 2017, Vol. 38
2017, Vol. 38文章信息
- 王政和, 徐荣彬, 董彦会, 阳益德, 王烁, 王西婕, 杨招庚, 邹志勇, 马军.
- Wang Zhenghe, Xu Rongbin, Dong Yanhui, Yang Yide, Wang Shuo, Wang Xijie, Yang Zhaogeng, Zou Zhiyong, Ma Jun.
- 剖宫产与6~17岁儿童青少年期肥胖的关联研究
- Association between cesarean birth and the risk of obesity in 6-17 year-olds
- 中华流行病学杂志, 2017, 38(12): 1598-1602
- Chinese journal of Epidemiology, 2017, 38(12): 1598-1602
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2017.12.002
-
文章历史
收稿日期: 2017-04-23




剖宫产是产科处理高危妊娠、解决难产从而降低孕产妇和婴儿死亡率的有效手段[1]。但也有研究表明,剖宫产可能会损害母婴的健康状况,尤其是婴儿[2]。建议人群剖宫产率的适宜水平为10%~15%[3]。随着社会经济的发展、医疗卫生保健网络的完善、手术和麻醉技术的进步与剖宫产术后并发症的降低,越来越多的孕妇选择剖宫产进行分娩[4-5]。为探讨剖宫产与儿童青少年期肥胖风险的关联。本研究基于2012年卫生行业公益性科研专项数据分析剖宫产与6~17岁儿童青少年肥胖风险的关联,为剖宫产的合理使用提供进一步的科学依据。
对象与方法1.研究对象:来自2012年卫生行业公益性科研专项“学生重大疾病防控技术和相关标准研制及应用”中湖南、宁夏、天津、重庆、辽宁、上海和广东7个省份的示范基地,采用分层整群随机抽样方法[6],在7个省份共抽取93所中小学校(各省份分别抽取1个经济水平好和1个经济水平差的城市,从中分别抽取12~16所中小学校),包括小学1~6年级及初一、初二、高一和高二年级学生。根据病史及体格检查资料,排除心、肺、肝、肾等重要脏器患有器质性疾病及身体发育异常或畸形者。选取其母亲分娩方式等资料完整的6~17岁中小学生共42 758人,其中男生21 097人(49.3%),女生21 661人(50.7%)。湖南省4 615人(10.8%),宁夏回族自治区2 239人(5.2%),天津市8 255人(19.3%),重庆市7 190人(16.8%),辽宁省7 050人(16.5%),上海市7 918人(15.4%)和广东省5 491人(12.8%)。本研究通过北京大学医学伦理委员会审批(批号:IRB0000105213034),所有研究对象均签署知情同意书。
2.研究方法:包括体格检查和问卷调查。体格检查(包括身高、体重、腰围和血压等指标)严格按照“2010年中国学生体质与健康调研报告”的操作规范[7]。采用自制问卷收集学生的基本情况、体力活动和饮食等。同时采用自制家长问卷收集其子女的分娩方式、出生体重,父母亲的基本情况和家庭经济收入等资料。
3.指标定义:分娩方式分为阴道产和剖宫产;喂养方式按母乳喂养时间分为母乳喂养(≥6个月)和非母乳喂养(<6个月),其中母乳喂养包括纯母乳、以母乳为主、母乳占50%和以母乳为辅的喂养方式。单胎指一次妊娠子宫腔内只有1个胎儿,多胎指一次妊娠子宫腔内同时有≥2个胎儿;体力活动水平按国际体力活动标准分为轻体力活动和中高等体力活动。父母亲肥胖的判定标准采用“中国肥胖问题工作组”制定的标准,将BMI ≥28.0 kg/m2定义为肥胖[8]。早产指妊娠满28周而不满37周期间分娩的胎儿;足月产指妊娠满37周而不满42周期间分娩的胎儿;过期产指妊娠≥42周分娩的胎儿。6岁和7~17岁组儿童青少年肥胖的判定标准分别按文献[9]和[10]。
