 2017, Vol. 38
2017, Vol. 38文章信息
- 王佳丽, 陈祚, 张林峰, 王馨, 董莹, 聂静雨, 郑聪毅, 邵澜, 田野, 王增武, 代表西藏与新疆地区慢性心肺疾病现状调查研究项目组.
- Wang Jiali, Chen Zuo, Zhang Linfeng, Wang Xin, Dong Ying, Nie Jingyu, Zheng Congyi, Shao Lan, Tian Ye, Wang Zengwu, for the Group of Study on Prevalence of Chronic Cardiopulmonary Disease in Tibet and Xinjiang Area.
- 新疆、西藏地区35岁及以上人群身体脂肪率、内脏脂肪指数与心脏代谢性危险因素聚集的关系
- Association between body fat percentage, visceral fat index and cardiometabolic risk factor clustering among population aged 35 year old or over, in Tibet Autonomous Region and Xinjiang Uygur Autonomous Region
- 中华流行病学杂志, 2017, 38(6): 727-731
- Chinese Journal of Epidemiology, 2017, 38(6): 727-731
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2017.06.007
-
文章历史
收稿日期: 2017-02-03




肥胖与心血管疾病危险因素及其聚集密切相关,尤其是中心性肥胖[1-2]。我国人群超重、肥胖患病率呈持续上升趋势[3]。肥胖相关慢性疾病的发病率和死亡率亦显著增加。肥胖已成为重要公共卫生问题。目前普遍采用BMI和腰围(WC)作为评价肥胖及内脏脂肪蓄积的指标。有研究提示身体脂肪率(body fat percentage,BFP)和内脏脂肪指数(visceral fat index,VFI)对心脏代谢性危险因素的预测效果可能更优[4-9],但目前尚无定论[10]。在我国人群中,尤其是新疆、西藏,BFP和VFI的应用价值尚缺乏充分证据。本研究利用新疆、西藏项目调查人群的数据进行分析,探讨BFP和VFI与心脏代谢性危险因素聚集的关系及其预测价值。
对象与方法1.研究对象:本研究采用分层多阶段随机抽样。首先分别在西藏自治区和新疆维吾尔自治区内按城乡分为2层,在每层内采用与容量大小成比例的概率(PPS)抽取所需数量的区/县;然后在被抽中的区/县中采用简单随机抽样(SRS)方法抽取2个街道/乡镇;再在被抽中的街道/乡镇中采用SRS法抽取3个居/村委会;最后在被抽中的居/村委会中分性别、年龄采用SRS方法随机抽取调查≥15岁个体,并对≥35岁个体采集空腹血标本。抽取新疆7个地区,西藏6个地区。本研究实际入选≥35岁调查对象7 571人,对数据完整的5 643人进行分析。本项研究通过中国医学科学院阜外医院伦理委员会批准,所有参加对象均签署知情同意书。
2.研究方法:采用横断面调查方法收集资料。内容包括问卷调查、体格检查和实验室检查。
(1)调查问卷内容包括:① 基本信息:年龄、性别、婚姻状况、文化程度、行为习惯(吸烟、饮酒等);② 疾病史:如脑卒中、糖尿病、血脂异常等。
(2)体格检查:① 血压:采用电子血压计(欧姆龙HBP-1300),要求调查对象在测量前30 min禁止剧烈活动或饮茶咖啡等兴奋性饮料,选择测量右上臂的血压,测量前静坐5 min。需连续测量3次,每两次间隔30 s,取平均值作为个体的血压值;② 体重、BFP和VFI:采用生物电阻抗法体重体脂测量仪(欧姆龙V-BODY HBF-371)测量,此类仪器可以准确地测量PBF和VFI[11]。
(3)实验室标本:采集空腹12 h血标本,测量FPG、TC、TG、HDL-C等生化指标。所有标本先保存于-70 ℃冰箱,由统一的实验室进行化验检测。所有生化检查采用美国贝克曼库尔特有限公司(Beckman Coulter,Inc.)AU400自动生化分析仪和试剂。血糖采用葡萄糖氧化酶——过氧化物偶联体系(GOP-POD)方法测定,血脂采用酶法测定。
