 2017, Vol. 38
2017, Vol. 38文章信息
- 高欣, 王临虹, 金叶, 叶鹏鹏, 杨柳, 耳玉亮, 邓晓, 汪媛, 段蕾蕾.
- Gao Xin, Wang Linhong, Jin Ye, Ye Pengpeng, Yang Liu, Er Yuliang, Deng Xiao, Wang Yuan, Duan Leilei.
- 1990年与2013年中国人群自杀疾病负担分析
- Disease burden caused by suicide in the Chinese population, in 1990 and 2013
- 中华流行病学杂志, 2017, 38(10): 1325-1329
- Chinese Journal of Epidemiology, 2017, 38(10): 1325-1329
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2017.10.006
-
文章历史
收稿日期: 2017-03-27




2. 100050 北京, 中国疾病预防控制中心慢性非传染性疾病预防控制中心;
3. 250021 济南市疾病预防控制中心
2. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China;
3. Jinan Center for Disease Control and Prevention, Jinan 250021, China
自杀是一个重要的公共卫生问题,WHO 2014年发布的自杀预防报告指出,世界范围内每40 s就有1个人死于自杀,自杀是15~29岁人群的第二位死亡原因[1]。2014年中国死因监测数据显示,自杀是我国全人群第三位伤害死亡原因,仅次于道路交通事故和意外跌落[2]。全球疾病负担(GBD)研究按照国际疾病分类标准(ICD)综合、系统地提供了疾病负担有关指标,包括分性别、年龄别、国家的年度死亡率、过早死亡损失寿命年(YLL)、伤残损失寿命年(YLD)和伤残调整寿命年(DALY)指标及其变化趋势[3]。该项研究采用统一的测量指标和估算框架,根据自杀发生、致残和死亡等情况,能够系统地反映不同时间、地区和人群的自杀流行状况。本研究基于DALY等相关指标描述中国2013年的自杀疾病负担状况,并比较1990年和2013年中国自杀疾病负担的变化,掌握自杀疾病负担的现状及变化趋势,为防控策略的制定提供依据。
资料与方法1.资料来源:使用数据来自于GBD2013中的中国数据,数据范围为1990-2013年。GBD2013采用统一、可比的方法估算了188个国家的疾病与伤害的寿命损失,对中国死亡的估计数据主要来自于2004-2005年中国第三次死因回顾调查、1989-2011年全国疾病监测点系统死因监测、2002-2007年原卫生部死因统计系统,以及一些已发表的文献或报告,具体研究方法参见文献[3-6]。
2.疾病分类与编码:不同年代不同来源的死因数据,分别采用《疾病和有关健康问题的国际统计分类》ICD-9和ICD-10将死因分类映射到GBD死因分类中。自杀的编码范围:ICD-9:E950~E958;ICD-10:X60~X84。在GBD2013中不能作为根本死因的编码被重新归类至可作为根本死因的分类中[6-7]。
3.分析方法和指标:GBD2013利用多来源的死因监测数据,主要应用死因整体建模策略,估计240种根本死因的死亡数、死亡率[3, 6]。同时,GBD2013综合考虑早死和致残导致的寿命损失,计算YLL、YLD及DALY。YLL的估计方法:将伤害死因别死亡人数乘以期望寿命得到不同年龄组、性别和年份的YLL[8-9];YLD的估计方法:估算自杀患病数,将患病数乘以伤残权重得到YLD,其中伤残权重来自对全球9个国家(孟加拉、印度尼西亚、秘鲁、坦桑尼亚、美国、匈牙利、意大利、瑞典和荷兰)大规模人群调查和网络调查的统计结果并经过非致死性共患疾病的校正[10];DALY=YLL+YLD。年龄别YLL率、YLD率和DALY率的计算为≥10岁人群各年龄组损失寿命年数除以该年龄组人口数。
