 2018, Vol. 39
2018, Vol. 39文章信息
- 任艳婷, 贾清珍, 张向东, 郭百锁, 张峰峰, 程晓天, 王永平.
- Ren Yanting, Jia Qingzhen, Zhang Xiangdong, Guo Baisuo, Zhang Fengfeng, Cheng Xiaotian, Wang Yongping.
- 山西省不同水碘地区孕妇和哺乳期妇女甲状腺功能调查
- Prevalence of thyroid function in pregnant and lactating women in areas with different iodine levels of Shanxi province
- 中华流行病学杂志, 2018, 39(5): 609-613
- Chinese Journal of Epidemiology, 2018, 39(5): 609-613
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.05.013
-
文章历史
收稿日期: 2017-09-18




碘是机体合成甲状腺激素的重要原料,研究资料显示,过量碘摄入可导致甲状腺肿、甲状腺功能异常及甲状腺相关疾病的发生[1-3]。山西省水源性高碘地区分布在10个县(市、区)的29个乡镇,这些地区的孕妇和哺乳期妇女存在碘摄入过量的潜在风险,且孕妇和哺乳期妇女处于特殊生理时期,甲状腺功能会发生较大变化,更易发生甲状腺相关疾病。本研究通过对高碘和适碘地区的孕妇和哺乳期妇女进行流行病学调查,探讨高碘对妊娠、哺乳期妇女甲状腺功能的影响。
对象与方法1.调查对象:在2013年山西省外环境水碘含量调查结果基础上,将汾阳、平遥2县作为调查地区(两县相距39 km),选择水碘含量>300 μg/L的地区(汾阳冀村镇4村、平遥宁固镇8村)作为高碘地区,并选择与其地理位置毗邻,水碘含量在50~100 μg/L之间,生活水平、饮食习惯、环境状况等相近的地区(汾阳阳城乡2村、汾阳贾家庄镇1村)作为适碘地区。采用分层随机抽样方法,在高碘和适碘地区共抽取19~40岁孕妇130(高碘64、适碘66)名、哺乳期妇女220(高碘124、适碘96)名作为调查对象。全部调查对象身体健康、在当地持续居住2年以上。本研究通过山西省地方病防治研究所伦理委员会审查,调查时均获得知情同意。
2.调查方法:调查前按统一方法培训现场调查和实验室人员。所有实验室检测项目从采样到结果报告均进行严格的质量控制,每一种指标均由同一名专业人员负责测定,保证实验室各项检测结果的准确性。
(1)水碘:在被调查村按东、西、南、北、中5个方位各采集2户居民饮用水水样,利用经无碘处理的采样瓶共采集水样(≥50 ml)150份。采样瓶用预采水样涮洗2次后再行采样,4 ℃冰箱冷藏,并尽快送实验室检测。采用砷铈催化分光光度法检测水碘含量。
(2)盐碘:在被调查村各采集盐样15份,根据《制盐工业通用试验方法碘离子的测定》(GB/T 13025.7-2012)检测盐碘含量。
(3)尿碘:采集调查对象1次随机尿样(≥5 ml),置于经无碘处理的聚乙烯塑料管或玻璃试管中,密封并置于4 ℃冰箱冷藏,尽快送实验室检测。根据《尿中碘的砷铈催化分光光度法》(WS/T 107-2006)检测尿碘含量。尿碘标准物由国家碘缺乏病参照实验室提供。
(4)血甲状腺功能:采集调查对象空腹静脉血5 ml,室温放置20~30 min后,离心半径8 cm,3 500 r/min离心10 min,而后取血清分装,冷冻待检。采用电化学发光免疫分析法检测血清促甲状腺素(TSH),试剂盒由罗氏诊断产品(上海)有限公司提供;采用化学发光免疫分析法检测血清游离甲状腺素(FT4)、抗甲状腺过氧化物酶自身抗体(TPOAb)、抗甲状腺球蛋白抗体(TGAb),试剂盒由德国西门子股份公司提供。
