 2017, Vol. 38
2017, Vol. 38文章信息
- 黄象艳, 石庆芬, 黄涛.
- Huang Xiangyan, Shi Qingfen, Huang Tao.
- 隐匿性乙型肝炎病毒感染研究进展
- Progress in research of occult hepatitis B virus infection
- 中华流行病学杂志, 2017, 38(5): 688-692
- Chinese Journal of Epidemiology, 2017, 38(5): 688-692
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2017.05.027
-
文章历史
收稿日期: 2016-12-05




2. 250021 济南市传染病医院检验科;
3. 250014 济南, 山东省疾病预防控制中心艾滋病防治所
2. Department of Laboratory Diagnostics, Jinan Infectious Disease Hospital, Jinan 250021, China;
3. Institute for AIDS Control and Prevention, Shandong Provincial Center for Disease Control and Prevention, Jinan 250014, China
HBV感染是发生肝脏疾病的主要原因之一,HBsAg通常被认为是HBV感染的主要血清学标志物。但不容忽视的是,有时商品化试剂盒不能检测到患者血清中的HBsAg,却可以在其肝脏或血液中检测到HBV的DNA,这就被称之为隐匿性HBV感染(occult hepatitis B virus infection,OBI)[1-2]。OBI患者的血清通常与大多数敏感的HBsAg检测试剂缺乏反应性,与HBsAg阳性的慢性乙型肝炎(乙肝)患者相比,往往呈现较低的病毒DNA水平。Wong等[3]研究了40例OBI患者和40例慢性乙肝患者肝内HBV复制状态,发现OBI患者的肝内总HBV的DNA低于慢性乙肝患者(P<0.000 1),这提示OBI患者往往具有低肝内HBV复制。有些OBI患者曾经有过慢性乙肝史,有些追溯不到既往HBV显性感染。
基于血清中抗-HBc和抗-HBs的检测结果,OBI可被分为血清学阳性和阴性两类。前者表现为抗-HBc阳性同时抗-HBs可为阳性也可为阴性;后者表现为抗-HBc和抗-HBs均为阴性[4]。多数OBI者携带有抗-HBc,但也存在除了HBV的DNA外检测不到任何血清学标志物的感染者。OBI是世界性的公共卫生问题之一,HBV的隐匿感染不仅可以造成临床诊断失误和肝脏损害的加剧[5],还会因为献血者中OBI造成血液污染而影响血液安全[6]。
1. OBI的发生机制:随着人们对OBI的认识和关注,有关其发生机制尚未完全阐明,但已经提出了许多免疫致病机制来解释导致其发生的原因。① 许多研究揭示了S基因突变与不同基因型OBI的相关性[7-9]。S基因突变引起OBI的机制有两点,一是HBsAg检测试剂盒中特异性抗体识别的靶位点一般在S抗原的主要疏水性区域(MHR),此区域的突变可导致抗原决定簇构象的改变或者抗原蛋白的修饰,从而导致检测抗体结合的失败[10]。尤其是MHR中“α”决定簇的突变,如G145R、Q129R和M133T,均可导致蛋白构象的改变。二是HBV基因组突变可以通过减少HBsAg的表达和分泌降低血清中HBsAg的产物量[11-12],因循环中HBsAg水平低于检测限而导致检测失败。② 血清中HBsAg和抗-HBs免疫复合物的形成可以隐藏HBsAg,导致无法检测到HBsAg的存在[2]。③ 如果同时感染了HCV或丁型肝炎病毒(HDV),由于病毒的干扰,HBV的复制会受到抑制,导致OBI的发生[13]。④ 有时患者本身的原因如免疫系统的原因也会造成HBV复制的下调,导致HBsAg检测的失败[14]。
S基因突变一般被认为是导致OBI的主要因素。研究发现前S基因(preS)和S基因的一些新突变位点,比如,preS1 nt 3 014~3 198缺失突变、preS1 nt 3 046~3 177缺失突变、s115-116 “INGTST”的插入突变等会减少HBsAg合成水平或降低抗体结合的能力从而导致OBI的发生[15]。但也有研究发现有些OBI标本中未发现S基因突变,提示在这些标本中,相比于S基因突变可能需要寻找其他更主要的导致OBI发生的因素[16]。有研究认为S蛋白突变可能不会在OBI发病机制中发挥主要作用[17]。总之,OBI的发生在不同个体中可能存在不同的机制,也可能在同一个体中存在多种因素共同作用导致OBI的发生,其发生机制还有待于进一步研究。
2.不同人群OBI发生率:OBI在不同国家和地区、不同人群中流行程度不同。除了在高危人群中的研究报道之外,目前在献血者、健康人群中研究报道OBI的也越来越多。在HBV流行度高的国家和地区,相关研究报道较多。