4.数据分析:本研究使用GBD2013死亡率、YLL、YLD和DALY绝对数等指标,分性别、年龄描述了2013年自杀疾病负担现状;同时,运用GBD2013世界标准人口[5]计算标化死亡率、标化DALY率,以此对1990年与2013年中国自杀的疾病负担变化情况行描述。
结果1.自杀疾病负担:2013年我国≥10岁人群自杀疾病负担各项指标均为男性高于女性。标化自杀死亡率为9.08/10万,男性为10.53/10万,女性为7.64/10万。随年龄增加而升高,≥80岁组自杀死亡率为73.39/10万,约为全人群的8倍。DALYs率随年龄变化出现两个峰值,20~24岁组DALYs率最高,为392.83/10万;35岁后DALYs率随年龄上升而升高,到75~79岁组达到第二个峰值,为559.15/10万。YLDs率随年龄上升而增加,≥80岁组达到最大,为12.13/10万。YLLs率变化同DALYs率变化一致,分别在20~24岁以及75~79岁组出现两个峰值。2013年自杀YLLs/YLDs为90.03,年龄越小,YLLs/YLDs越大,10~14岁组该比值为633.89。男性自杀YLLs/YLDs为89.83,高于女性(89.00),而10~14岁组女性YLLs/YLDs为701.99,高于男性(579.99)。见表 1。

2.自杀死亡疾病负担变化:1990- 2013年我国≥10岁人群自杀死亡率逐渐下降,其中女性下降幅度大于男性(图 1),1990年和1995年,女性自杀死亡率高于男性,随着时间推移,2000年及此后,女性自杀死亡率低于男性。

|
| 图 1 1990-2013年中国人群自杀标化死亡率变化趋势 |
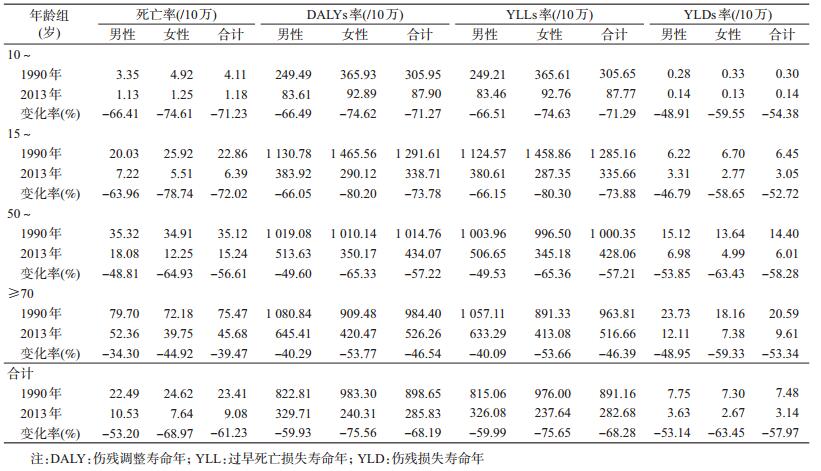
3.自杀疾病负担各指标的变化:相较于1990年,2013年我国≥10岁人群自杀死亡率明显下降,标化自杀死亡率从23.41/10万下降到9.08/10万,女性下降了68.97%,下降幅度大于男性(53.20%),15~49岁组下降最明显,死亡率下降了72.02%,≥70岁组下降了39.47%,在各年龄段中下降幅度最低。DALYs率和YLLs率变化同死亡率变化一致,均为女性下降幅度大于男性,≥70岁组下降幅度最低,15~49岁组下降幅度最高,而YLDs率则为50~69岁组下降幅度最大。见表 2。
本研究结果显示,从1990-2013年,我国自杀率、DALYs、YLLs及YLDs都大幅下降,下降水平列居G20国家的第一位。自杀与社会环境(包括经济危机、政治危机、社会动荡、工作变迁、生活变化等)密切相关[11]。我国自杀的减少反映了我国相关法律、政策的成效,及我国社会文明的进步和社会稳定的良性发展。随着我国物质文明和精神文明的不断推进,自杀的相关危险因素得到了不同程度的控制。我国的《中华人民共和国枪支管理法》[12]、《农药管理条例》[13]、《麻醉药品和精神药品管理条例》[14]等法律法规,有利于限制自杀工具的可获得性,从而减少自杀的发生。Phillips等[15]研究结果显示,在所有自杀死亡者中,40%为抑郁症,7%为精神分裂症,7%为酒精依赖。中国政府高度重视精神卫生工作,先后采取一系列政策措施,推动了精神卫生事业发展,深入开展的严重精神障碍管理治疗工作取得了显著成效,截至2014年底,全国已登记在册严重精神障碍患者430万人,其中73.2%的患者接受了基层医疗卫生机构提供的随访管理及康复指导服务[16]。从1990-2013年,我国自杀死亡率下降了61.23%,特别是女性下降了68.97%,可能是随着城镇化脚步的迈进,女性的婚姻自由、工作权利不断提高,信息交流途径不断扩展[17-18],从而处理负性生活事件的资源增加,减少了自杀的发生。此外,遭受暴力也将增加自杀的风险[1],2006-2013年,全国死因监测系统中暴力的粗死亡率下降了46.3%,全国伤害监测系统中暴力病例占所有伤害病例的比例下降了49.2%[19-20]。
