 2018, Vol. 39
2018, Vol. 39文章信息
- 陈志华, 张梅, 李镒冲, 赵振平, 张笑, 黄正京, 李纯, 王丽敏.
- Chen Zhihua, Zhang Mei, Li Yichong, Zhao Zhenping, Zhang Xiao, Huang Zhengjing, Li Chun, Wang Limin.
- 我国成年人血压水平与心脑血管疾病行为危险因素及其聚集关系分析
- Study on relationship between prevalence or co-prevalence of risk factors for cardiovascular disease and blood pressure level in adults in China
- 中华流行病学杂志, 2018, 39(5): 640-645
- Chinese Journal of Epidemiology, 2018, 39(5): 640-645
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.05.019
-
文章历史
收稿日期: 2017-09-14




2. 100191 北京大学临床研究所数据管理部
2. Peking University Clinical Research Institute, Beijing 100191, China
高血压是我国最常见的慢性病,也是心脑血管疾病重要的危险因素之一。Rapsomaniki等[1]随访研究125万人的队列发现,与理想血压者相比,随着血压水平升高心脑血管疾病发病和死亡风险也增加。现有研究已发现血压水平与吸烟、过量饮酒、蔬菜水果摄入不足、身体活动不足、超重/肥胖、食盐摄入过多行为危险因素相关[2-3],但目前还没有全国代表性的数据对我国≥18岁成年人全人群的血压水平与上述行为危险因素及其聚集的关系进行研究,为此本研究利用“2013年中国慢性病及其危险因素监测”数据探讨我国成年人血压水平与心脑血管疾病行为危险因素及其聚集的关系。
对象与方法1.研究对象:来自2013年中国慢性病及其危险因素监测人群。该监测系统覆盖298个监测区(县),采用多阶段分层整群随机方法抽取181 200名≥18岁常住居民。其总体设计、研究对象的选取方法和定义见文献[4]。
2.研究方法:采用面对面询问调查方式,利用问卷收集基本人口学信息、吸烟、饮酒、蔬菜水果摄入量、身体活动及高血压相关信息;按常规方法测量血压,统一使用欧姆龙HBP-1300电子血压计,测量3次(各间隔1 min),取后2次测量均值作为个体血压值(精确到1 mmHg,1 mmHg=0.133 kPa);统一使用量程为2.0 m、精确度为0.1 cm的身高计和量程为150 kg、最小刻度为0.1 kg的电子体重秤测量身高体重。