3.诊断标准:① 高血压诊断标准采用2010年中国高血压防治指南推荐的标准:SBP≥140 mmHg(1 mmHg=0.133 kPa)或DBP≥90 mmHg,对既往确诊的高血压患者或在两周内服用过降压药者,不论检查时血压是否异常均诊断为高血压;② 糖尿病定义为既往确诊或实验室检查FPG≥7.0 mmol/L定义为糖尿病;③ 血脂异常采用2007年中国成人血脂异常指南推荐的标准:高甘油三酯血症定义为TG≥2.26 mmol /L,低高密度脂蛋白胆固醇血症定义为HDL-C<1.04 mmol /L;④ 危险因素聚集指在上述4项危险因素中,同一个体同时具有2项及以上危险因素;⑤ 吸烟者定义为平均每日吸烟1支及以上,并连续吸1年以上;⑥ 饮酒定义为最近1个月每周至少饮酒1次。
4.质量控制:调查中采用统一的调查方案、手册及问卷。调查前,牵头单位负责组织各调查单位所有项目参与人员集中培训和考核。考核合格后方可参加调查。
5.统计学分析:采用EpiData 3.1软件建立数据库,SAS 9.3及MedCalc 17.0.4软件进行统计学分析。计量资料使用x±s表示,计数资料用人数和构成比(%)描述。采用非条件logistic回归模型分析BFP、VFI与危险因素聚集的关系。采用受试者工作特征(ROC)曲线比较BFP和VFI对危险因素聚集的预测价值。以P<0.05为差异有统计学意义。
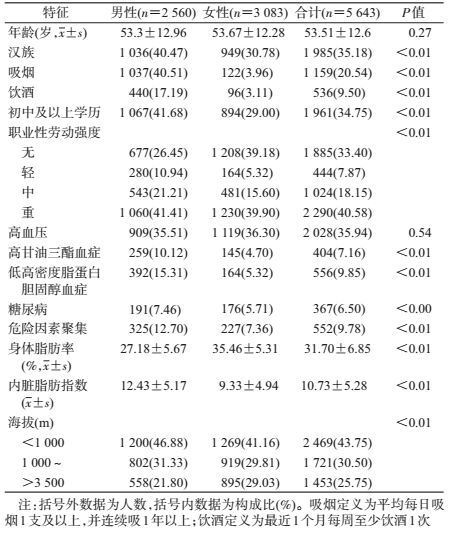
结果1.基本情况:男性2 560人,占45.36%。男性中VFI水平、汉族所占比例、吸烟率、饮酒率、职业劳动强度重的比例、初中及以上文化程度比例及危险因素聚集患病率均显著高于女性(P<0.01)。见表 1。
2. BFP、VFI人群中危险因素及其聚集的分布情况:BFP四分位不同组间,高血压、糖尿病、高甘油三酯血症、低高密度脂蛋白胆固醇血症和危险因素聚集率差异有统计学意义(P<0.05)。两两比较显示,按BFP四分位分组,第一组和第二组、第一组和第四组以及第二组和第三组间差异有统计学意义(P<0.008 3)。由BFP低到高四组的危险因素聚集患病率分别为7.60%、10.81%、8.80%和10.97%。见图 1。

|
| 注:运用四分位数法将体脂脂肪分为:第一组5.0%~27.0%,第二组:27.1%~31.7%,第三组31.8%~36.6%,第四组:36.7%~50.0% 图 1 不同身体脂肪率分组中各项危险因素及其聚集的患病率 |
VFI四分位不同组间,高血压、糖尿病、高TG血症、低HDL-C血症和危险因素聚集率差异有统计学意义(P<0.05)。两两比较显示,按VFI四分位分组,除第一组和第二组间无差异,其余各组间差异均有统计学意义(P<0.008 3)。由VFI低到高四组的危险因素聚集患病率分别为3.68%、5.11%、9.19%和18.60%。高血压、糖尿病、高TG血症、低HDL-C血症和危险因素聚集患病率均随着VFI升高呈上升趋势。见图 2。

|
| 注:运用四分位数法将内脏脂肪指数分为:第一组:1~6,第二组:7~9,第三组:10~13,第四组:14~30 图 2 不同内脏脂肪指数分组中各项危险因素及其聚集的患病率 |
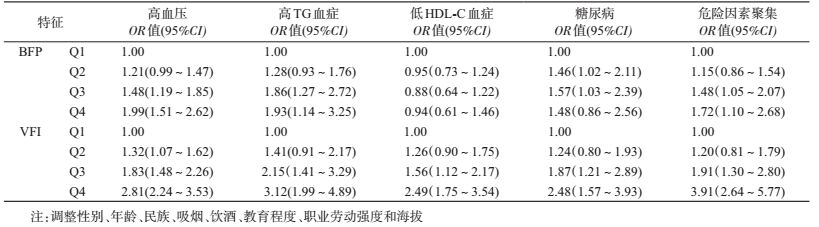
3.多因素分析BFP、VFI与危险因素聚集:以危险因素聚集为因变量,采用多因素logistic回归分析不同BFP、VFI水平对各项危险因素及其聚集的影响。BFP、VFI按照四分位数分组,调整性别、年龄、民族、吸烟、饮酒、教育程度、职业劳动强度和海拔,结果显示,随着BFP或VFI水平升高,BFP或VFI与危险因素聚集关联的OR值增大。以BFP为5.0%~27.0%组OR值为1,BFP为27.1%~31.7%组、31.8%~36.6%组和36.7%~50.0%组OR值(95%CI)分别为1.15(0.86~1.54)、1.48(1.05~2.07)和1.72(1.10~2.68);以VFI为1~6组OR值为1,VFI为7~9组、10~13组和14~30组OR值(95%CI)分别为1.20(0.81~1.79)、1.91(1.30~2.80)和3.91(2.64~5.77)。BFP≥31.6%和VFI≥10是心脏代谢性危险因素聚集的独立危险因素。见表 2。