研究发现2013年我国老年人自杀死亡率、DALYs率、YLLs率及YLDs率均高于其他年龄人群,且从1990-2013年,老年人自杀率降低幅度低于其他年龄人群。GBD2015数据显示[21],在金砖5国(中国、俄罗斯、巴西、印度和南非)中,70岁以上老年人死亡率中国最低,而70岁以上老年人自杀死亡率中国最高。我国老年人自杀问题已非常严峻,老年人是我国自杀防控应最优先关注的群体。工作和财富丧失、歧视、隔离、精神障碍、慢性疼痛与疾病、丧失(亲人去世)等都是自杀的危险因素[1],而老年人正是暴露于这些危险因素的脆弱人群。目前中国家庭小型化,独生子女状态可能会冲击我国传统的居家养老模式,影响到老年人的家庭环境,从而对老年人的健康与健康需求产生更多的影响,老年人中还有一些特定的弱势群体:如高龄、独居、伤残老人[22],这些都影响着老年人的身体和精神健康。老年人随着年龄的增长,暴露于危险因素的时间延长,由于机体器官老化、抗病能力减弱,慢性病患病危险性随之增高[23]。在慢性病患者中抑郁症比例远高于一般人群,其中老年慢性病患者更高,刘同洲等[24]对综合医院住院患者抑郁障碍患病率调查显示,>65岁者中45.6%有抑郁,<25岁者中29.4%有抑郁,而我国人群抑郁症患病率为6.1%[25]。有研究显示自杀死亡老年人中有90%以上患有抑郁症或精神障碍[26]。对于老年人自杀的防控,应从个人身心健康、家庭环境、社区社会服务等多方面考虑,致力于实现老有所养、老有所医、老有所为、老有所学、老有所乐。
分析发现,2013年≥10岁人群男性自杀YLL/YLD为89.83,女性YLL/YLD为89.00,意味着自杀的致死性高、后果极为严重,对于自杀的防控还应强调降低自杀严重性的相关策略。全国伤害监测系统数据显示农村自残/自杀者中高达72.0%选择服毒的方式,提示应进一步加强对现有管理条例、办法的执行力度,特别是对农村剧毒、高毒农药的管理[27]。自杀未遂史是再次自杀的高危因素,我国自杀死亡者中27%有自杀未遂史[28]。我国60.8%的自残/自杀就诊者在门/急诊后仍然会留在医院(观察、住院或转院),这意味着我国具备对自杀未遂者进行再次自杀干预的时间和空间条件,应利用其在院期间进行心理评估和干预,并建立更为长期的治疗、随访关系,预防自杀行为的再次发生[27]。此外,自杀未遂者难以发现可能是YLL/YLD高的另外一个原因,由于“家丑不可外扬”、对精神疾病的歧视以及对于医保不承担自杀所致的医疗费用等原因,自杀问题的暴露如冰山一角,很多未出现严重后果的自杀未遂者无法被发现。故对于自杀的预防,还应关注隐匿的自杀人群,包括增加社会关爱,鼓励精神障碍患者及时治疗等。
本研究采用GBD2013描述了中国人群自杀疾病负担及变化情况,在其方法学及内容涵盖范围方面尚有局限性。GBD数据的来源及估计方法有其不确定性,来自医疗系统的死亡数据缺乏死因细分类或准确性不高,国家数据的差异(如高收入国家与低收入国家的信息系统质量、传染性疾病与非传染性疾病发病率的差异)会影响GBD数据的估算以及国别间的可比性[4]。由于我国自杀发生的数据较为缺乏,GBD对我国自杀疾病负担的估计将会产生一定的影响。本研究主要呈现了不同人群间自杀所致的死亡及寿命损失等情况,并未呈现自杀原因、手段、时点、地点等特征,对于确定自杀危险因素以及提出基于证据的防控优先领域,还需要更多的相关研究。
利益冲突: 无
| [1] | World Health Organization.Preventing Suicide:A Global Imperative[M]. Geneva: World Health Organization, 2014. |
| [2] |
国家卫生和计划生育委员会统计信息中心, 中国疾病预防控制中心慢性非传染性疾病预防控制中心.中国死因监测数据集2014[M]. 北京: 科学普及出版社, 2015: 12.