4.统计学分析:采用EpiData 3.1软件建立数据库,双录入核查、逻辑检错及清理数据后,采用SPSS 20.0和R软件进行数据分析与统计检验。连续性变量采用x±s的形式,分类变量采用频数(百分比)的形式。采用t检验比较阴道产和剖宫产儿童青少年连续性指标的差异,采用χ2检验比较两组间分类变量的差异,同时考虑到剖宫产率较高,采用Log-Binomial回归模型分析各年龄剖宫产与儿童青少年期肥胖风险的关联。检验水准α=0.05。
结果1.基本情况:研究对象年龄(10.5±3.2)岁,其中出生为阴道产(11.1±3.3)岁,剖宫产(9.7±2.9)岁,差异有统计学意义(P<0.001)。剖宫产者的肥胖率(17.6%)显著高于阴道产者(10.2%)(P<0.001),且剖宫产的出生体重较阴道产高56.9 g(P<0.001)。剖宫产者中男婴的比例显著高于女婴(51.4% :48.6%,P<0.001)、城市地区的比例显著高于乡村(61.8% : 31.8%,P<0.001)。此外,阴道产与剖宫产两者间的喂养方式、胎数、摄入牛奶频率、摄入高能量食物和油炸食品的频率、父母文化程度、家庭经济收入、父母肥胖、体力活动水平和孕周的差异均有统计学意义(P<0.001)。见表 1。

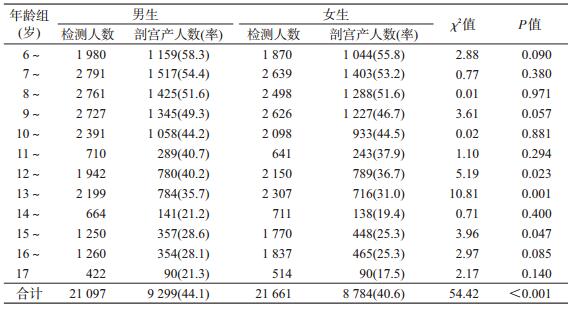
2.剖宫产率的比较:研究对象的剖宫产率男生为44.1%,显著高于女生的40.6%,差异有统计学意义(P<0.001)。按年龄组分析,除12、13和15岁男生的剖宫产率显著高于女生外(P<0.05),其余各年龄组的差异均无统计学意义(P>0.05)。见表 2。
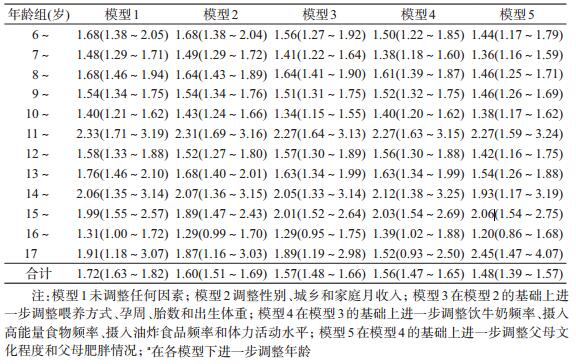
3.剖宫产与儿童青少年期肥胖的关联:以是否肥胖为因变量,分娩方式为自变量进行Log-Binomial回归分析显示(表 3),与阴道产者相比,剖宫产显著增加儿童青少年期肥胖的风险(OR=1.72,95%CI:1.63~1.82;P<0.001)。在调整年龄、性别、城乡、家庭经济月收入、喂养方式、胎数、孕周、出生体重、饮牛奶频率、摄入高能量食物频率、摄入油炸食品频率、体力活动水平、父母文化程度和父母肥胖后,剖宫产仍显著增加儿童青少年期肥胖的发生风险(OR=1.48,95%CI:1.39~1.57;P<0.001)。
本研究发现我国7省份研究对象剖宫产率为42.3%,其中男生(44.1%)显著高于女生(40.6%)。与在新疆地区3~12岁学生中的调查结果一致(男生为55.3%,显著高于女生的44.7%[11])。此外,本研究还发现,剖宫产可显著增加儿童青少年期的肥胖风险(OR=1.72)。这与国内外研究结果一致,如Yuan等[2]分析美国2万余人的队列数据发现,9~28岁剖宫产出生者肥胖的风险是阴道产的1.3倍。吴洁等[11]发现我国新疆地区3~12岁剖宫产出生者肥胖的风险是阴道产的1.7倍。在调整年龄、性别、城乡、家庭经济收入、喂养方式、胎数、孕周、出生体重、饮牛奶频率、摄入高能量食物频率、摄入油炸食品频率、体力活动水平、父母文化程度和父母肥胖等因素后,剖宫产与儿童青少年期更高的肥胖风险(OR=1.48)仍显著相关。提示剖宫产可能会显著增加儿童青少年期发生肥胖的风险。
尽管目前尚不清楚剖宫产增加儿童青少年期肥胖风险的机制,但已有研究发现剖宫产者更高的肥胖风险可能与出生时体内建立的肠道微生物菌群差异有关[12-14]。阴道产者主要暴露于母体阴道和肠道微生物菌群,而剖宫产者主要暴露于母体皮肤微生物群和出生时外部环境菌群[15-17],这种早期不同的微生物传播模式导致了剖宫产者和阴道产者肠道微生物菌群的差异[13]。与阴道产者相比,剖宫产者的肠道微生物菌群中含有较多的葡萄球菌,而含有较少的双歧杆菌。这种肠道菌群模式因具有更强的能量吸收能力而增加后期超重/肥胖的发生风险[13, 18-19]。但这种差异能否维持终身尚需进一步研究证实。