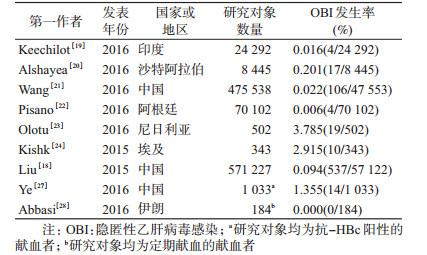
(1)献血者中OBI发生率:中国是HBV高流行地区,献血者中HBV流行率约为1.1%~3.1%[18]。持续疫苗接种计划、无偿献血制度的制定发展和血液筛检技术的进步已经使献血者中HBV感染情况明显好转,但OBI的存在却威胁着输血安全,多个国家和地区在献血者中发现OBI[19-24]。Liu等[18]利用Meta分析发现在中国571 227名献血者中OBI的发生率约为0.094%。OBI在中国无偿献血人群中的比率高于阿根廷、印度、伊朗等国,但低于非洲国家(表 1)。在HBV非流行区,献血者OBI发生率相对较低,如在苏格兰1989-2011年7 925 259名献血者中仅检测到5名OBI[25]。Stramer等[26]报道在美国3 700 000名献血者中,OBI发生率仅为0.000 2%。Ye等[27]研究了抗-HBc阳性的健康献血者(表 1),其中发现14例OBI,在抗-HBc阳性的健康人群中存在相对高的OBI发生率。值得注意的是,这14例OBI使用血站常规核酸扩增检测技术(NAT)检测结果为阴性。所以在中国抗-HBc阳性率较高的HBV高流行区,需要敏感度更高的NAT来提高血液安全。定期无偿献血者可能会减少OBI的潜在危险,Abbasi等[28]在184名定期献血者中没有发现OBI(表 1),这可能与定期血液检测排除转为显性感染的OBI有关。
(2)乙肝疫苗免疫人群中OBI发生率:我国新生儿乙肝疫苗接种计划自1992年在全国实施,有效降低了HBV感染率。但是接种乙肝疫苗并不能完全杜绝HBV感染,Ni等[29]报道中国台湾地区1984年7月开始接种乙肝疫苗,HBsAg血清学阳性率由未接种疫苗时的6.7%降至0.5%;接种乙肝疫苗后HBsAg仍为阳性的感染者中77%的母亲为HBV感染者。这项研究对4 605名接种过疫苗的健康人进行研究,显示OBI约为0.13%(表 2)。其他国家和地区的报道也显示尽管接受过乙肝疫苗的接种,这些人群中还是存在OBI[16, 30-31]。部分HBsAg阳性母亲所生婴儿免疫阻断后虽然HBsAg阴性且符合目前HBV母婴阻断成功的标准,但其血清中HBV的DNA检测阳性,提示这些婴儿免疫阻断后存在OBI[32]。国内一项研究显示,母亲如果是HBsAg阳性,即便是新生儿接受了针对HBV的主动和被动免疫,在7月龄时还是可检测到OBI,发生率高达20%[33](表 2)。该研究发现新生儿体内HBV与母亲HBV具有同源性,但没有发现G145R突变,随着年龄的增长,监测到3岁时,31例都在某个时间点发生了HBV-DNA消失,但有6例出现了反弹。鉴于乙肝疫苗免疫产生的抗-S抗原在HBV高流行区不能完全预防OBI的发生,开发针对S抗原以外更多抗原位点的疫苗可改善这种状况[31]。另外,不同个体对乙肝疫苗的反应水平不同,疫苗无反应性相关因素之一可能是当前或过去的HBV感染的存在。无论是HBV显性感染还是OBI都可导致乙肝疫苗的无反应性或低反应性的病例出现。

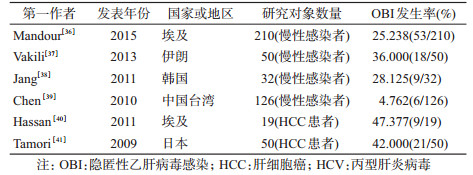
(3)HCV感染者中OBI发生率:OBI在HCV阳性者中的发生率显著高于HCV阴性者[34]。在慢性丙型肝炎(丙肝)患者中,近1/3病例中发现了OBI,可能与HCV干扰HBV复制而导致OBI发生有关,HCV核心蛋白可通过与HBX蛋白和聚合酶之间的作用抑制HBV基因表达和复制[13]。OBI会加重慢性丙肝患者的肝损伤和肝细胞癌(HCC)的进展[35]。不同研究报道慢性HCV感染者中OBI的发生率不同(表 3),3项研究表明OBI发生率均大于25%[36-38],在另一项研究中OBI发生率相对较低[39],但在HCV感染的HCC患者中,OBI发生率都在40%以上[40-41],明显高于慢性HCV感染者。一般认为,OBI与HCV感染的HCC发生有相关性,OBI在HCV感染的HCC患者中的比例明显高于未感染HCV的HCC患者[2]。
(4)HIV感染者中OBI发生率:多数HIV感染者因感染途径的原因,会增加HBV感染的概率,而其中发生OBI的比率也有不同国家的研究报道。智利的研究对象中未检测到OBI[42],但是其他研究都在HIV感染者中检测到OBI[43-44],2项研究报道OBI发生率为4%左右,另外4项研究中OBI发生率较高,约15%~48%[10, 45-47](表 4)。健康成年人接种乙肝疫苗具有良好的免疫效果,HIV感染者、注射吸毒者、慢性肝病患者等高危人群接种乙肝疫苗的安全性已被证实,但其免疫效果低于健康成年人[48],这可能是HIV感染者中OBI发生率相对较高的原因之一。