Statistical Information Center, National Health and Family Planning Commission of the People's Republic of China, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention.China death surveillance database 2014[M]. Beijing: Popular Science Press, 2015: 12. |
| [3] | GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013:a systematic analysis for the Global Burden of Disease Study 2013[J]. Lancet, 2015, 385(9963): 117–171. DOI:10.1016/S0140-6736(14)61682-2 |
| [4] | Murray CJL, Lopez AD. Measuring the global burden of disease[J]. N Eng J Med, 2013, 369(5): 448–457. DOI:10.1056/NEJMra1201534 |
| [5] | GBD 2013 DALYs and HALE Collaborators, Murray CJL, Barber RM, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013:quantifying the epidemiological transition[J]. Lancet, 2015, 386(10009): 2145–2191. DOI:10.1016/S0140-6736(15)61340-X |
| [6] | Zhou MG, Wang HD, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990-2013:a systematic subnational analysis for the Global Burden of Disease Study 2013[J]. Lancet, 2016, 387(10015): 251–272. DOI:10.1016/S0140-6736(15)00551-6 |
| [7] | Haagsma JA, Graetz N, Bolliger I, et al. The global burden of injury:incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013[J]. Inj Prev, 2016, 22(1): 3–18. DOI:10.1136/injuryprev-2015-041616 |
| [8] | Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet, 2012, 380(9859): 2095–2128. DOI:10.1016/S0140-6736(12)61728-0 |
| [9] | Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet, 2013, 380(9859): 2163–2196. DOI:10.1016/S0140-6736(12)61729-2 |
| [10] | Haagsma JA, de Noordhout CM, Polinder S, et al. Assessing disability weights based on the responses of 30660 people from four European countries[J]. Popul Health Metr, 2015, 13: 10. DOI:10.1186/s12963-015-0042-4 |
| [11] |
郗春嫒.
《自杀论》及其方法论解读[J]. 中北大学学报:社会科学版, 2009, 25(5): 80–82, 86.
Xi CA. On suicide and its interpretation of the methodology[J]. J North Univ of China:Social Science Edition, 2009, 25(5): 80–82, 86. DOI:10.3969/j.issn.1673-1646.2009.05.021 |
| [12] |
中华人民共和国枪支管理法[Z]. 2015.
Law of the People's Republic of China on the control of firearms[Z]. 2015. |
| [13] |
中华人民共和国国务院. 农药管理条例[Z]. 2017.
The State Council of the People's Republic of China. Regulations on the control of agricultural chemicals[Z]. 2017. |
| [14] |
中华人民共和国国务院. 令第442号麻醉药品和精神药品管理条例[S]. 北京: 中华人民共和国国务院, 2005.
The State Council of the People's Republic of China. Decree No.442 Regulations on the administration of narcotics and psychotropic drugs[S]. Beijing:The State Council of People's Republic of China, 2005. |
| [15] | Phillips MR, Yang GH, Zhang YP, et al. Risk factors for suicide in China:a national case-control psychological autopsy study[J]. Lancet, 2002, 360(9347): 1728–1736. DOI:10.1016/S0140-6736(02)11681-3 |
| [16] |
国务院办公厅. 国办发[2015] 44号国务院办公厅关于转发卫生计生委等部门全国精神卫生工作规划(2015-2020年)的通知[S]. 北京: 国务院办公厅, 2015.
General Office of the State Council of the People's Republic of China. Issued 2015 No.44 The general office of the State Council on Forwarding health and Family Planning Commission and other departments of the planning work of mental health (2015-2020)[S]. Beijing:General Office of the State Council of the People's Republic of China, 2015. |
| [17] |
杨功焕, 周灵妮, 黄正京, 等.
中国人群自杀水平的变化趋势和地理分布特点[J]. 中华流行病学杂志, 2004, 25(4): 280–284.
