这些表型都与跌倒风险存在内在联系[2]。另外,肌少症(年龄相关的肌肉质量和功能下降)作为衰弱的肌肉表现,可能是糖尿病与跌倒之间的关键病理生理联系[28]。而胰岛素抵抗、慢性炎症和线粒体功能障碍又为糖尿病与肌少症之间建立了直接联系[29]。衰弱前期与未来跌倒风险关系的既往研究结果也不一致。本研究显示,在三组人群中,衰弱前期都与未来3年跌倒发生风险不相关,与Kiely等[30]结果一致。Ensrud等[31]关于老年女性的研究也有类似发现,但Ensrud等[32]关于老年男性的研究发现较高的跌倒风险与衰弱前期相关,且相关程度低于其与衰弱的关系,与Samper-Ternent等[33]和Tom等[20]发现类似。结果不一致的原因可能是随访时间、跌倒和衰弱的定义以及性别不同等。
本研究存在局限性。首先,跌倒相关信息通过自我报告获得,可能存在回忆偏倚,造成一些受试者分组错误。其次,只考虑了基线衰弱状态,忽略了衰弱状态随时间的变化。然而,在自然状态下,从衰弱过度到健壮是非常少见的事例,因此不太可能影响本研究的结果。此外,因受访者拒绝访问、死亡、外出,以及人口流动性较大等问题造成失访率较高,使得样本量较小,限制了分层分析的能力。将随访样本和总样本间基线变量进行比较后,发现差异无统计学意义,故较高的失访率并未对样本代表性造成影响。
综上所述,本研究证实衰弱是社区老年人发生跌倒的预测因子,尤其对糖尿病老年人的预测能力更强;而衰弱前期既不是糖尿病也不是非糖尿病老年人发生跌倒的危险因素。由此可推测,衰弱可能是干预糖尿病相关跌倒的一个重要靶点。鉴于跌倒可能给老年人带来灾难性后果,因此,早期识别糖尿病患者合并衰弱综合征是非常必要的。
利益冲突: 无
| [1] | Pijpers E, Ferreira I, De Jongh RT, et al. Older individuals with diabetes have an increased risk of recurrent falls:analysis of potential mediating factors:the Longitudinal Ageing Study Amsterdam[J]. Age Ageing, 2012, 41(3): 358–365. DOI:10.1093/ageing/afr145 |
| [2] | Kojima G, Kendrick D, Skelton DA, et al. Frailty predicts short-term incidence of future falls among British community-dwelling older people:a prospective cohort study nested within a randomised controlled trial[J]. BMC Geriatr, 2015, 15: 155. DOI:10.1186/s12877-015-0152-7 |
| [3] | Xu Y, Wang LM, He J, et al. Prevalence and control of diabetes in Chinese adults[J]. JAMA, 2013, 310(9): 948–959. DOI:10.1001/jama.2013.168118 |
| [4] | Berlie HD, Garwood CL. Diabetes medications related to an increased risk of falls and fall-related morbidity in the elderly[J]. Ann Pharmacother, 2010, 44(4): 712–717. DOI:10.1345/aph.1M551 |
| [5] | Roman De Mettelinge T, Cambier D, Calders P, et al. Understanding the relationship between type 2 diabetes mellitus and falls in older adults:a prospective cohort study[J]. PLoS One, 2013, 8(6): e67055. DOI:10.1371/journal.pone.0067055 |
| [6] | Gravesande J, Richardson J. Identifying non-pharmacological risk factors for falling in older adults with type 2 diabetes mellitus:a systematic review[J]. Disabil Rehabil, 2017, 39(15): 1459–1465. DOI:10.1080/09638288.2016.1199741 |
| [7] | Kojima G. Frailty as a predictor of future falls among community-dwelling older people:a systematic review and meta-analysis[J]. J Am Med Dir Assoc, 2015, 16(12): 1027–1033. DOI:10.1016/j.jamda.2015.06.018 |
| [8] | Umegaki H. Sarcopenia and frailty in older patients with diabetes mellitus[J]. Geriatr Gerontol Int, 2016, 16(3): 293–299. DOI:10.1111/ggi.12688 |
| [9] | Castro-Rodríguez M, Carnicero JA, Garcia-Garcia FJ, et al. Frailty as a major factor in the increased risk of death and disability in older people with diabetes[J]. J Am Med Dir Assoc, 2016, 17(10): 949–955. DOI:10.1016/j.jamda.2016.07.013 |
| [10] | van Kan GA, Rolland Y, Bergman H, et al. The I.A.N.A. task force on frailty assessment of older people in clinical practice[J]. J Nutr Health Aging, 2008, 12(1): 29–37. DOI:10.1007/BF02982161 |
| [11] | Dong LJ, Qiao XX, Tian XY, et al. Cross-cultural adaptation and validation of the FRAIL scale in Chinese community-dwelling older adults[J]. J Am Med Dir Assoc, 2018, 19(1): 12–17. DOI:10.1016/j.jamda.2017.06.011 |
| [12] | Malmstrom TK, Miller DK, Morley JE. A comparison of four frailty models[J]. J Am Geriatr Soc, 2014, 62(4): 721–726. DOI:10.1111/jgs.12735 |
| [13] | Ravindrarajah R, Lee DM, Pye SR, et al. The ability of three different models of frailty to predict all-cause mortality:results from the European Male Aging Study (EMAS)[J]. Arch Gerontol Geriatr, 2013, 57(3): 360–368. DOI:10.1016/j.archger.2013.06.010 |
| [14] | Woo J, Leung J, Morley JE. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation[J]. J Am Geriatr Soc, 2012, 60(8): 1478–1486. DOI:10.1111/j.1532-5415.2012.04074.x |
| [15] | Woo J, Yu RY, Wong M, et al. Frailty screening in the community using the FRAIL scale[J]. J Am Med Dir Assoc, 2015, 16(5): 412–419. DOI:10.1016/j.jamda.2015.01.087 |
| [16] |
陈春明, 国际生命科学学会中国办事处中国肥胖问题工作组联合数据汇总分析协作组. 中国成人体质指数分类的推荐意见简介[J]. 中华预防医学杂志, 2001, 35(5): 349–350.
