 2017, Vol. 38
2017, Vol. 38文章信息
- 吴昕, 赵骏, 崔雪莲, 李晴, 陶华, 潘秦镜, 张询, 陈汶, 李艳萍, 李荣成, 吴婷, 黎明强.
- Wu Xin, Zhao Jun, Cui Xuelian, Li Qing, Tao Hua, Pan Qinjing, Zhang Xun, Chen Wen, Li Yanping, Li Rongcheng, Wu Ting, Li Mingqiang.
- 广西壮族自治区柳州市18~45岁社区女性人乳头瘤病毒感染及型别分布的横断面调查
- Prevalence of type-specific human papillomavirus infection among 18-45 year-old women from the general population in Liuzhou, Guangxi Zhuang Autonomous Region: a cross-sectional study
- 中华流行病学杂志, 2017, 38(4): 467-471
- Chinese journal of Epidemiology, 2017, 38(4): 467-471
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2017.04.011
-
文章历史
收稿日期: 2016-08-23




2. 361100 厦门大学公共卫生学院分子疫苗学和分子诊断学国家重点实验室, 国家传染病诊断试剂与疫苗工程技术研究中心;
3. 518028 深圳市妇幼保健院妇科;
4. 545500 广西壮族自治区柳州市妇幼保健院妇科;
5. 100021 北京, 国家癌症中心/中国医学科学院北京协和医学院肿瘤医院细胞室;
6. 100021 北京, 国家癌症中心/中国医学科学院北京协和医学院肿瘤医院病理科;
7. 100021 北京, 国家癌症中心/中国医学科学院北京协和医学院肿瘤医院流行病室;
8. 530023 南宁, 广西壮族自治区疾病预防控制中心临床试验中心;
9. 545000 广西壮族自治区柳州市疾病预防控制中心
2. State Key Laboratory of Molecular Vaccinology and Molecular Diagnostics, National Institute of Diagnostics and Vaccine Development in Infectious Diseases, School of Public Health, Xiamen University, Xiamen 361100, China;
3. Department of Gynecology and Obstetricsbirth, Shenzhen Maternity and Child Healthcare Hospital, Shenzhen 518028, China;
4. Department of Gynecology, Liuzhou Maternity and Child Healthcare Hospital, Liuzhou 545500, China;
5. Department of Cytology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing 100021, China;
6. Department of Pathology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing 100021, China;
7. Department of Epidemiology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing 100021, China;
8. Guangxi Autonomous Region Center for Disease Control and Prevention, Nanning 530023, China;
9. Liuzhou City Center for Disease Control and Prevention, Guangxi Zhuang Autonomous Region, Liuzhou 545000, China
全球每年约有53万宫颈癌新发病例,死亡27万[1],2015年我国新增宫颈癌病例约9.9万,死亡3.1万[2]。大部分宫颈癌发生与HPV感染有关[3-5],HPV感染主要通过性接触传播[6],以宫颈涂片为主的早期筛查是现今国内防控宫颈癌的主要方式。目前全球已有3种预防性HPV疫苗上市,分别是HPV 16/18二价疫苗(Cervarix®,英国GSK公司)、HPV 6/11/16/18四价疫苗(Gardasil®,德国Merck公司)以及HPV 6/11/16/18/31/33/45/52/58九价疫苗(Gardasil®9,德国Merck公司)。发达国家数据显示,青春期前的女性接种HPV疫苗最具成本效益[7]。GSK的二价疫苗Cervarix®于2016年7月在中国获得批准,除此之外,尚有多家单位正在进行HPV疫苗研发。本研究通过对广西壮族自治区柳州市18~45岁女性开展横断面调查获得育龄女性HPV感染特征及型别分布数据,为HPV疫苗研发、推广及免疫策略制定提供科学依据。
对象与方法1.研究对象:2013年3-7月在柳州市进行了以社区人群为基础的横断面研究。本研究预计人群HPV感染率(p)为15%[8-9],容许误差为0.1 p,α=0.05,估计调查样本量至少为2 260人。研究现场在社区通过广告、报纸、海报等方式招募了2 493名女性志愿者。研究对象纳入标准:① 18~45岁;② 有性生活史;③ 宫颈完整;④ 未接种过HPV疫苗。主要排除标准为48 h内同房或阴道冲洗。研究者筛选后,最终入组2 300人。本研究获得柳州市CDC伦理审查委员会批准,所有研究对象均在自愿的前提下签署知情同意书。
2.细胞学标本采集及诊断:研究对象由妇科医师按照美国Hologic公司ThinPrep® Pap法采样要求采集宫颈转换区及宫颈口的脱落细胞,并对每份标本进行液基细胞学诊断和HPV DNA检测。
液基细胞学诊断结果由细胞学专家采用Bethesda系统(TBS 2001)分类判读,包括不满意、未见上皮内病变细胞和恶性细胞(NILM)、意义不明确的非典型上皮细胞(ASC-US)、低度鳞状上皮内病变(LSIL)、非典型鳞状细胞不除外高度病变(ASC-H)、高度鳞状上皮内病变(HSIL)、非典型腺细胞(AGC)、宫颈内膜原位腺癌(AIS)。对诊断为ASC-US的标本进一步进行HC2(德国Qiagen公司)检测,根据临床规范对液基细胞学诊断异常(ASU-CS及以上)或HC2检测阳性的女性转诊阴道镜检查。
3.标本HPV DNA检测分型:采用HPV DNA酶免疫分析方法(荷兰Labo Biomedical公司)对宫颈脱落细胞标本进行HPV的定性检测[10]。该检测方法以SPF10作为引物,扩增HPV DNA,并通过标记的特异性DNA探针杂交进行检测。对DEIA检测阳性的标本采用反向杂交线型探针检测技术(荷兰Labo Biomedical公司)进行HPV分型检测。该方法可检测13种高危型别(HPV 16、18、31、33、35、39、45、51、52、56、58、59和68型)和12种低危型别(HPV 6、11、34、40、42、43、44、53、54、66、70和74型)[11]。
4.组织学标本采集和诊断:根据临床操作规范确定是否进行活检。由病理学专家根据WHO女性生殖器官肿瘤分类(2003)对活检采集的组织学标本进行病理诊断及结果报告。诊断结果包括慢性炎(阴性)、宫颈上皮内瘤变1~3级(CIN1~3)对组织学标本同样进行HPV DNA分型检测。
5.统计学分析:使用SAS 9.2软件对数据进行统计学分析。统计检验均使用α=0.05的双侧检验,率使用双侧95%CI。计量资料采用x±s描述,计数资料采用例数和率描述。均数比较采用t检验或秩和检验(如不满足t检验条件),率的比较采用χ2检验或Fisher精确概率法(如不满足χ2检验条件)。各年龄组HPV感染率比较采用Cochran-Armitage趋势性χ2检验。
结果1.入组情况:共入组2 300人,平均年龄(29.6±7.2)岁。其中2 103人(91.4%)液基细胞学诊断结果正常(NILM)或为ASC-US/HC2阴性,其余197人(8.6%)符合阴道镜转诊标准且均完成阴道镜检查,其中111人采集了组织学标本。
2. HPV DNA感染率及型别:在2 300份宫颈脱落细胞标本中,检测到任一型别HPV DNA阳性者522份,感染率为22.7%(95%CI:21.0%~24.4%),其中高危型和低危型HPV感染率分别为17.3%(95%CI:16.0%~19.1%)和8.2%(95%CI:7.1%~9.3%)。高危型HPV感染率前5位为HPV 52、16、51、58和39(图 1)。HPV DNA阳性人群中感染HPV 16/18二价、HPV 6/11/16/18四价和HPV 6/11/16/18/31/33/45/52/58九价HPV疫苗相关型别的比例分别为15.9%、18.6%和58.4%。