3.判定标准:①正常值参考范围:根据《中国甲状腺疾病诊治指南》和《妊娠和产后甲状腺疾病诊治指南》推荐使用罗氏试剂和西门子试剂的参考值范围[4]。哺乳期妇女为FT4 11.5~22.7 pmol/L、TSH 0.27~4.20 mIU/L;孕早期(T1)妇女为FT4 14.34~20.53 pmol/L、TSH 0.05~5.17 mIU/L;孕中期(T2)妇女为FT4 12.63~18.83 pmol/L、TSH 0.39~5.22 mIU/L;孕晚期(T3)妇女为FT4 11.6~17.49 pmol/L、TSH 0.60~6.84 mIU/L。自身抗体阳性判定标准:TPOAb 0~60 U/ml、TGAb 0~60 U/ml。②甲状腺功能状态实验室判定标准参照《中国甲状腺疾病诊治指南》和《妊娠和产后甲状腺疾病诊治指南》[4]。③甲状腺自身抗体阳性为TPOAb>60 U/ml和/或TGAb>60 U/ml。
4.统计学分析:应用SPSS 19.0软件进行统计学分析。数据经正态性检验,尿碘和甲状腺功能指标均呈偏态分布,以M和P25~P75表示,各指标M的比较采用秩和检验,率的比较采用χ2检验。检验水准α=0.05。
结果1.基本情况及碘营养环境调查:350名妇女年龄范围为19~40岁,适碘地区孕妇、哺乳期妇女和高碘地区孕妇、哺乳期妇女的年龄分别为(24.55±6.28)、(26.02±6.37)、(24.84±6.24)、(25.92±6.79)岁,差异无统计学意义(t=1.094,P>0.05)。共采集水样150份,经实验室复核检测,适碘地区水碘M为57.5 μg/L,高碘地区水碘M为464.8 μg/L(表 1)。适碘地区共采集盐样45份,盐碘M为22.3(1.1~24.7)mg/kg,碘盐覆盖率为97.87%,合格碘盐食用率为95.56%,调查74名8~10岁儿童尿碘M为278.7 μg/L;高碘地区共采集盐样179份,其中无碘盐164份,无碘食盐覆盖率为91.62%,调查196名8~10岁儿童尿碘M为680.4 μg/L。两地区碘营养环境调查情况符合调查点分组要求。
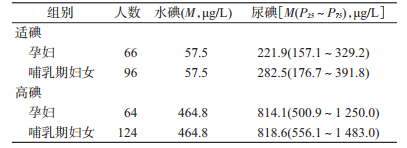
2.尿碘检测:参照文献[5]的标准,350名妇女中,适碘地区孕妇尿碘M为221.9 μg/L,碘营养水平适宜;哺乳期妇女尿碘M为282.5 μg/L,碘营养水平超过适宜量。高碘地区孕妇和哺乳期妇女尿碘M分别为814.1、818.6 μg/L,碘营养水平均过量。高、适碘两组进行组内比较,孕妇和哺乳期妇女之间尿碘水平差异无统计学意义(Z=-1.440、-0.873,均P>0.05);组间比较,高碘组孕妇和哺乳期妇女尿碘水平均高于适碘组孕妇和哺乳期妇女,差异有统计学意义(Z=-9.880、-7.009,均P<0.01)。见表 1。
3.甲状腺激素水平及抗体检测:将低于和/或高于参考值的指标定义为异常值。行组内比较,高、适碘两地区内哺乳期妇女血FT4水平低于孕妇、TSH异常值率高于孕妇,差异有统计学意义(FT4:Z=-6.677、-4.041,均P<0.01;TSH:Z=8.797、8.910,均P<0.01),血TSH水平差异无统计学意义(均P>0.05);高碘地区哺乳期妇女血FT4异常值率高于孕妇,差异有统计学意义(Z=7.338,P=0.007),适碘地区血FT4异常值率组内差异无统计学意义(P>0.05)。行组间比较,高碘地区哺乳期妇女血FT4水平低于适碘地区哺乳期妇女,差异有统计学意义(Z=-4.687,P<0.01),TSH水平差异无统计学意义(P>0.05);孕妇血FT4、TSH水平组间差异无统计学意义(均P>0.05)。4组妇女血甲状腺自身抗体阳性率组内和组间比较差异均无统计学意义(均P>0.05)。见表 2。

将孕妇按不同孕期分组后行组内比较,高碘地区内T1期孕妇血FT4高于T2、T3期孕妇、TSH水平低于T2、T3期孕妇,差异有统计学意义(FT4:Z=-2.174、-2.238,均P<0.05;TSH:Z=-2.985、-1.978,均P<0.05);适碘地区内不同孕期妇女血FT4、TSH水平差异无统计学意义(均P>0.05)。不同孕期妇女血甲状腺自身抗体阳性率差异无统计学意义(均P>0.05)。见表 3。

4.甲状腺功能状态实验室判定情况:350名孕妇和哺乳期妇女中甲状腺功能平均正常率为84.6%。适碘地区孕妇、哺乳期妇女和高碘地区孕妇、哺乳期妇女的甲状腺功能异常例数分别为0例(0.0%)、12例(12.5%)、7例(10.9%)、35例(20.2%),高碘地区孕妇、哺乳期妇女的甲状腺功能异常率均高于适碘地区,差异有统计学意义(χ2=7.630、7.965,均P<0.01)。其中高碘地区孕妇、哺乳期妇女的亚临床甲状腺功能减退症(甲减)率均有升高,差异有统计学意义(χ2=5.363、5.007,均P<0.05)。甲状腺功能亢进症(甲亢)、亚临床甲亢、甲减率在4组间比较差异均无统计学意义(均P>0.05)。见表 4。