Chen CM, International Life Sciences Institute China Office China Obesity Task Force Joint Data Analysis Collaborative Team. An introduction to the recommendations of China's adult body mass index classification[J]. Chin J Prev Med, 2001, 35(5): 349–350. DOI:10.3760/j:issn:0253-9624.2001.05.019 |
| [17] | Katzman R, Zhang MY, Ouang-Ya-Qu, et al. A Chinese version of the mini-mental state examination; Impact of illiteracy in a Shanghai dementia survey[J]. J Clin Epidemiol, 1988, 41(10): 971–978. DOI:10.1016/0895-4356(88)90034-0 |
| [18] |
何扬利, 蹇在金. 简易营养评价法及简易营养评价精法对老年人营养不良的评价[J]. 中华老年医学杂志, 2005, 24(4): 278–281.
He YL, Jian ZJ. The application and evaluation of the elderly malnutrition assessment methods[J]. Chin J Geriatr, 2005, 24(4): 278–281. DOI:10.3760/j:issn:0254-9026.2005.04.017 |
| [19] |
张迪, 何耀, 刘淼, 等. 北京市农村社区老年人跌倒情况调查及影响因素研究[J]. 中华流行病学杂志, 2016, 37(5): 624–628.
Zhang D, He Y, Liu M, et al. Study on incidence and risk factors of fall in the elderly in a rural community in Beijing[J]. Chin J Epidemiol, 2016, 37(5): 624–628. DOI:10.3760/cma.j.issn.0254-6450.2016.05.007 |
| [20] | Tom SE, Adachi JD, Anderson FA, et al. Frailty and fracture, disability, and falls:a multiple country study from the global longitudinal study of osteoporosis in women[J]. J Am Geriatr Soc, 2013, 61(3): 327–334. DOI:10.1111/jgs.12146 |
| [21] | Chiba Y, Kimbara Y, Kodera R, et al. Risk factors associated with falls in elderly patients with type 2 diabetes[J]. J Diabetes Complications, 2015, 29(7): 898–902. DOI:10.1016/j.jdiacomp.2015.05.016 |
| [22] | Sheehan KJ, O'Connell MDL, Cunningham C, et al. The relationship between increased body mass index and frailty on falls in community dwelling older adults[J]. BMC Geriatr, 2013, 13: 132. DOI:10.1186/1471-2318-13-132 |
| [23] | Himes CL, Reynolds SL. Effect of obesity on falls, injury, and disability[J]. J Am Geriatr Soc, 2012, 60(1): 124–129. DOI:10.1111/j.1532-5415.2011.03767.x |
| [24] | Boutin E, Natella PA, Schott AM, et al. Interrelations between body mass index, frailty, and clinical adverse events in older community-dwelling women: the EPIDOS cohort study[J]. Clin Nutr, 2017. in Press. DOI: 10.1016/j.clnu.2017.07.023. http://europepmc.org/abstract/MED/28844302 |
| [25] | Wu TY, Chie WC, Yang RS, et al. Risk factors for single and recurrent falls:a prospective study of falls in community dwelling seniors without cognitive impairment[J]. Prev Med, 2013, 57(5): 511–517. DOI:10.1016/j.ypmed.2013.07.012 |
| [26] | de Vries OJ, Peeters GMEE, Lips P, et al. Does frailty predict increased risk of falls and fractures? A prospective population-based study[J]. Osteoporos Int, 2013, 24(9): 2397–2403. DOI:10.1007/s00198-013-2303-z |
| [27] | Forti P, Rietti E, Pisacane N, et al. A comparison of frailty indexes for prediction of adverse health outcomes in an elderly cohort[J]. Arch Gerontol Geriatr, 2012, 54(1): 16–20. DOI:10.1016/j.archger.2011.01.007 |
| [28] | Liccini AP, Malmstrom TK. Frailty and sarcopenia as predictors of adverse health outcomes in persons with diabetes mellitus[J]. J Am Med Dir Assoc, 2016, 17(9): 846–851. DOI:10.1016/j.jamda.2016.07.007 |
| [29] | Cobo A, Vázquez LA, Reviriego J, et al. Impact of frailty in older patients with diabetes mellitus:an overview[J]. Endocrinol Nutr, 2016, 63(6): 291–303. DOI:10.1016/j.endonu.2016.01.004 |
| [30] | Kiely DK, Cupples LA, Lipsitz LA. Validation and comparison of two frailty indexes:the MOBILIZE Boston study[J]. J Am Geriatr Soc, 2009, 57(9): 1532–1539. DOI:10.1111/j.1532-5415.2009.02394.x |
| [31] | Ensrud KE, Ewing SK, Taylor BC, et al. Frailty and risk of falls, fracture, and mortality in older women:the study of osteoporotic fractures[J]. J Gerontol A Biol Sci Med Sci, 2007, 62(7): 744–751. DOI:10.1093/gerona/62.7.744 |
| [32] | Ensrud KE, Ewing SK, Cawthon PM, et al. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men[J]. J Am Geriatr Soc, 2009, 57(3): 492–498. DOI:10.1111/j.1532-5415.2009.02137.x |
| [33] | Samper-Ternent R, Karmarkar A, Graham J, et al. Frailty as a predictor of falls in older Mexican Americans[J]. J Aging Health, 2012, 24(4): 641–653. DOI:10.1177/0898264311428490 |