 2017, Vol. 38
2017, Vol. 38文章信息
- 陈志华, 张梅, 李镒冲, 黄正京, 王丽敏.
- Chen Zhihua, Zhang Mei, Li Yichong, Huang Zhengjing, Wang Limin.
- 2012年中国流动人口慢性病危险因素聚集性及其影响因素分析
- Co-prevalence of chronic disease risk factors and influencing factors in floating population in China
- 中华流行病学杂志, 2017, 38(9): 1226-1230
- Chinese journal of Epidemiology, 2017, 38(9): 1226-1230
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2017.09.017
-
文章历史
收稿日期: 2017-01-12




慢性非传染性疾病(慢性病)已成为导致我国居民死亡的主要原因[1-3]。随着个人慢性病危险因素数量增加,不良健康后果的风险也随之增加,而遵循健康的行为生活方式,会大幅降低早死风险,且能减少慢性病发生[4-6]。而城市化和工业化的发展导致人口大规模流动,目前我国已具有总人口1/6的流动人口[7]。针对流动人口调查发现其中大多是收入较低、文化程度不高、社会保障缺乏,为从农村流向城市的青壮年劳动力人口[7];与常住居民相比,其特征上的差异可能使慢性病危险因素在流动人口中更广泛流行,从而导致慢性病疾病负担增加。为此本文分析流动人口慢性病危险因素流行现状、聚集性及其影响因素,为流动人口慢性病干预提供科学依据。
资料与方法1.样本数据:源自中国慢性病及其危险因素监测(2012)流动人口专题调查。该调查在全国31个省(自治区、直辖市)和新疆生产建设兵团共170个县(区、团)开展,每个调查县(区、团)内按6类行业(制造业、批发零售业、住宿餐饮业、社会服务业、建筑业和其他)分层整群等额抽样,即每类行业调查选取至少50人,每个调查县(区、团)不得少于300人,全国共预计调查51 000人。调查对象为≥18岁就业流动人口(即外来务工或经商人员),并符合:① 居住地和户口登记所在县(区、团)不同,但排除同一市内跨区人口;② 过去12个月内,在调查县(区、团)居住>6个月。学生、无业人员、探亲访友者等外来人口不纳入调查。由于≥60岁调查对象很少,本文仅分析18~59岁流动人口。
2.调查内容及相关定义:通过问卷询问一般情况、吸烟、饮酒、饮食、身体活动状况等信息。同时测量被调查者的身高和在清晨空腹体重,并计算BMI。5类危险因素定义:① 现在吸烟者是指被调查时吸烟。② 根据WHO《国际酒精消费和相关损害监测指南》推荐的标准[8-9],不健康饮酒行为包括危险饮酒和有害饮酒;危险饮酒指男性饮酒者日均酒精摄入量≥41 g且<61 g的饮酒行为,女性饮酒者日均酒精摄入量≥21 g且<41 g的饮酒行为;有害饮酒定义为男性饮酒者日均酒精摄入量≥61 g,女性饮酒者日均酒精摄入量≥41 g的饮酒行为。本研究将男性饮酒者日均酒精摄入量≥41 g,女性饮酒者日均酒精摄入量≥21 g的行为视为过量饮酒,即过量饮酒者等于危险饮酒者加上有害饮酒者。③ 从不锻炼者是指通常1周内业余时间从不参加锻炼者。④ 根据WHO推荐标准,蔬菜水果摄入不足是指日均蔬菜水果摄入<400 g者[10]。⑤ 按照《中国成人超重和肥胖症预防控制指南》标准,超重/肥胖是指BMI≥24 kg/m2。