4. BFP、VFI对各项危险因素及其聚集的预测价值:BFP、VFI预测危险因素聚集、糖尿病、高甘油三酯血症的ROC曲线下面积(95%CI)分别为0.55(0.53~0.56)和0.70(0.68~0.71),0.55(0.54~0.57)和0.63(0.62~0.65),0.52(0.51~0.54)和0.65(0.64~0.66),VFI对危险因素聚集、糖尿病和高甘油三酯血症预测的ROC曲线下面积均大于BFP(P<0.01)。见表 3。

肥胖与心血管疾病危险因素及其聚集密切相关[12-13],探索肥胖相关的有效筛查指标以预测心血管危险因素聚集在慢病防治中具有重要意义。本研究结果显示,BFP、VFI水平均与心脏代谢性危险因素聚集相关,VFI对危险因素聚集的预测价值较好。
我国新疆、西藏地区危险因素聚集患病率相对较高,男性12.70%,女性7.36%。其中男性高甘油三酯血症、低高密度脂蛋白胆固醇血症和糖尿病患病率均高于女性。国内一项研究显示,2项以上危险因素聚集(高血压、糖尿病、血脂异常)患病率男性(37.0%)显著高于女性(14.4%)[7],本研究与之一致。危险因素聚集患病率相对较高可能与新疆、西藏居民饮食多为肉类等高热量高脂低纤维食物以及气候寒冷及环境受限,人们缺少体育锻炼有关。既往研究报道,女性BFP更高[14]。本研究中女性BFP高于男性,但男性VFI显著高于女性。研究发现内脏型肥胖对心血管健康的影响更密切[15],这可能是男性危险因素聚集患病率高的原因之一。男性吸烟、饮酒率高于女性,女性健康意识较强等可部分解释危险因素的性别差异,提示当地居民应适当控制摄入高热量食物,增加体育运动。
既往研究发现,高BFP水平可增加心血管疾病的发病风险,且该效应独立于BMI的影响[6];VFI与MS及其各成分也密切相关,MS患病风险随VFI升高而增加[9, 16]。亚洲人BMI水平较低,但在相同的BMI水平中,其BFP水平较高[17]。本调查发现,BFP、VFI均与代谢性危险因素聚集相关,高血压、糖尿病、高甘油三酯血症、低高密度脂蛋白胆固醇血症和危险因素聚集患病率均随着VFI水平的升高而增加;调整混杂因素后,BFP和VFI水平升高仍与代谢性危险因素聚集的患病风险呈正相关。
本研究利用ROC曲线分析,提示BFP和VFI对高血压均有一定预测价值,与一项对我国35~64岁人群的研究结果一致[18]。研究显示,VFI对危险因素聚集的预测价值较高,且VFI对危险因素聚集、糖尿病、高甘油三酯血症的预测价值均优于BFP。Knowles等[19]的研究也发现VFI是MS及其组分较好的预测工具。国内一项研究也证明VFI在男女中均能较好预测MS[20]。相比于身体脂肪,内脏脂肪与危险因素聚集关系更为密切[21]。腰围虽为间接评价内脏脂肪的指标,但其并不能区分皮下脂肪和内脏脂肪的质量[22]。VFI比腰围能更加准确反映内脏脂肪含量[23],区分内脏脂肪和皮下脂肪。提示脂肪堆积和/或内脏脂肪堆积可能是心血管代谢异常和其他危险因素聚集的重要预测因素。
本研究基于大规模且具有代表性的抽样调查,但也存在一定局限性。研究为横断面调查,BFP、VFI与危险因素聚集的深层关系需要前瞻性研究进一步证实。本研究提示,VFI与心脏代谢性危险因素聚集关系紧密,VFI可作为一个简便筛查工具,对高血压、糖尿病、危险因素聚集等的高危人群筛查和家庭健康监测具有重要意义。对肥胖相关心血管代谢性疾病的预防,不仅要关注脂肪含量,脂肪分布亦不容忽视。高危人群应倡导健康生活方式,预防相关疾病的发生发展。
志谢: 感谢参与项目的所有专家及所有调查人员;协作组组成单位及主要调查人员:国家心血管病中心中国医学科学院阜外医院:王增武、张林峰、陈祚、王馨、邵澜、郭敏、田野、赵天明、范国辉、董莹、聂静雨、王佳丽、郑聪毅、贾秀云、朱曼璐、王文、陈伟伟、高润霖;卫生部北京医院:郭岩斐、孙铁英、王玉霞、柴迪、马雅立、仝亚琪;中国人民解放军总医院:陈韵岱、冯斌、朱庆磊、周珊珊、刘杰、王晶、杨丽娜、杨瑛、段鹏;新疆维吾尔自治区人民医院:李南方、周玲、张德莲、姚晓光、洪静、索菲亚、曹梅;中国疾病预防控制中心:吴静、石文惠、翟屹、何柳利益冲突: 无