(5)其他人群中OBI发生率:免疫力受影响的人群或易感人群,如白血病患者、肿瘤患者、肺结核患者、静脉吸毒者、血液透析患者等,都有关于OBI发生率的研究报道。注射吸毒者中OBI发生率较高[49],肺结核患者中OBI发生率相对较低[50],肿瘤患者中OBI发生率相对较高[5, 51-52],血液透析患者中OBI发生率在3%~8%[53-54],白血病患者中OBI发生率明显高于骨折的对照组(10.5%比2.9%,P<0.001)[51]。Baghbanian等[52]研究发现OBI在血液肿瘤患者中的发生率比在实体瘤患者中稍高(4.8%比4.3%)。见表 5。

3. OBI传播:由于OBI患者常规HBsAg筛查呈阴性而容易被忽视,其是否存在HBV传播可能性更应该引起注意。多数OBI患者血液中病毒载量很低,OBI病原体可以传播给免疫抑制患者,但是通过输血、母婴传播、医源性途径等能否将OBI病原体传播给免疫力正常的受血者、新生儿或患者尚无定论,有待进一步研究。
OBI献血者能否将HBV传播给受血者一直是关注的焦点。Bouike等[55]研究表明,虽然OBI献血者中HBV的DNA水平很低,但是HBV还是通过输血传染给了受血者。有研究表明带有抗-HBs的OBI患者血液可能不具有传染性,而仅含有抗-HBc或除DNA外没有其他血清学标志物的OBI患者血液具有传染性[56]。Lieshout-Krikke等[57]对接受OBI献血者血液的受血者进行回顾性研究,传播概率为5%。在HBV高流行区献血者中OBI发生率虽然高,但中国香港和台湾地区的两项研究表明接受OBI献血者血液成分的受血者虽然存在个别输血途径感染,但传播的可能性极小[58-59]。OBI献血者的血制品虽然存在通过血液传播HBV的危险性,但这种危险性与抗-HBs存在与否以及输入的血浆量有关。
OBI是否可以通过母婴传播使婴儿发生HBV感染,尚无研究报道。目前的研究只是显示个别HBsAg阳性母亲可以导致接受过免疫阻断的新生儿发生OBI[32-33],但缺乏OBI母亲孕产过程中母婴垂直传播的研究报道。
一项关于OBI患者和其子的研究报道,OBI可能通过紧密接触传播HBV。尽管OBI患者的孩子进行了乙肝疫苗注射,但还是发生了HBV感染,经过HBV序列比对发现父亲体内的HBV是其子HBV感染的来源,表明OBI可能通过密切接触传播,并表现为显性感染[60]。
通过输血、器官移植和血液透析传播OBI的重要性已被广泛认可,OBI传播可能性与被感染者接触的病毒含量及其免疫状态有关。由表 3~5可见因未检出HBsAg而认定为无HBV感染的OBI患者,在就诊过程中是有可能通过医源性途径传播HBV的。因此,提高OBI的检出率和寻找预防OBI患者传播HBV的方法应引起关注。
综上所述,OBI影响临床诊断和血液安全,与肝损伤严重程度有一定相关性。OBI不仅存在于HCV、HIV感染者及肿瘤、透析患者等人群中,也在健康人群中存在并有传播的可能性。因此,OBI需进一步引起大家的关注,研究更加敏感的HBV检测方法以减少HBV的漏检,研发HBV新疫苗以减少OBI的发生,都将对预防OBI起到积极作用。
利益冲突: 无
| [1] | Raimondo G, Allain JP, Brunetto MR, et al. Statements from the Taormina expert meeting on occult hepatitis B virus infection[J]. J Hepatol, 2008, 49(4): 652–657. DOI:10.1016/j.jhep.2008.07.014 |
| [2] | Huang X, Hollinger FB. Occult hepatitis B virus infection and hepatocellular carcinoma:a systematic review[J]. J Viral Hepat, 2014, 21(3): 153–162. DOI:10.1111/jvh.12222 |
| [3] | Wong DK, Fung J, Lee CK, et al. Intrahepatic hepatitis B virus replication and liver histology in subjects with occult hepatitis B infection[J]. Clin Microbiol Infect, 2016, 22(3): 290.e1–3. DOI:10.1016/j.cmi.2015.10.036 |
| [4] | Fierro NA, Roman S, Realpe M, et al. Multiple cytokine expression profiles reveal immune-based differences in occult hepatitis B genotype H-infected Mexican Nahua patients[J]. Mem Inst Oswaldo Cruz, 2011, 106(8): 1007–1013. DOI:10.1590/S0074-02762011000800018 |