既往研究表明[6-7],孕妇、哺乳期妇女的甲状腺激素水平与非妊娠期妇女相差较大,且不同孕期妇女甲状腺激素水平亦不同。本研究结果显示,在适碘和高碘地区哺乳期妇女的FT4水平低于孕妇,高碘地区哺乳期妇女血FT4异常值率高于该地区孕妇;且高碘地区孕早期妇女的FT4水平高于孕中、晚期妇女,分析原因,一是催乳素可以过下丘脑-垂体-甲状腺轴的反馈抑制作用,间接抑制和影响血甲状腺激素的生成和代谢[8-9],哺乳期妇女FT4水平下降及血FT4异常值率增高可能与其催乳素分泌增加有关。二是在孕早期,女性人绒毛膜促性腺激素(hCG)水平6~8周达峰值,此后逐渐下降,hCG具有TSH样作用,可刺激甲状腺合成激素增加,并反馈性抑制垂体分泌TSH;且在孕中、晚期,孕妇雌激素水平不断增高,血中甲状腺素结合球蛋白(TBG)亦随之增加,TBG与FT4结合从而影响其储存和代谢,此外,妊娠后期孕妇体液较正常人明显增多,故孕早期妇女FT4水平相对较高,TSH水平相对较低可能与上述原因有关。
本研究还显示,高碘地区哺乳期妇女血FT4水平低于适碘地区,孕妇、哺乳期妇女的甲状腺功能异常率和亚临床甲减率均高于适碘地区。提示高碘可能增加妇女甲状腺功能异常的发生风险。长期过量碘摄入可能导致甲状腺细胞表面的钠/碘同向转运体表达下降,碘转运障碍,甲状腺细胞内碘浓度下降,甲状腺激素合成减少[10]。史晓光等[11]研究报道,孕期碘超足量和碘过量可以导致母体亚临床甲减患病率和低T4血症的增加,但对甲状腺自身抗体没有影响。本研究与该研究结果一致。亚临床甲减的发生受多种因素的影响,碘生物暴露水平的增加可能导致亚临床甲减患病风险增高[12]。动物实验亦发现,随着碘摄入量的增加,大鼠血清和甲状腺组织中的甲状腺激素水平呈现降低趋势[13]。碘可能作为环境因素促发妇女亚临床甲减及其他甲状腺疾病的发生和发展。
综上所述,高碘可能增加孕妇和哺乳期妇女特殊人群甲状腺功能异常的危险性,并增加妇女甲状腺疾病的患病率及可能影响胎儿的智力发育和生存率[14]。建议关注高碘地区孕妇和哺乳期妇女的亚临床甲减问题,加强对该人群的碘营养及甲状腺功能的监测。本研究存在不足。受调查人群个体差异、调查样本量等因素的影响,结果可能存在一定偏倚,还需进一步探讨。
利益冲突: 无
| [1] |
桑仲娜, 魏薇, 张淑芬, 等. 高碘地区妊娠晚期妇女与育龄妇女甲状腺功能的比较[J]. 中华内分泌代谢杂志, 2011, 27(8): 667–670.
Sang ZN, Wei W, Zhang SF, et al. A comparative study on thyroid function during late pregnancy and of fertile women in iodine excess area[J]. Chin J Endocrinol Metab, 2011, 27(8): 667–670. DOI:10.3760/cma.j.issn.1000-6699.2011.08.014 |
| [2] |
林琳, 高美丽, 申红梅, 等. 不同碘营养水平哺乳期母鼠及其仔鼠甲状腺形态观察[J]. 中华地方病学杂志, 2012, 31(3): 255–258.
Lin L, Gao ML, Shen HM, et al. Different levels of iodine intake and thyroid morphological changes of lactating rats and their newborns[J]. Chin J Endemiol, 2012, 31(3): 255–258. DOI:10.3760/cma.j.issn.1000-4955.2012.03.005 |
| [3] |
任艳婷, 贾清珍, 张向东, 等. 山西省不同碘摄入量地区育龄妇女甲状腺疾病调查[J]. 中华流行病学杂志, 2014, 35(1): 45–48.