| [1] | Ammar KA, Redfield MM, Mahoney DW, et al. Central obesity:association with left ventricular dysfunction and mortality in the community[J]. Am Heart J, 2008, 156(5): 975–981. DOI:10.1016/j.ahj.2008.06.018 |
| [2] | Dagenais GR, Yi Q, Mann JF, et al. Prognostic impact of body weight and abdominal obesity in women and men with cardiovascular disease[J]. Am Heart J, 2005, 149(1): 54–60. DOI:10.1016/j.ahj.2004.07.009 |
| [3] | Gordon-Larsen P, Wang HJ, Popkin BM. Overweight dynamics in Chinese children and adults[J]. Obes Rev, 2014, 15(1): 37–48. DOI:10.1111/obr.12121 |
| [4] | Yamashita K, Kondo T, Osugi S, et al. The significance of measuring body fat percentage determined by bioelectrical impedance analysis for detecting subjects with cardiovascular disease risk factors[J]. Circ J, 2012, 76(10): 2435–2442. DOI:10.1253/circj.CJ-12-0337 |
| [5] | Cho YG, Song HJ, Kim JM, et al. The estimation of cardiovascular risk factors by body mass index and body fat percentage in Korean male adults[J]. Metabolism, 2009, 58(6): 765–771. DOI:10.1016/j.metabol.2009.01.004 |
| [6] | Zeng Q, Dong SY, Sun XN, et al. Percent body fat is a better predictor of cardiovascular risk factors than body mass index[J]. Braz J Med Biol Res, 2012, 45(7): 591–600. DOI:10.1590/S0100-879X2012007500059 |
| [7] |
董剩勇, 王曼柳, 孙晓楠, 等.
体脂肪率评估心血管危险因素研究[J]. 中国全科医学, 2015, 18(36): 4416–4421.
Dong SY, Wang ML, Sun XN, et al. Body fat percentage in the evaluation of risk factors for cardiovascular risk factors[J]. Chin Genl Pract, 2015, 18(36): 4416–4421. DOI:10.3969/j.issn.1007-9572.2015.36.004 |
| [8] | Schuster J, Vogel P, Eckhardt C, et al. Applicability of the visceral adiposity index (VAI) in predicting components of metabolic syndrome in young adults[J]. Nutr Hosp, 2014, 30(4): 806–812. DOI:10.3305/nh.2014.30.4.7644 |
| [9] |
窦相峰, 白真真, 闫坤丽, 等.
女性内脏脂肪指数与代谢综合征的关系[J]. 中国循证心血管医学杂志, 2013, 5(1): 24–26.