本文存在局限性。如分娩方式资料为母亲自报,未调整产次、选择剖宫产的原因等重要混杂因素,可能会降低剖宫产与后期发生肥胖的关联强度。但考虑到分娩方式明确可辨,错误报告概率较低,其回忆偏倚较小,在一定程度上还是反映了剖宫产与儿童青少年期肥胖风险的关联性。
利益冲突: 无
| [1] |
朱逸博, 李宏田, 刘建蒙.
剖宫产及孕妇要求剖宫产的流行状况[J]. 中国生育健康杂志, 2012, 23(1): 76–78.
Zhu YB, Li HT, Liu JM. Cesarean section and pregnant women require cesarean section of the epidemic situation[J]. Chin J Reprod Heal, 2012, 23(1): 76–78. DOI:10.3969/j.issn.1671-878X.2012.01.039 |
| [2] | Yuan C, Gaskins AJ, Blaine AI, et al. Association between cesarean birth and risk of obesity in offspring in childhood, adolescence, and early adulthood[J]. JAMA Pediatr, 2016, 170(11): e162385. DOI:10.1001/jamapediatrics.2016.2385 |
| [3] | No Authors Listed. Appropriate technology for birth[J]. Lancet, 1985, 2(8452): 436–437. DOI:10.1016/S0140-6736(85)92750-3 |
| [4] | Villar J, Valladares E, Wojdyla D, et al. Caesarean delivery rates and pregnancy outcomes:the 2005 WHO global survey on maternal and perinatal health in Latin America[J]. Lancet, 2006, 367(9525): 1819–1829. DOI:10.1016/S0140-6736(06)68704-7 |
| [5] | Lumbiganon P, Laopaiboon M, Gülmezoglu AM, et al. Method of delivery and pregnancy outcomes in Asia:the WHO global survey on maternal and perinatal health 2007-08[J]. Lancet, 2010, 375(9713): 490–499. DOI:10.1016/S0140-6736(09)61870-5 |
| [6] | Chen YJ, Ma L, Ma YH, et al. A national school-based health lifestyles interventions among Chinese children and adolescents against obesity:rationale, design and methodology of a randomized controlled trial in China[J]. BMC Public Health, 2015, 15(1): 210. DOI:10.1186/s12889-015-1516-9 |
| [7] |
中国学生体质与健康研究组.2010年中国学生体质与健康调研报告[M]. 北京: 高等教育出版社, 2012.