| [5] | Coppola N, Onorato L, Iodice V, et al. Occult HBV infection in HCC and cirrhotic tissue of HBsAg-negative patients:a virological and clinical study[J]. Oncotarget, 2016, 7(38): 62706–62714. DOI:10.18632/oncotarget.10909 |
| [6] | Zaaijer HL, Torres P, Ontañón A, et al. Multiple surface antigen mutations in five blood donors with occult hepatitis B virus infection[J]. J Med Virol, 2008, 80(8): 1344–1349. DOI:10.1002/jmv.21233 |
| [7] | El Chaar M, Candotti D, Crowther RA, et al. Impact of hepatitis B virus surface protein mutations on the diagnosis of occult hepatitis B virus infection[J]. Hepatology, 2010, 52(5): 1600–1610. DOI:10.1002/hep.23886 |
| [8] | Huang X, Qin Y, Li W, et al. Molecular analysis of the hepatitis B virus presurface and surface gene in patients from eastern China with occult hepatitis B[J]. J Med Virol, 2013, 85(6): 979–986. DOI:10.1002/jmv.23556 |
| [9] | Svicher V, Cento V, Bernassola M, et al. Novel HBsAg markers tightly correlate with occult HBV infection and strongly affect HBsAg detection[J]. Antiviral Res, 2012, 93(1): 86–93. DOI:10.1016/j.antiviral.2011.10.022 |
| [10] | Sadeghi A, Shirvani-Dastgerdi E, Tacke F, et al. HBsAg mutations related to occult hepatitis B virus infection in HIV-positive patients result in a reduced secretion and conformational changes of HBsAg[J]. J Med Virol, 2017, 89(2): 246–256. DOI:10.1002/jmv.24623 |
| [11] | Martin CM, Welge JA, Rouster SD, et al. Mutations associated with occult hepatitis B virus infection result in decreased surface antigen expression in vitro[J]. J Viral Hepat, 2012, 19(10): 716–723. DOI:10.1111/j.1365-2893.2012.01595.x |
| [12] | Zhu HL, Li X, Li J, et al. Genetic variation of occult hepatitis B virus infection[J]. World J Gastroenterol, 2016, 22(13): 3531–3546. DOI:10.3748/wjg.v22.i13.3531 |
| [13] | Chen SY, Kao CF, Chen CM, et al. Mechanisms for inhibition of hepatitis B virus gene expression and replication by hepatitis C virus core protein[J]. J Biol Chem, 2003, 278(1): 591–607. DOI:10.1074/jbc.M204241200 |
