 2018, Vol. 39
2018, Vol. 39文章信息
- 韩迪迪, 韩春霞, 李璐钰, 王明, 杨靖寰, 李曼.
- Han Didi, Han Chunxia, Li Luyu, Wang Ming, Yang Jinghuan, Li Man.
- 中国2013-2017年人感染H7N9禽流感的流行病学特征
- Epidemiology of human infection with avian influenza A(H7N9) virus in China, 2013-2017
- 中华流行病学杂志, 2018, 39(1): 44-46
- Chinese Journal of Epidemiology, 2018, 39(1): 44-46
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2018.01.009
-
文章历史
收稿日期: 2017-06-26




自2013年3月上海市和安徽省公布首批3例人感染H7N9禽流感(即病毒核酸检测阳性的临床患者),之后陆续发现并新增H7N9确诊病例。首个H7N9感染病例出现至今,人感染H7N9禽流感已经有5波周期性流行,分别为2013年3-4月,2013年11月至2014年4月,2014年11月至2015年4月,2015年11月至2016年4月,2016年10月至2017年4月,前4波病例有明显下降趋势[1],然而第5波来势汹汹,2016年12月的发病例数为既往同期病例的2.7~6.1倍[2]。为了解H7N9的疫情现状,以便为该传染病的实时防控提供科学依据,现对人感染H7N9禽流感病例的流行病学分布特征进行描述和分析。
资料与方法1.资料来源:2013年3月至2017年4月WHO及国家卫生和计划生育委员会报告的实验室确诊人感染H7N9禽流感病例的公开数据[3-4]。
2.统计学方法:将所有病例相关资料(年龄、性别、发病时间、地区分布、暴露情况等)录入计算机,采用Excel 2007软件对数据进行统计学分析,绘制线图和直方图等,描述其流行病学特征。
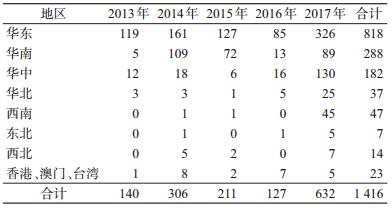
结果1.时间分布:2013年3月,上海市和安徽省首次发现人感染甲型H7N9禽流感病毒病例。截至2017年4月,我国累计出现1 416例人感染H7N9禽流感确诊病例,第1波和第2波报告病例数相近,第3波、第4波报告病例逐年下降。第5波的流行始于2016年10月,早于以往流行期,此后4个月H7N9禽流感病例显著增加,2017年1月发病人数达到292人(图 1)。人感染H7N9禽流感病死率较高,2013年3月至2017年4月,各年度病死率分别为34.3%、44.1%、43.6%、57.5%、33.4%(表 1)。