3.统计学分析:为减少调查样本与目标总体结构上的偏差所导致的估计偏倚,本文采用《流动人口动态监测调查数据(2012)》 [11]对调查样本的年龄、性别和行业进行事后分层调整。将危险因素数量分成“0个”、“1个”、“2个”、“≥3个”四个等级,采用秩和检验分析,用指标秩和检验参数——mean score比较各亚组间危险因素数量分布是否存在差异(其值越高表示该亚组人群分布越集中在危险因素数量等级高处,反之则分布集中在危险因素数量等级低处),并将有序分组资料做Spearman秩相关分析,以P<0.05为差异有统计学意义。统计分析采用SAS 9.4软件。
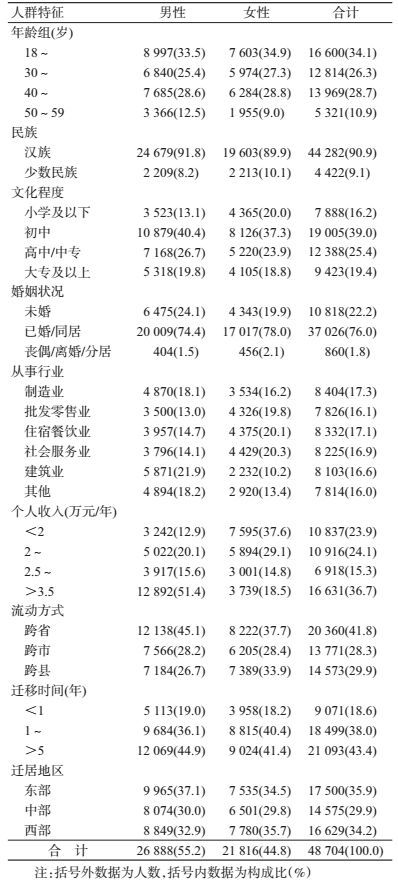
结果1.一般情况:共48 704人纳入分析,其中男性占55.2%(26 888人),女性占44.8%(21 816人);年龄以18~29岁为主(34.1%,16 600人);汉族占90.9%(44 282人);文化程度以初中为主(39.0%,19 005人);婚姻状况以未婚为主(22.2%,10 818人);各行业流动人口数量基本一致(本次调查采用分行业等额抽样);年收入存在性别差异,男性以>3.5万元为主(51.4%,12 892人),女性以<2万元为主(37.6%,7 595人);流动方式以跨省迁移为主(41.8%,20 360人);迁移时间以>5年为主(43.4%,21 093人);迁居地区以东部为主(35.9%,17 500人)。见表 1。
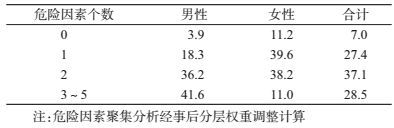
2.危险因素流行率:18~59岁流动人口现在吸烟率为32.5%,其中男性(55.3%)明显高于女性(1.9%);饮酒者中过量饮酒率为11.0%,其中男性(13.5%)明显高于女性(3.8%);蔬菜水果摄入不足比例为44.1%,其中男性为46.2%、女性为41.2%;从不锻炼率在不同性别人群中均较高,男性为69.3%、女性为74.1%;超重/肥胖率为41.3%,其中男性(48.6%)明显高于女性(31.4%)。见表 2。分析个人危险因素聚集数量,27.4%的样本人群具有1种危险因素,37.1%具有2种危险因素,28.5%具有≥3种危险因素(表 3)。

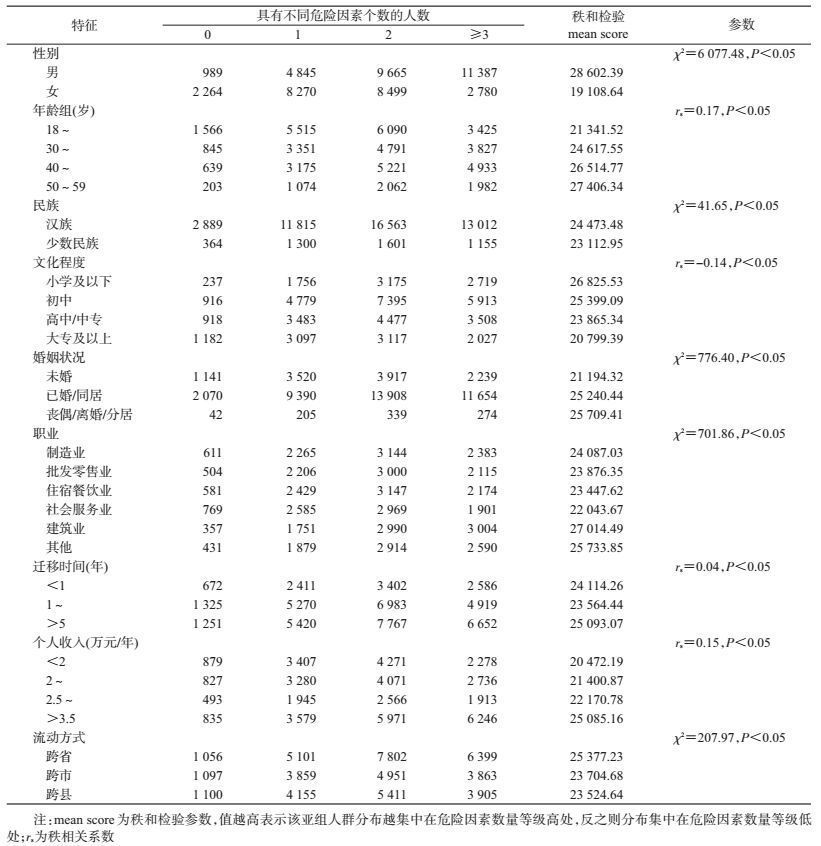
3.不同亚组间危险因素数量秩和检验和有序分组资料秩相关分析:不同性别、民族、婚姻状况、行业及流动方式的危险因素数量分布差异有统计学意义(P<0.000 1)。男性流动人口危险因素数量mean score高于女性;汉族流动人口危险因素数量mean score比少数民族高;已婚/同居、丧偶/离婚/分居状态流动人口危险因素数量mean score比未婚者高;同行业流动人口危险因素数量mean score以建筑业最高,跨省流动者危险因素数量mean score高于跨市或跨县流动者。将年龄、文化程度、年收入和迁移时间4个变量与危险因素数量做秩相关分析,结果发现:危险因素数量与年龄(rs=0.17,P<0.05)、收入(rs=0.15,P<0.05)和迁移时间(rs=0.04,P<0.05)呈正相关,与文化程度(rs=-0.14,P<0.05)呈负相关(表 4)。
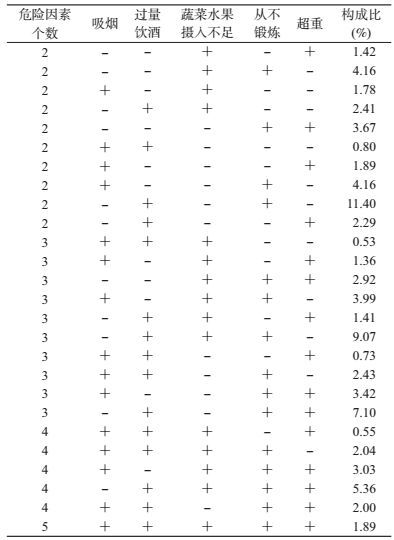
4.聚集模式分析:具有4项危险因素的流动人口,以过量饮酒、蔬菜水果摄入不足、从不锻炼合并超重模式最常见,为5.36%;有3项危险因素者,以过量饮酒、蔬菜水果摄入不足合并从不锻炼模式最常见,为9.07%;过量饮酒合并从不锻炼是有2项危险因素的流动人口最常见的聚集模式,占11.40%(表 5)。
本次分析发现2012年我国18~59岁流动人口慢性病5类危险因素十分普遍,男性普遍存在吸烟行为,现在吸烟率为55.3%,但女性吸烟率呈较低水平(1.9%);过量饮酒占11.0%,其中男性高于女性;而蔬菜水果摄入不足(44.1%)和业余时间从不锻炼(71.3%)现象严重;超重/肥胖率亦呈较高水平(41.3%)。各项危险因素流行率与国内既往关于流动人口的调查结果基本一致[12-15]。表明流动人口将面临慢性病患病的潜在巨大风险,将成为未来我国公共卫生工作的巨大挑战。