| [14] | Pollicino T, Raffa G, Costantino L, et al. Molecular and functional analysis of occult hepatitis B virus isolates from patients with hepatocellular carcinoma[J]. Hepatology, 2007, 45(2): 277–285. DOI:10.1002/hep.21529 |
| [15] | Chen JH, Liu Y, Zhao J, et al. Characterization of novel hepatitis B virus PreS/S-Gene mutations in a patient with occult hepatitis B virus infection[J]. PLoS One, 2016, 11(5): e0155654. DOI:10.1371/journal.pone.0155654 |
| [16] | Borzooy Z, Jazayeri SM, Mirshafiey A, et al. Identification of occult hepatitis B virus (HBV) infection and viral antigens in healthcare workers who presented low to moderate levels of anti-HBs after HBV vaccination[J]. Germs, 2015, 5(4): 134–140. DOI:10.11599/germs.2015.1081 |
| [17] | Zhang ZH, Zhang L, Dai Y, et al. Occult hepatitis B virus infection:influence of S protein variants[J]. Virol J, 2016, 13: 10. DOI:10.1186/s12985-016-0464-z |
| [18] | Liu GC, Sui GY, Liu GY, et al. A Bayesian Meta-analysis on prevalence of hepatitis B virus infection among Chinese volunteer blood donors[J]. PLoS One, 2013, 8(11): e79203. DOI:10.1371/journal.pone.0079203 |
| [19] | Keechilot CS, Shenoy V, Kumar A, et al. Detection of occult hepatitis B and window period infection among blood donors by individual donation nucleic acid testing in a tertiary care center in South India[J]. Pathog Glob Health, 2016, 110(7/8): 287–291. DOI:10.1080/20477724.2016.1248171 |
| [20] | Alshayea AI, Eid GE, El-Hazmi MM, et al. Prevalence and characterization of occult hepatitis B infection among blood donors in central Saudi Arabia[J]. Saudi Med J, 2016, 37(10): 1114–1119. DOI:10.15537/smj.2016.10.14708 |
| [21] | Wang Z, Zeng JF, Li TT, et al. Prevalence of hepatitis B surface antigen (HBsAg) in a blood donor population born prior to and after implementation of universal HBV vaccination in Shenzhen, China[J]. BMC Infect Dis, 2016, 16: 498. DOI:10.1186/s12879-016-1834-2 |
| [22] | Pisano MB, Blanco S, Carrizo H, et al. Hepatitis B virus infection in blood donors in Argentina:prevalence of infection, genotype distribution and frequency of occult HBV infection[J]. Arch Virol, 2016, 161(10): 2813–2817. DOI:10.1007/s00705-016-2960-2 |