3.分析指标及标准:按照欧洲高血压协会和欧洲心脏病学会定义[5],将血压划分为6个水平:理想血压(SBP<120 mmHg且DBP<80 mmHg)、正常血压(SBP<130 mmHg或DBP<85 mmHg)、正常高值(SBP 130~139 mmHg或DBP 85~89 mmHg)及高血压Ⅰ期(SBP 140~159 mmHg或DBP 90~99 mmHg)、Ⅱ期(SBP 160~179 mmHg或DBP 100~109 mmHg)、Ⅲ期(SBP≥180 mmHg或DBP>110 mmHg)。行为危险因素判断:①现在吸烟率为被调查时吸烟者在总人群中所占的比例;②过量饮酒率为男性日均酒精摄入量≥41 g的饮酒行为者或女性日均酒精摄入量≥21 g的饮酒行为者占饮酒者的比例[6];③蔬菜水果摄入不足比例为日均蔬菜水果摄入<400 g者在总人群中所占的比例[7];④身体活动不足率为每周中等强度身体活动<150 min者在总人群中所占的比例[7];⑤超重/肥胖率则按照《中国成人超重和肥胖症预防控制指南》标准[8],即BMI≥24 kg/m2者在总人群中所占的比例;⑥食盐摄入过多比例是根据《中国膳食指南(2007)》的建议,每人食盐摄入量>6 g/d者在总人群中所占的比例[9]。本文将具备上述6种危险因素的数量判为危险因素聚集,共分4个等级(0、1、2、≥3个)。
4.统计学分析:采用SAS 9.4软件进行数据分析,由于样本来自复杂抽样设计,所有统计分析均经过复杂加权。首先描述样本人群不同人口学特征构成(性别、年龄、民族、城乡等)及血压水平分布,并用方差分析(或t检验)比较不同人群血压均值的差异;其次按性别、血压水平分层估计研究对象(剔除服用控制血压药物者)现在吸烟率、过量饮酒率、蔬菜水果摄入不足比例、身体活动不足率和超重/肥胖率,并分析血压水平随危险因素的变化趋势(采用χ2趋势检验);再采用Goodman-Kruskal Gamma方法(Gamma)按性别、“是否服用降压药(即氨氯地平、缬沙坦等)”分层分析血压水平与心血管危险因素聚集的关联性;最后采用累积比数logistic回归分析影响血压水平的因素。检验水准α=0.05。
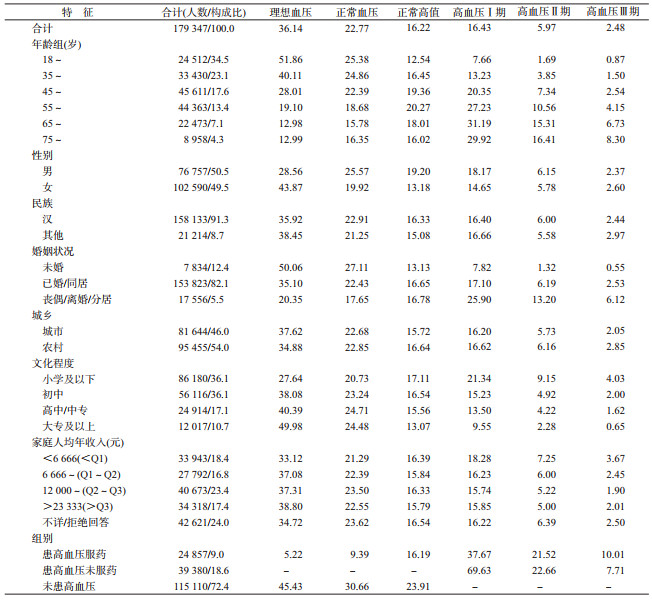
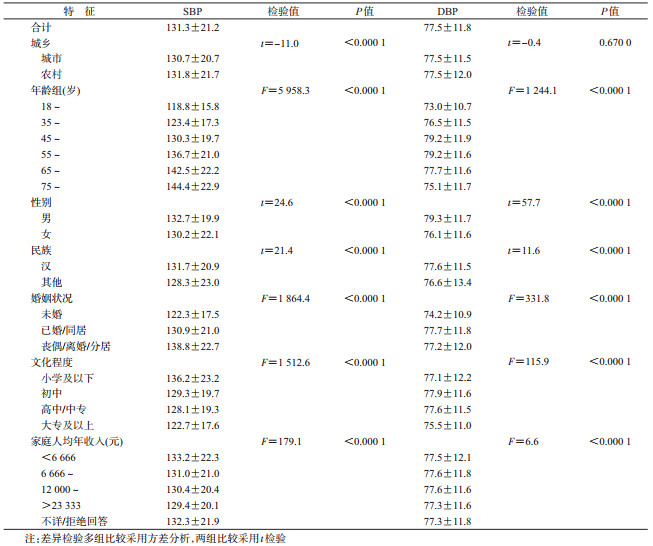
结果1.样本概况及血压水平:本研究纳入有效样本179 347人。年龄45~54岁(M),49.5%为女性,汉族占91.3%,初中及以下文化程度占72.2%,已婚或同居者占82.1%,城市户籍占46.0%,家庭人均年收入12 000~23 333元(M);理想血压者6.48万人(36.14%),正常血压者4.08万人(22.77%),正常高值者2.91万人(16.22%)及高血压Ⅰ、Ⅱ、Ⅲ期分别为2.95万人(16.43%)、1.07万人(5.97%)、0.44万人(2.48%);SBP和DBP平均水平分别为131.3 mmHg和77.5 mmHg;农村户籍人群SBP均值(131.8 mmHg)略高于城市(130.7 mmHg)(P<0.000 1),而城乡人群DBP均值的差异无统计学意义(P=0.67);男性、汉族、有伴侣(已婚/同居、丧偶/离婚/分居)、年龄越大、经济收入越低、文化程度越低者SBP和DBP均值更高,亚组间的差异均有统计学意义(P<0.05)。见表 1、2。