危险因素聚集性分析显示,37.1%的流动人口具有2种危险因素,28.5%具有≥3种危险因素,可见该人群危险因素聚集现象较严重。分析中还发现年长、汉族、男性、建筑业、跨省流动和迁移时间越长的流动人口可能聚集更多危险因素。在发达国家已有较多关于危险因素聚集性的研究,发现一种危险因素常伴随另一种危险因素同时存在,通常以某种特定组合模式出现[16-19]。从干预角度看,若危险因素间存在关联并以某种模式聚集,仅对单个危险因素进行干预,很可能达不到预期效果,有研究建议将单一危险因素干预扩大到多项危险因素干预,将具有更好的成本效益[20]。本文中不同数量危险因素最常见的聚集模式是以过量饮酒、从不锻炼、超重/肥胖3项危险因素至少同时存在2项。因此,对流动人口尤其过量饮酒、从不锻炼、超重/肥胖者实施多项危险因素的综合干预是解决其慢性病问题的有效策略。
社会经济地位主要衡量要素包括收入、受教育程度和职业[21]。本次调查样本中初中及以下文化程度的流动人口占55.4%,个人年收入低于3.5万元者占63.3%,大多集中在第二、三产业中劳动强度大、技术含量低的职业,社会经济地位普遍较低。分析中发现社会经济地位对流动人口危险因素聚集性影响显著,表现为危险因素的数量随个人年收入增加而增加,随着文化程度的降低而升高,前者与Li等[22]对常住居民的研究结论存在差异,后者一致。因此,在针对流动人口不健康行为干预时,应重点关注文化水平低、收入较高者。
本研究存在局限性。由于流动人口大多数从事中高强度体力工作,因此身体活动不足以“业余时间从不锻炼”衡量,在一定程度上被高估。但业余时间身体锻炼是被公认的慢性病保护因素,若流动人口形成了业余时间不锻炼的生活习惯,即使工作强度降低,也难改变此习惯,因此了解流动人口这一指标的流行情况并进行身体活动的健康教育是必要的。
综上所述,我国流动人口一方面慢性病相关危险因素广泛流行且聚集现象严重,另一方面社会经济地位普遍较低,若不及时采取流动人口不健康行为综合性干预措施,最终有可能导致健康不公平加剧。
利益冲突: 无
| [1] | GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015:a systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet, 2016, 388(10053): 1459–1544. DOI:10.1016/S0140-6736(16)31012-1 |
| [2] | GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015:a systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet, 2016, 388(10053): 1659–1724. DOI:10.1016/S0140-6736(16)31679-8 |
| [3] |
中国疾病预防控制中心慢性非传染性疾病预防控制中心.中国死因监测数据集2014[M]. 北京: 科学普及出版社, 2015.
National Center for Chronic and Non-Communicable Disease Chinese Center for Disease Control and Prevention.National Disease Surveillance Points System:Death Cause Data Set (2014)[M]. Beijing: Popular Science Press, 2015. |