| [23] | Olotu AA, Oyelese AO, Salawu L, et al. Occult hepatitis B virus infection in previously screened, blood donors in Ile-Ife, Nigeria:implications for blood transfusion and stem cell transplantation[J]. Virol J, 2016, 13: 76. DOI:10.1186/s12985-016-0533-3 |
| [24] | Kishk R, Nemr N, Elkady A, et al. Hepatitis B surface gene variants isolated from blood donors with overt and occult HBV infection in north eastern Egypt[J]. Virol J, 2015, 12: 153. DOI:10.1186/s12985-015-0389-y |
| [25] | Larralde O, Dow B, Jarvis L, et al. Hepatitis B escape mutants in Scottish blood donors[J]. Med Microbiol Immunol, 2013, 202(3): 207–214. DOI:10.1007/s00430-012-0283-9 |
| [26] | Stramer SL, Wend U, Candotti D, et al. Nucleic acid testing to detect HBV infection in blood donors[J]. N Engl J Med, 2011, 364(3): 236–247. DOI:10.1056/NEJMoa1007644 |
| [27] | Ye XL, Li T, Xu XX, et al. Characterisation and follow-up study of occult hepatitis B virus infection in anti-HBc-positive qualified blood donors in southern China[J]. Blood Transfus, 2016, 15(1): 6–12. DOI:10.2450/2016.0268-15 |
| [28] | Abbasi S, Makvandi M, Karimi G, et al. The Prevalence of SEN Virus and Occult Hepatitis B (OBI) Virus Infection Among Blood Donors in Ahvaz City[J]. Jundishapur J Microbiol, 2016, 9(7): e37329. DOI:10.5812/jjm.37329 |
| [29] | Ni YH, Chang MH, Jan CF, et al. Continuing decrease in hepatitis B virus infection 30 years after initiation of infant vaccination program in Taiwan[J]. Clin Gastroenterol Hepatol, 2016, 14(9): 1324–1330. DOI:10.1016/j.cgh.2016.04.030 |
| [30] | Darmawan E, Turyadi, El-Khobar KE, et al. Seroepidemiology and occult hepatitis B virus infection in young adults in Banjarmasin, Indonesia[J]. J Med Virol, 2015, 87(2): 199–207. DOI:10.1002/jmv.24045 |
| [31] | Utsumi T, Yano Y, Lusida MI, et al. Serologic and molecular characteristics of hepatitis B virus among school children in East Java, Indonesia[J]. Am J Trop Med Hyg, 2010, 83(1): 189–193. DOI:10.4269/ajtmh.2010.09-0589 |
| [32] |
刘亚琳, 卢颖, 李杰.
乙型肝炎疫苗阻断母婴传播的新挑战:隐匿性感染[J]. 中华肝脏病杂志, 2016, 24(2): 157–160.