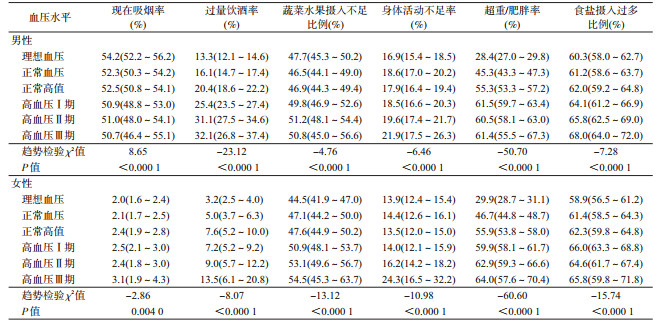
2.未服控制血压药物者血压水平与各危险因素的关系:未服控制血压药物者中,无论性别,血压水平均随着过量饮酒率、蔬菜水果摄入不足比例、身体活动不足率、超重/肥胖率和食盐摄入过多比例的增加而升高。女性血压水平随着现在吸烟率增加而升高(χ2=-2.86,P<0.000 1),而男性血压水平随着现在吸烟率增加而降低(χ2=8.65,P<0.000 1)。见表 3。
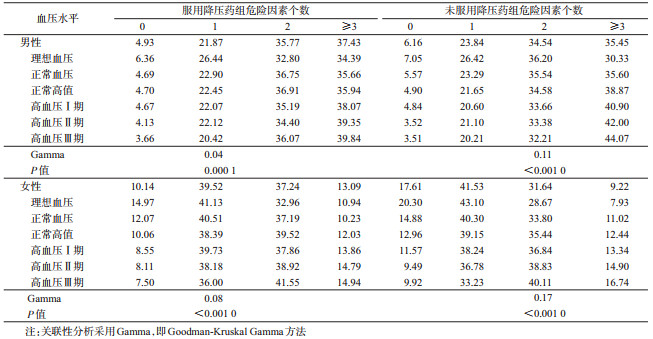
3.我国成年人不同血压水平的危险因素聚集数量分布:按“是否服用降压药”分层发现,无论是否服用降压药,我国成年男女性血压水平均随着危险因素聚集数量增加而升高(P<0.05);未服降压药组关联系数(男女性分别为0.11和0.17)高于服用降压药组(男女性分别为0.04和0.08),说明未服药组血压水平受危险因素数量聚集影响更大(表 4)。
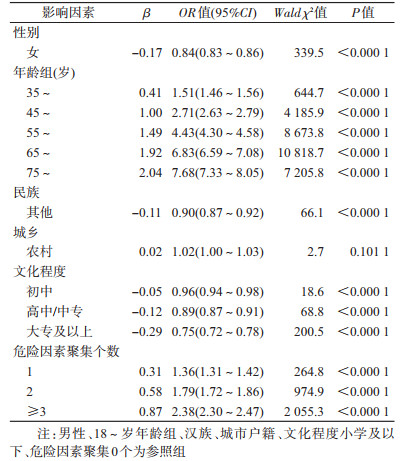
4.影响血压水平的多因素分析:采用多因素logistic分析方法,调整性别、年龄、文化程度、家庭人均年收入等人口学因素影响后,具有危险因素1、2、≥3个组分别是不具有危险因素组的1.36、1.79、2.38倍(表 5)。
本研究发现,我国成年人血压水平控制不佳,普遍存在不健康行为生活方式,尤其是血压水平高者具有更多的行为危险因素。以往调查显示,我国成年人群高血压患病率为27.8%,仅9.7%的高血压患者血压得到控制[10]。本文结果表明我国约1/4成年人血压未达到理想控制水平。究其原因,这可能与我国高血压知晓率较低,管理和治疗效果不佳有关。2010年中国成年人慢性病危险因素监测数据显示,我国仅54.1%的高血压病例知晓自己患有高血压[11];≥35岁的高血压人群管理率为43.99%,而纳入社区高血压管理的病例中规范管理率仅35.30%[12]。此外,我国成年人群中普遍存在高血压相关行为危险因素。本研究结果显示,男性吸烟率与血压水平呈负相关,而女性吸烟率与血压水平呈正相关,关联强度均较弱;无论性别,过量饮酒、蔬菜水果摄入不足、超重/肥胖、食盐摄入过多均与血压水平呈正相关。因此,戒烟限酒、控制体重、减少食盐摄入、增加蔬菜水果摄入,能够有效控制血压水平。