| [4] | Khaw KT, Wareham N, Bingham S, et al. Combined impact of health behaviours and mortality in men and women:the EPIC-Norfolk prospective population study[J]. PLoS Med, 2008, 5(1): e12. DOI:10.1371/journal.pmed.0050012 |
| [5] | Li YC, Feng XQ, Zhang M, et al. Clustering of cardiovascular behavioral risk factors and blood pressure among people diagnosed with hypertension:a nationally representative survey in China[J]. Sci Rep, 2016, 6: 27627. DOI:10.1038/srep27627 |
| [6] | Martínez-Gómez D, Guallar-Castillón P, León-Mu?oz LM, et al. Combined impact of traditional and non-traditional health behaviors on mortality:a national prospective cohort study in Spanish older adults[J]. BMC Med, 2013, 11(1): 47. DOI:10.1186/1741-7015-11-47 |
| [7] |
国家人口和计划生育委员会流动人口服务管理司.中国流动人口发展报告2016[M]. 北京: 中国人口出版社, 2016.
Department of Service and Management for Migrant Populayion on National Health and Family Planning Commission of the PRC.Report on China's Migrant Population Development 2016[M]. Beijing: China Population Publishing House, 2016. |
| [8] | World Health Organization.International Guide for Monitoring Alcohol Consumption and Related Harm[M]. Geneva: World Health Organization, 2000: 54. |
| [9] | English DR, Holman CDJ, Milne E, et al.The Quantification of Drug-caused Morbidity and Mortality in Australia, 1995[M]. Canberra: Commonwealth Department of Human Services and Health, 1995. |
| [10] | WHO/FAO. Diet, nutrition and the prevention of chronic diseases report of the joint WHO/FAO expert consultation[R]. WHO Technical Report Series No. 916, Geneva:World Health Organization, 2003. |
| [11] |
国家人口和计划生育委员会流动人口服务管理司.中国流动人口发展报告2012[M]. 北京: 中国人口出版社, 2012.