Yang GH, Zhou LN, Huang ZJ, et al. The trend and geographic distribution of suicide in Chinese population[J]. Chin J Epidemiol, 2004, 25(4): 280–284. DOI:10.3760/j.issn.0254-6450.2004.04.002 |
| [18] | Yip PSF, Liu KY, Hu JP, et al. Suicide rates in China during a decade of rapid social changes[J]. Soc Psychiatry Psychiatr Epidemiol, 2005, 40(10): 792–798. DOI:10.1007/s00127-005-0952-8 |
| [19] |
高欣, 叶鹏鹏, 耳玉亮, 等.
2006-2013年全国伤害监测系统中因暴力就诊病例特征分析[J]. 中华流行病学杂志, 2015, 36(1): 3–6.
Gao X, Ye PP, Er YL, et al. Analysis on the characteristics of violence based on data from the Chinese National Injury Surveillance System from 2006 to 2013[J]. Chin J Epidemiol, 2015, 36(1): 3–6. DOI:10.3760/cma.j.issn.0254-6450.2015.01.002 |
| [20] |
耳玉亮, 高欣, 段蕾蕾, 等.
我国暴力流行及预防控制现状分析[J]. 中华流行病学杂志, 2016, 37(1): 5–9.
Er YL, Gao X, Duan LL, et al. Analysis on violence injury incidence and prevention in China[J]. Chin J Epidemiol, 2016, 37(1): 5–9. DOI:10.3760/cma.j.issn.0254-6450.2016.01.002 |
| [21] | Institute for Health Metrics and Evaluation. GBD 2015. Both sexes, 70+years, 2015, Deaths per 100000[EB/OL] [2017-03-03]. https://vizhub.healthdata.org/gbd-compare/. |
| [22] |
"健康中国2020"战略研究报告编委会."健康中国2020战略"研究报告[M]. 北京: 人民卫生出版社, 2012.
Health Chinese 2020" Strategic Research Report Editor Committee."Health China 2020" Strategy Research Report[M]. Beijing: People's Medical Publishing House, 2012. |
| [23] |
刘竟芳, 陈哲, 杨非柯, 等.
长沙市社区老年人慢性病现状[J]. 中华老年医学杂志, 2014, 34(11): 3115–3117.
Liu JF, Chen Z, Yang FK, et al. Current status of chronic diseases in the elderly in Changsha[J]. Chin J Geriatr, 2014, 34(11): 3115–3117. DOI:10.3969/j.issn.1005-9202.2014.11.095 |
| [24] |
刘同洲, 韩建波, 刘兰芬, 等.
综合医院住院患者抑郁障碍患病率调查[J]. 精神医学杂志, 2009, 22(5): 331–333.
Liu TZ, Han JB, Liu LF, et al. Prevalence of depressive disorder of inpatients in general hospital[J]. J Psychiatry, 2009, 22(5): 331–333. DOI:10.3969/j.issn.1009-7201.2009.05.004 |
| [25] | Phillips MR, Zhang JX, Shi QC, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-05:an epidemiological survey[J]. Lancet, 2009, 373(9680): 2041–2053. DOI:10.1016/S0140-6736(09)60660-7 |
| [26] | Wright PP, Thorpe CW. Triple threat among the elderly:depression, suicide risk, and handguns[J]. Journal of Emergency Nursing, 2016, 42(1): 14–18. DOI:10.1016/j.jen.2015.01.010 |
| [27] |
高欣, 段蕾蕾, 杨超, 等.
2006-2013年全国伤害监测系统中自残/自杀病例特征分析[J]. 中华流行病学杂志, 2015, 36(1): 17–19.
Gao X, Duan LL, Yang C, et al. Analysis on the characteristics of self-inflicted injury/suicide based on the Chinese National Injury Surveillance System from 2006 to 2013[J]. Chin J Epidemiol, 2015, 36(1): 17–19. DOI:10.3760/cma.j.issn.0254-6450.2015.01.005 |
| [28] |
秦霞.
自杀未遂相关因素与心理干预的研究进展[J]. 中国现代药物应用, 2013, 7(20): 241.
Qin X. Research progress of related factors of and psychological intervention of suicide attempt[J]. Chin J Mod Drug Appl, 2013, 7(20): 241. |