本研究采用多因素分析控制混杂因素后,发现危险因素聚集数量越多血压水平越高,行为危险因素个数呈算术级数增长时,血压水平升高的OR值并未呈几何级数增长。因此危险因素在个体聚集时产生的血压水平升高作用不是简单的单个因素作用叠加,而是存在一种正向的交互和协同作用,导致高血压患病风险成倍增加。本文结果与国内外大型队列研究结果类似[13-14]。目前,对于多项行为危险因素聚集导致血压水平升高的病理生理机制,以及相互之间的量效关系尚不清楚[15-16]。但Elmer等[17]对高血压前期和高血压Ⅰ期的研究对象分组(仅有健康教育组作为对照)进行行为干预,发现多重行为干预组(包括降低BMI、增加身体活动及减少食盐、酒精摄入)、多重行为干预+DASH(dietary approaches to stop hypertension)饮食干预(包括增加蔬菜水果、减少饱和脂肪酸及总脂肪摄入)组高血压患病风险是仅有健康教育组的0.83和0.77倍。
综上所述,本研究利用大样本人群验证了我国成年人群血压水平与吸烟、过量饮酒、蔬菜水果摄入不足、食盐摄入过多、身体活动不足、超重/肥胖等行为危险因素相关,且随个人危险因素聚集数量的增加而升高。
志谢: 感谢31个省(自治区、直辖市)和新疆生产建设兵团各级卫生行政部门的大力支持,以及302个监测点现场工作人员的积极参与和相关专家的悉心指导利益冲突: 无
| [1] | Rapsomaniki E, Timmis A, George J, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1. 25 million people[J]. Lancet, 2014, 383(9932): 1899–1911. DOI:10.1016/S0140-6736(14)60685-1 |
| [2] | Forman JP, Stampfer MJ, Curhan GC. Diet and lifestyle risk factors associated with incident hypertension in women[J]. JAMA, 2009, 302(4): 401–411. DOI:10.1001/jama.2009.1060 |
| [3] | Masala G, Bendinelli B, Versari D, et al. Anthropometric and dietary determinants of blood pressure in over 7000 Mediterranean women:the European Prospective Investigation into Cancer and Nutrition-Florence cohort[J]. J Hypertens, 2008, 26(11): 2112–2120. DOI:10.1097/HJH.0b013e32830ef75c |
| [4] |
王丽敏, 张梅, 李镒冲, 等. 2013年中国慢性病及其危险因素监测总体方案[J]. 中华预防医学杂志, 2018, 52(2): 191–194.