Ren YT, Jia QZ, Zhang XD, et al. Epidemiological investigation on thyroid disease among fertile women in different iodine intake areas of Shanxi province[J]. Chin J Epidemiol, 2014, 35(1): 45–48. DOI:10.3760/cma.j.issn.0254-6450.2014.01.011 |
| [4] |
中华医学会内分泌学分会, 中华医学会围产医学分会. 妊娠和产后甲状腺疾病诊治指南[J]. 中华内分泌代谢杂志, 2012, 28(5): 354–371.
Chinese Society of Endocrinology, Chinese Society of Perinatal Medicine. Guidelines for the diagnosis and management of thyroid disease during pregnancy and the postpartum[J]. Chin J Endocrinol Metab, 2012, 28(5): 354–371. DOI:10.3760/cma.j.issn.1000-6699.2012.05.002 |
| [5] | WHO/UNICEF/ICCIDD.Assessment of Iodine deficiency disorders and monitoring their elimination:a guide for programme managers[M]. 3rd ed. Geneva: WHO, 2007: 32–34. |
| [6] |
莫哲, 楼晓明, 王晓峰, 等. 浙江省孕妇以及哺乳期妇女甲状腺激素参考区间的探讨[J]. 中华地方病学杂志, 2017, 36(4): 279–283.
Mo Z, Lou XM, Wang XF, et al. Reference data of thyroid hormones for pregnancy and lactating women in Zhejiang[J]. Chin J Endemiol, 2017, 36(4): 279–283. DOI:10.3760/cma.j.issn.2095-4255.2017.04.010 |
| [7] |
陈伯尼, 陈志辉, 兰莺, 等. 福建省不同孕期孕妇甲状腺功能指标参考值的建立和运用[J]. 中华地方病学杂志, 2017, 36(5): 357–360.
Chen BN, Chen ZH, Lan Y, et al. Establishment and application of women thyroid function indicators reference interval during pregnancy in Fujian Province[J]. Chin J Endemiol, 2017, 36(5): 357–360. DOI:10.3760/cma.j.issn.2095-4255.2017.05.011 |
| [8] | Bonomo IT, Lisboa PC, Passos MC, et al. Prolactin inhibition at the end of lactation programs for a central hypothyroidism in adult rat[J]. J Endocrinol, 2008, 198(2): 331–337. DOI:10.1677/joe-07-0505 |
| [9] | Lisboa PC, Pires L, de Oliveira E, et al. Prolactin inhibition at mid-lactation influences adiposity and thyroid function in adult rats[J]. Horm Metab Res, 2010, 42(8): 562–569. DOI:10.1055/s-0030-1253434 |
| [10] | Eng PHK, Cardona GR, Fang SL, et al. Escape from the acute Wolff-Chaikoff effect is associated with a decrease in thyroid sodium/iodide symporter messenger ribonucleic acid and protein[J]. Endocrinology, 1999, 140(8): 3404–3410. DOI:10.1210/en.140.8.3404 |
| [11] |
史晓光, 滕晓春, 单忠艳, 等. 妊娠早期碘营养状况与甲状腺功能关系的流行病学调查[J]. 中国实用内科杂志, 2009, 29(6): 520–522.
Shi XG, Teng XC, Shan ZY, et al. An epidemiological study of the relationship between iodine intake levels and thyroid function during early pregnancy[J]. Chin J Prac Intern Med, 2009, 29(6): 520–522. |
| [12] |
桑仲娜, 张万起, 董作亮, 等. 不同碘摄入水平与人群甲状腺疾病关系[J]. 中国公共卫生, 2008, 24(8): 952–954.
Sang ZN, Zhang WQ, Dong ZL, et al. Relationship between different iodine intake levels and thyroid disease in medical students[J]. Chin J Public Health, 2008, 24(8): 952–954. DOI:10.11847/zgggws2008-24-08-30 |
| [13] |
叶艳, 王琨, 张璐, 等. 不同碘摄入量对大鼠碘代谢及甲状腺功能影响[J]. 中国公共卫生, 2007, 23(6): 714–716.
Ye Y, Wang K, Zhang L, et al. Effects of different levels of iodine intake on iodine metabolism and thyroid function in rats[J]. Chin J Public Health, 2007, 23(6): 714–716. DOI:10.3321/j.issn:1001-0580.2007.06.044 |
| [14] | Cooper DS. Clinical practice. Subclinical hypothyroidism[J]. N Engl J Med, 2001, 345(4): 260–265. DOI:10.1056/NEJM200107263450406 |