|
| 图 1 2013-2017年WHO报告我国人感染H7N9病例 |

2.地区分布:1 416例H7N9感染病例广泛分布于全国28个省(自治区、直辖市)。统计数据显示,人感染H7N9禽流感病例与地区分布具有非常密切的联系,地域性明显,病例主要集中在华东、华南和华中地区(表 2)。发病例数排在前三位的省份为浙江(299例)、广东(258例)、江苏(243例),占全国总报告病例数的56.59%。
3.人群分布:
(1) 年龄性别构成:1 416例病例中,男性956例,女性415例,比例约为2.3 : 1,性别不详45例(表 3)。病例年龄M=55岁,提示50~60岁人群为H7N9高发人群。
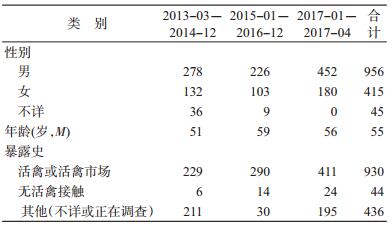
(2) 暴露情况:1 416例病例中,有过活禽和活禽市场接触史的为930例,明确表示无接触史的为44例,而接触史不详或正在调查者为436例,见表 3。
(3) 聚集性病例:是指7 d内在小范围(如1个家庭、1个社区等)发现≥2例,提示可能存在人际传播或因共同暴露而感染的人感染H7N9禽流感确诊病例或疑似病例。截至2017年4月,我国共发生35起家庭聚集性病例(2013年5起[5],2014年9起[5],2015年6起[5],2016年5起,2017年10起),累计72例。在35起家族聚集性病例中,发生在有血缘关系的亲属中的有23起,发生在无血缘关系但有密切接触的有8起。
讨论本研究结果显示,H7N9发病时间集中,发病的高峰均出现在每年11月至次年4月,7-9月是发病的低谷时期,具有冬春季高发的季节性特点。
从地区分布上分析,确诊的H7N9病例主要集中在我国华东、华中和华南,有明显的地区聚集性。这可能与当地居民的活禽养殖、消费和饮食习惯有关。华东、华南地区自然环境和禽类销售链(销售市场80%主要集中在长江流域以南地区)可能是地区聚集性的主要原因之一[6]。华东和华南地区的地理条件相似,都是温暖潮湿,有利于病原体增殖,再加上华东和华南地区经济发达、人口密度大、人流量巨大,极易导致流行病的传播。
从人群分布特点分析,人感染H7N9禽流感确诊的病例中以男性、中老年人居多,这与前期的研究结果一致[7]。男性明显多于女性。这可能与我国男性较女性有较高的慢性呼吸道疾病患病率有关[6]。
从暴露情况来分析,大多数病例在发病前具有相关活禽暴露(暴露于活禽市场或活禽环境)的情况。已有研究表明,暴露在活禽的环境下,与感染H7N9病毒的风险增加有关[8]。而活禽市场的控制措施已确定能够有效控制H7N9禽流感暴发[9]。目前,确诊的人感染H7N9禽流感病例仍以散发状态为主,占总比例的95%。还没有充分的证据可以说明病毒可在人群中持续传播,但家庭聚集性病例的出现提示人传人的可能。
利益冲突: 无
| [1] | Xiang NJ, Li XY, Ren RQ, et al. Assessing change in avian influenza A(H7N9) virus infections during the fourth epidemic-China, September 2015-August 2016[J]. MMWR Morb Mortal Wkly Rep, 2016, 65(49): 1390–1394. DOI:10.15585/mmwr.mm6549a2 |
| [2] | Zhou L, Ren RQ, Yang L, et al. Sudden increase in human infection with avian influenza A(H7N9) virus in China, September-December 2016[J]. Western Pacific Surveill Response J, 2017, 8(1): 6–14. DOI:10.5365/WPSAR.2017.8.1.001 |
| [3] | Huo X, Chen L, Qi X, et.al. Significantly elevated number of human infections with H7N9 virus in Jiangsu in eastern China, October 2016 to January 2017[J]. Euro Surveill, 2017, 22(13): pii=30496. DOI:10.2807/1560-7917.ES.2017.22.13.30496 |
| [4] |
李鹏媛, 徐浩, 顾豪高, 等.
中国大陆H7N9禽流感病毒流行病学特征及血凝素和神经氨酸酶的分子进化[J]. 中山大学学报:医学科学, 2014, 35(6): 933–940.
Li PY, Xu H, Gu HG, et al. Epidemiological characteristics of influenza virus H7N9 and evolutionary analysis of hemagglutinin and neuraminidase genes[J]. J Sun Yat-sen Univ:Med Sci, 2014, 35(6): 933–940. DOI:10.13471/j.cnki.j.sun.yat-sen.univ(med.sci).2014.01.54 |
| [5] |
贾潇岳, 杜沛玲, 徐镇喜, 等.
人禽流感H7N9病例的流行病学特征分析[J]. 汕头大学医学院学报, 2016, 29(4): 229–230.
Jia XY, Du PL, Xu ZX, et al. The charcteristic of human H7N9 cases[J]. J Shantou Univ Med Coll, 2016, 29(4): 229–230. DOI:10.13401/j.cnki.jsumc.2016.04.016 |
| [6] | Li J, Rao YH, Sun QL, et al. Identification of climate factors related to human infection with avian influenza A H7N9 and H5N1 viruses in China[J]. Nat Sci Rep, 2015, 5: 18094. DOI:10.1038/srep18094 |
| [7] | Li Q, Zhou L, Zhou MH, et al. Epidemiology of human infections with avian influenza A(H7N9) virus in China[J]. N Engl J Med, 2014, 370(6): 520–532. DOI:10.1056/NEJMoa1304617 |
| [8] | Zhou L, Ren RQ, Ou JM, et al. Risk factors for influenza A(H7N9) Disease in China, a matched case control study, October 2014 to April 2015[J]. Open Forum Infect Dis, 2016, 3(3): ofw182. DOI:10.1093/ofid/ofw182 |
| [9] | Yu HJ, Wu JT, Cowling BJ, et al. Effect of closure of live poultry markets on poultry-to-person transmission of avian influenza A H7N9 virus:an ecological study[J]. Lancet, 2014, 383(9916): 541–548. DOI:10.1016/S0140-6736(13)61904-2 |