Wang LM, Zhang M, Li YC, et al. Scheme of the Chinese chronic non-communicable disease and risk factor surveillance[J]. Chin J Prev Med, 2018, 52(2): 191–194. DOI:10.3760/cma.j.issn.0253-9624.2018.02.015 |
| [5] | Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension:the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)[J]. Blood Press, 2013, 22(4): 193–278. DOI:10.3109/08037051.2013.812549 |
| [6] | Desapriya EBR, Stockwell T, Doll SR, et al. International guide for monitoring alcohol consumption and related harm[R]. WHO/MSD/MSB/00. 4. Geneva: World Health Organization, 2000. DOI: 10.13140/RG.2.2.29007.48808. |
| [7] | WHO. Draft action plan for the prevention and control of noncommunicable diseases 2013-2020[R]. Geneva: World Health Organization, 2013. |
| [8] |
陈春明, 孔灵芝. 中国成人超重和肥胖症预防控制指南[M]. 北京: 人民卫生出版社, 2006.
Chen CM, Kong LZ.The guidelines for prevention and control of overweight and obesity in Chinese adults[M]. Beijing: People's Medical Publishing House, 2006. |
| [9] |
中国营养学会. 中国居民膳食指南2016[M]. 北京: 人民卫生出版社, 2016.
Chinese Nutrition Society.Dietary guidelines for Chinese residents (2016)[M]. Beijing: People's Medical Publishing House, 2016. |
| [10] |
中国疾病预防控制中心. 中国慢性病及其危险因素监测报告2013[M]. 北京: 军事医学科学出版社, 2016.
Chinese Center for Disease Control and Prevention.Report on chronic disease risk factor surveillance in China[M]. Beijing: Military Medical Science Press, 2016. |
| [11] | Pan Y, Zhao X, Yong J, et al. Prevalence, awareness and control of hypertension in patients with transient ischemic attacks in China[J]. Neuroepidemiology, 2016, 46(2): 84–87. DOI:10.1159/000442419 |
| [12] |
曾新颖, 王丽敏, 王临虹, 等. 中国35岁以上高血压患者社区管理的现状研究[J]. 中华预防医学杂志, 2013, 47(11): 1014–1019.
Zeng XY, Wang LM, Wang LH, et al. The study of management of hypertensive people aged 35 and over in communities in China[J]. Chin J Prev Med, 2013, 47(11): 1014–1019. DOI:10.3760/cma.j.issn.0253-9624.2013.11.010 |
| [13] |
吴兆苏, 姚崇华, 赵冬, 等. 11省市队列人群心血管病发病前瞻性研究Ⅱ.个体危险因素聚集与心血管病发病的关系[J]. 中华心血管病杂志, 2001, 29(4): 246–250.
Wu ZS, Yao CH, Zhao D, et al. A prospective cohort study on cardiovascular disease incidence in 11 provinces in China Ⅱ. Associations between individual risk factor aggregation and cardiovascular disease incidence[J]. Chin J Cardiol, 2001, 29(4): 246–250. DOI:10.3760/j:issn:0253-3758.2001.04.016 |
| [14] | Levy RI. The Framingham Study:the epidemiology of atherosclerotic disease[J]. JAMA, 1981, 245(5): 512. DOI:10.1001/jama.1981.03310300064027 |
| [15] | Yu DH, Huang JF, Hu DS, et al. Association between prehypertension and clustering of cardiovascular disease risk factors among Chinese adults[J]. J Cardiovasc Pharmacol, 2009, 53(5): 388–400. DOI:10.1097/FJC.0b013e3181a02238 |
| [16] | Li YC, Feng XQ, Zhang M, et al. Clustering of cardiovascular behavioral risk factors and blood pressure among people diagnosed with hypertension:a nationally representative survey in China[J]. Sci Rep, 2016, 6: 27627. DOI:10.1038/srep27627 |
| [17] | Elmer PJ, Obarzanek E, Vollmer WM, et al. Effects of comprehensive lifestyle modification on diet, weight, physical fitness, and blood pressure control:18-month results of a randomized trial[J]. Ann Intern Med, 2006, 144(7): 485–495. DOI:10.7326/0003-4819-144-7-200604040-00007 |