Department of Service and Management for Migrant Population on National Health and Family Planning Commission of the PRC.Report on China's Migrant Population Development 2012[M]. Beijing: China Population Publishing House, 2012. |
| [12] | Wan X, Shin SS, Wang Q, et al. Smoking among young rural to urban migrant women in China:a cross-sectional survey[J]. PLoS One, 2011, 6(8): e23028. DOI:10.1371/journal.pone.0023028 |
| [13] |
禹震, 乔磊, 王旭红, 等.
北京市某区流动人口危害健康行为的现况调查[J]. 中国慢性病预防与控制, 2010, 18(5): 448–451.
Yu Z, Qiao L, Wang XH, et al. Investigation on health-threatening behaviors among the immigrants living in an urban district of Beijing[J]. Chin J Prev Contr Chronic Non-Commun Dis, 2010, 18(5): 448–451. DOI:10.16386/j.cjpccd.issn.1004-6194.2010.05.013 |
| [14] |
霍小宁, 杨小龙, 吕红波.
兰州市男性农民工和城区工人饮酒状况对照研究[J]. 中国药物滥用防治杂志, 2013, 19(1): 20–24.
Huo XN, Yang XL, Lv HB. Lanzhou city male migrant workers and urban workers drinking status control study[J]. Chin J Drug Abuse Prev Treat, 2013, 19(1): 20–24. DOI:10.3969/j.issn.1006-902X.2013.01.005 |
| [15] |
周庆誉, 翁昊艺, 郭静.
青年流动人口健康知识水平与行为形成状况调查[J]. 中国公共卫生, 2014, 30(9): 1157–1159.
Zhou QY, Weng HY, Guo J. Health knowledge and behavior among young migrants[J]. Chin J Public Health, 2014, 30(9): 1157–1159. DOI:10.11847/zgggws2014-30-09-15 |
| [16] | van Nieuwenhuijzen M, Junger M, Velderman MK. Clustering of health-compromising behavior and delinquency in adolescents and adults in the Dutch population[J]. Prev Med, 2009, 48(6): 572–578. DOI:10.1016/j.ypmed.2009.04.008 |
| [17] | McAloney K, Graham H, Law C, et al. A scoping review of statistical approaches to the analysis of multiple health-related behaviours[J]. Prev Med, 2013, 56(6): 365–371. DOI:10.1016/j.ypmed.2013.03.002 |
| [18] | Alamian A, Paradis G. Individual and social determinants of multiple chronic disease behavioral risk factors among youth[J]. BMC Public Health, 2012, 12(1): 224. DOI:10.1186/1471-2458-12-224 |
| [19] | Ottevaere C, Huybrechts I, Benser J, et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents:the HELENA study[J]. BMC Public Health, 2011, 11(1): 328. DOI:10.1186/1471-2458-11-328 |
| [20] | Cecchini M, Sassi F, Lauer JA, et al. Tackling of unhealthy diets, physical inactivity, and obesity:health effects and cost-effectiveness[J]. Lancet, 2010, 376(9754): 1775–1784. DOI:10.1016/S0140-6736(10)61514-0 |
| [21] |
马玉霞, 张兵.
社会经济地位测量方法的研究进展[J]. 中国健康教育, 2011, 27(5): 372–376, 386.
Ma YX, Zhang B. The review of progress on measurement of socioeconomic status[J]. Chin J Health Educat, 2011, 27(5): 372–376, 386. DOI:10.16168/j.cnki.issn.1002-9982.2011.05.015 |
| [22] | Li YC, Zhang M, Jiang Y, et al. Co-variations and clustering of chronic disease behavioral risk factors in China:China chronic disease and risk factor surveillance, 2007[J]. PLoS One, 2012, 7(3): e33881. DOI:10.1371/journal.pone.0033881 |