Research group of Chinese students' physique and health.2010 Reports on the physical fitness and health research of Chinese school students[M]. Beijing: Higher Education Press, 2012. |
| [8] |
中国肥胖问题工作组.
中国成人超重和肥胖症预防与控制指南(节录)[J]. 营养学报, 2004, 26(1): 1–4.
Working Group on Obesity in China. Guidelines for prevention and control of overweight and obesity in Chinese adults[J]. Acta Nutrimenta Sinica, 2004, 26(1): 1–4. DOI:10.3321/j.issn:0512-7955.2004.01.001 |
| [9] |
李辉, 宗心南, 季成叶, 等.
中国2~18岁儿童青少年超重和肥胖筛查体重指数界值点的研究[J]. 中华流行病学杂志, 2010, 31(6): 616–620.
Li H, Zong XN, Ji CY, et al. Body mass index cut-offs for overweight and obesity in Chinese children and adolescents aged 2-18 years[J]. Chin J Epidemiol, 2010, 31(6): 616–620. DOI:10.3760/cma.j.issn.0254-6450.2010.06.004 |
| [10] |
中国肥胖问题工作组.
中国学龄儿童青少年超重、肥胖筛查体重指数值分类标准[J]. 中华流行病学杂志, 2004, 25(2): 97–102.
Group of China Obesity Task Force. Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents[J]. Chin J Epidemiol, 2004, 25(2): 97–102. DOI:10.3760/j.issn:0254-6450.2004.02.003 |
| [11] |
吴洁, 阿达力别克, 葛娟, 等.
母亲剖宫产与儿童肥胖的相关性研究[J]. 中国妇幼保健, 2014, 31(29): 5125–5128.
Wu J, Bahetiguli, Ge J, et al. Study on the correlation between cesarean section and childhood obesity[J]. Mat Child Health Care China, 2014, 31(29): 5125–5128. DOI:10.7620/zgfybj.j.issn.1001-4411.2014.31.38 |
| [12] | Barros FC, Matijasevich A, Hallal PC, et al. Cesarean section and risk of obesity in childhood, adolescence, and early adulthood:evidence from 3 Brazilian birth cohorts[J]. Am J Clin Nutr, 2012, 95(2): 465–470. DOI:10.3945/ajcn.111.026401 |
| [13] | Musso G, Gambino R, Cassader M. Obesity, diabetes, and gut microbiota:the hygiene hypothesis expanded?[J]. Diab Care, 2010, 33(10): 2277–2284. DOI:10.2337/dc10-0556 |
| [14] | Neu J, Rushing J. Cesarean versus vaginal delivery:long-term infant outcomes and the hygiene hypothesis[J]. Clin Perinatol, 2011, 38(2): 321–331. DOI:10.1016/j.clp.2011.03.008 |
| [15] | Biasucci G, Benenati B, Morelli L, et al. Cesarean delivery may affect the early biodiversity of intestinal bacteria[J]. J Nutr, 2008, 138(9): 1796S–1800S. |
| [16] | Huurre A, Kalliomäki M, Rautava S, et al. Mode of delivery-effects on gut microbiota and humoral immunity[J]. Neonatology, 2008, 93(4): 236–240. DOI:10.1159/111102 |
| [17] | Dominguez-Bello MG, Costello EK, Contreras M, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns[J]. Proc Natl Acad Sci USA, 2010, 107(26): 11971–11975. DOI:10.1073/pnas.1002601107 |
| [18] | Turnbaugh PJ, Ley RE, Mahowald MA, et al. An obesity-associated gut microbiome with increased capacity for energy harvest[J]. Nature, 2006, 444(7122): 1027–1031. DOI:10.1038/nature05414 |
| [19] | Ajslev TA, Andersen CS, Gamborg M, et al. Childhood overweight after establishment of the gut microbiota:the role of delivery mode, pre-pregnancy weight and early administration of antibiotics[J]. Int J Obes, 2011, 35(4): 522–529. DOI:10.1038/ijo.2011.27 |