Dou XF, Bai ZZ, Yan KL, et al. Relationship between visceral fat indexes and metabolic syndrome in women[J]. Chin J Evid Based Cardiovasc Med, 2013, 5(1): 24–26. DOI:10.3969/j.1674-4055.2013.01.009 |
| [10] | Hyun YJ, Kim OY, Jang Y, et al. Evaluation of metabolic syndrome risk in Korean premenopausal women:not waist circumference but visceral fat[J]. Circ J, 2008, 72(8): 1308–1315. DOI:10.1253/circj.72.1308 |
| [11] | Bosy-Westphal A, Later W, Hitze B, et al. Accuracy of bioelectrical impedance consumer devices for measurement of body composition in comparison to whole body magnetic resonance imaging and dual X-ray absorptiometry[J]. Obes Facts, 2008, 1(6): 319–324. DOI:10.1159/000176061 |
| [12] | Arnlöv J, Ingelsson E, Sundström J, et al. Impact of body mass index and the metabolic syndrome on the risk of cardiovascular disease and death in middle-aged men[J]. Circulation, 2010, 121(2): 230–236. DOI:10.1161/circulationaha.109.887521 |
| [13] | Yun JE, Won S, Sung J, et al. Impact of metabolic syndrome independent of insulin resistance on the development of cardiovascular disease[J]. Circ J, 2012, 76(10): 2443–2448. DOI:10.1253/circj.CJ-12-0125 |
| [14] | Lavie CJ, De Schutter A, Patel DA, et al. Body composition and survival in stable coronary heart disease:impact of lean mass index and body fat in the "obesity paradox"[J]. J Am Coll Cardiol, 2012, 60(15): 1374–1380. DOI:10.1016/j.jacc.2012.05.037 |
| [15] | Tong J, Boyko EJ, Utzschneider KM, et al. Intra-abdominal fat accumulation predicts the development of the metabolic syndrome in non-diabetic Japanese-Americans[J]. Diabetologia, 2007, 50(6): 1156–1160. DOI:10.1007/s00125-007-0651-y |
| [16] | Amato MC, Giordano C, Galia M, et al. Visceral adiposity index:a reliable indicator of visceral fat function associated with cardiometabolic risk[J]. Diabetes Care, 2010, 33(4): 920–922. DOI:10.2337/dc09-1825 |
| [17] | WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies[J]. Lancet, 2004, 363(9403): 157–163. DOI:10.1016/s0140-6736(03)15268-3 |
| [18] |
郝光, 王增武, 张林峰, 等.
不同肥胖测量指标对心脏代谢性疾病预测价值的比较[J]. 医学研究杂志, 2014, 43(12): 18–22.
Hao G, Wang ZW, Zhang LF, et al. Comparison of various anthropometric and body fat indices in identifying cardio metabolic disturbances in Chinese population[J]. J Med Res, 2014, 43(12): 18–22. |
| [19] | Knowles KM, Paiva LL, Sanchez SE, et al. Waist circumference, body mass index, and other measures of adiposity in predicting cardiovascular disease risk factors among peruvian adults[J]. Int J Hypertens, 2011, 2011: 931402. DOI:10.4061/2011/931402 |
| [20] |
张强, 陈晓平, 施迪, 等.
内脏脂肪指数与缺血性心血管病发病风险的关系[J]. 西部医学, 2016, 28(10): 1378–1381.
Zhang Q, Chen XP, Shi D, et al. Relationship between visceral adiposity index and risk of ischemic cardiovascular disease[J]. Med J West China, 2016, 28(10): 1378–1381. DOI:10.3969/j.issn.1672-3511.2016.10.010 |
| [21] | Matsushita Y, Nakagawa T, Yamamoto S, et al. Associations of visceral and subcutaneous fat areas with the prevalence of metabolic risk factor clustering in 6292 Japanese individuals:the Hitachi Health Study[J]. Diabetes Care, 2010, 33(9): 2117–2119. DOI:10.2337/dc10-0120 |
| [22] | Mathieu P, Pibarot P, Larose E, et al. Visceral obesity and the heart[J]. Int J Biochem Cell Biol, 2008, 40(5): 821–836. DOI:10.1016/j.biocel.2007.12.001 |
| [23] | Amato MC, Giordano C, Pitrone M, et al. Cut-off points of the visceral adiposity index (VAI) identifying a visceral adipose dysfunction associated with cardiometabolic risk in a Caucasian Sicilian population[J]. Lipids Health Dis, 2011, 10: 183. DOI:10.1186/1476-511x-10-183 |