Liu YL, Lu Y, Li J. Occult hepatitis B virus infection:a new challenge for hepatitis B vaccine to block mother-to-child transmission[J]. Chin J Hepatol, 2016, 24(2): 157–160. DOI:10.3760/cma.j.issn.1007-3418.2016.02.019 |
| [33] | Lu Y, Liu YL, Nie JJ, et al. Occult HBV infection in immunized neonates born to HBsAg-positive mothers:a prospective and follow-up study[J]. PLoS One, 2016, 11(11): e0166317. DOI:10.1371/journal.pone.0166317 |
| [34] | Branco F, Mattos AA, Coral GP, et al. Occult hepatitis B virus infection in patients with chronic liver disease due to hepatitis C virus and hepatocellular carcinoma in Brazil[J]. Arq Gastroenterol, 2007, 44(1): 58–63. DOI:10.1590/S0004-28032007000100013 |
| [35] | Coppola N, Onorato L, Pisaturo M, et al. Role of occult hepatitis B virus infection in chronic hepatitis C[J]. World J Gastroenterol, 2015, 21(42): 11931–11940. DOI:10.3748/wjg.v21.i42.11931 |
| [36] | Mandour M, Nemr N, Shehata A, et al. Occult HBV infection status among chronic hepatitis C and hemodialysis patients in Northeastern Egypt:regional and national overview[J]. Rev Soc Bras Med Trop, 2015, 48(3): 258–264. DOI:10.1590/0037-8682-0037-2015 |
| [37] | Vakili Ghartavol Z, Alavian SM, Amini S, et al. Prevalence of occult hepatitis B virus in plasma and peripheral blood mononuclear cell compartments of patients with chronic hepatitis C infection in tehran-iran[J]. Hepat Mon, 2013, 13(5): e10134. DOI:10.5812/hepatmon.10134 |
| [38] | Jang JY, Jeong SW, Cheon SR, et al. Clinical significance of occult hepatitis B virus infection in chronic hepatitis C patients[J]. Korean J Hepatol, 2011, 17(3): 206–212. DOI:10.3350/kjhep.2011.17.3.206 |
| [39] | Chen LW, Chien RN, Yen CL, et al. Therapeutic effects of pegylated interferon plus ribavirin in chronic hepatitis C patients with occult hepatitis B virus dual infection[J]. J Gastroenterol Hepatol, 2010, 25(2): 259–263. DOI:10.1111/j.1440-1746.2009.06006.x |
| [40] | Hassan ZK, Hafez MM, Mansor TM, et al. Occult HBV infection among Egyptian hepatocellular carcinoma patients[J]. Virol J, 2011, 8: 90. DOI:10.1186/1743-422X-8-90 |
| [41] | Tamori A, Hayashi T, Shinzaki M, et al. Frequent detection of hepatitis B virus DNA in hepatocellular carcinoma of patients with sustained virologic response for hepatitis C virus[J]. J Med Virol, 2009, 81(6): 1009–1014. DOI:10.1002/jmv.21488 |
| [42] | Vargas JI, Jensen D, Sarmiento V, et al. Presence of anti-HBc is associated to high rates of HBV resolved infection and low threshold for Occult HBV Infection in HIV patients with negative HBsAg in Chile[J]. J Med Virol, 2016, 88(4): 639–646. DOI:10.1002/jmv.24384 |
| [43] | Oliveira MP, Lemes PS, Matos MA, et al. Overt and occult hepatitis B virus infection among treatment-naïve HIV-infected patients in Brazil[J]. J Med Virol, 2016, 88(7): 1222–1229. DOI:10.1002/jmv.24462 |
| [44] | Chadwick D, Doyle T, Ellis S, et al. Occult hepatitis B virus coinfection in HIV-positive African migrants to the UK:a point prevalence study[J]. HIV Med, 2014, 15(3): 189–192. DOI:10.1111/hiv.12093 |
| [45] | Alvarez-Muñoz MT, Maldonado-Rodriguez A, Rojas-Montes O, et al. Occult hepatitis B virus infection among Mexican human immunodeficiency virus-1-infected patients[J]. World J Gastroenterol, 2014, 20(37): 13530–13537. DOI:10.3748/wjg.v20.i37.13530 |
| [46] | Coffin CS, Mulrooney-Cousins PM, Osiowy C, et al. Virological characteristics of occult hepatitis B virus in a North American cohort of human immunodeficiency virus type 1-positive patients on dual active anti-HBV/HIV therapy[J]. J Clin Virol, 2014, 60(4): 347–353. DOI:10.1016/j.jcv.2014.04.021 |
| [47] | Bell TG, Makondo E, Martinson NA, et al. Hepatitis B virus infection in human immunodeficiency virus infected southern African adults:occult or overt-that is the question[J]. PLoS One, 2012, 7(10): e45750. DOI:10.1371/journal.pone.0045750 |
| [48] |
徐爱强, 张丽.
中国成年人乙型肝炎疫苗免疫策略的循证与思考[J]. 中华预防医学杂志, 2016, 50(6): 473–477.
Xu AQ, Zhang L. Immunization strategy of hepatitis B vaccine among adults in China:evidence based-medicine and consideration[J]. Chin J Prev Med, 2016, 50(6): 473–477. DOI:10.3760/cma.j.issn.0253-9624.2016.06.001 |
| [49] | Asli M, Kandelouei T, Rahimyan K, et al. Characterization of occult hepatitis B infection among injecting drug users in Tehran, Iran[J]. Hepat Mon, 2016, 16(3): e34763. DOI:10.5812/hepatmon.34763 |
| [50] | Iglecias LM, Puga MA, Pompílio MA, et al. Epidemiological study of hepatitis B virus among prisoners with active tuberculosis in Central Brazil[J]. Int J Tuberc Lung Dis, 2016, 20(11): 1509–1515. DOI:10.5588/ijtld.15.0743 |
| [51] | Zhang ZH, Zhang Y, Xu N, et al. High risk of occult hepatitis B virus infection in leukemia patients from China[J]. Arch Virol, 2016, 162(2): 349–357. DOI:10.1007/s00705-016-3111-5 |
| [52] | Baghbanian M, Halvani M, Roghani HS, et al. Prevalence of occult hepatitis B infection in iranian cancer patients before chemotherapy treatment[J]. Arq Gastroenterol, 2016, 53(3): 175–179. DOI:10.1590/S0004-28032016000300010 |
| [53] | Esmail MA, Mahdi WK, Khairy RM, et al. Genotyping of occult hepatitis B virus infection in Egyptian hemodialysis patients without hepatitis C virus infection[J]. J Infect Public Health, 2016, 9(4): 452–457. DOI:10.1016/j.jiph.2015.11.018 |
| [54] | Rastegarvand N, Makvandi M, Samarbafzadeh A, et al. Molecular characterization of Pre-Core/Core and S region of hepatitis B virus in hemodialysis patients with occult hepatitis B infection[J]. Jundishapur J Microbiol, 2015, 8(10): e23686. DOI:10.5812/jjm.23686 |
| [55] | Bouike Y, Imoto S, Mabuchi O, et al. Infectivity of HBV DNA positive donations identified in look-back studies in Hyogo-Prefecture, Japan[J]. Transfus Med, 2011, 21(2): 107–115. DOI:10.1111/j.1365-3148.2010.01057.x |
| [56] | Said ZNA. An overview of occult hepatitis B virus infection[J]. World J Gastroenterol, 2011, 17(15): 1927–1938. DOI:10.3748/wjg.v17.i15.1927 |
| [57] | Lieshout-Krikke RW, van Kraaij MG, Danovic F, et al. Rare transmission of hepatitis B virus by Dutch donors with occult infection[J]. Transfusion, 2016, 56(3): 691–698. DOI:10.1111/trf.13401 |
| [58] | Yuen MF, Wong DK, Lee CK, et al. Transmissibility of hepatitis B virus (HBV) infection through blood transfusion from blood donors with occult HBV infection[J]. Clin Infect Dis, 2011, 52(5): 624–632. DOI:10.1093/cid/ciq247 |
| [59] | Su TH, Chen PJ, Chen TC, et al. The clinical significance of occult hepatitis B transfusion in Taiwan-a look-back study[J]. Transfus Med, 2011, 21(1): 33–41. DOI:10.1111/j.1365-3148.2010.01036.x |
| [60] | Hu LP, Liu DP, Chen QY, et al. Occult HBV infection may be transmitted through close contact and manifest as an overt infection[J]. PLoS One, 2015, 10(10): e0138552. DOI:10.1371/journal.pone.0138552 |