|
| 图 1 高危型HPV在广西壮族自治区柳州市18~45岁女性人群中的分布 |
在522名任一HPV型别阳性女性中,133人(25.5%)为多重感染,其中以双重感染最为常见,占77.4%。多重感染组合以高危型和高危型混合感染为主,共63例,占47.4%,其次为高危型和低危型混合感染,共61例,占45.9%,低危型和低危型混合感染仅9例,占6.8%。
3. HPV DNA感染及CIN2+病变年龄分布:按照任一型别、高危型别HPV感染进行分类后可见感染率均随研究对象的年龄变化呈双峰分布(图 2)。如高危型HPV感染率在18~25岁最高,为20.5%(95%CI:17.9%~23.1%),31~35岁降至14.0%(95%CI:10.2%~18.6%),后随年龄增长缓慢升高,41~45岁时达15.3%(95%CI:11.1%~20.2%)。任一型别、高危型别、低危型别HPV感染率随年龄变化趋势经检验差异有统计学意义(Z=2.59,P<0.05;Z=2.79,P<0.05;Z=2.30,P<0.05)。

|
| 图 2 广西壮族自治区柳州市18~45岁女性各年龄组HPV感染情况 |
按不同价态HPV疫苗所包含HPV型别感染特点,可以发现仅九价苗组型别感染率随年龄变化呈双峰分布(图 3):18~25岁感染率最高,为14.6%(95%CI:12.4%~17.0%),31~35岁降至10.1%(95%CI:6.9%~13.6%),后随年龄增长,36~40岁时升至12.1%(95%CI:8.9%~6.1%)。各年龄组间HPV 16/18二价、HPV 6/11/16/18四价和HPV 6/11/16/18/31/33/45/52/58九价疫苗相关HPV型别感染率随年龄变化趋势均无统计学意义(Z=1.75,P=0.080;Z=1.91,P=0.056;Z=1.88,P=0.061)。

|
| 图 3 广西壮族自治区柳州市18~45岁女性各年龄组HPV感染情况 |
在本研究中CIN2+的分布情况:18~25岁11人(1.2%,95%CI:0.5%~1.9%);26~45岁23人(1.7%,95%CI:1.0%~2.4%),差异无统计学意义(Z=-0.73,P=0.314)。
4. HPV DNA感染在不同级别病变中分布:对所有研究对象采集的细胞学标本满意率为100%,其中2 037例(88.6%)液基细胞学诊断为NILM,147例(6.4%)诊断为ASC-US,91例(4.0%)诊断为LSIL,2例(0.1%)诊断为ASC-H,20例(0.9%)诊断为HSIL,2例(0.09%)诊断为AGC和1例(0.04%)诊断为AIS合并为3例可疑癌。组织学诊断33例(1.4%)CIN1,23例(1.0%)CIN2,11例(0.5%)CIN3,见表 1。与未感染高危型HPV者相比,高危型别HPV感染者被诊断为HSIL+病变(HSIL,ASC-H和可疑癌)的OR值为25.9(95%CI:8.8~76.1)。
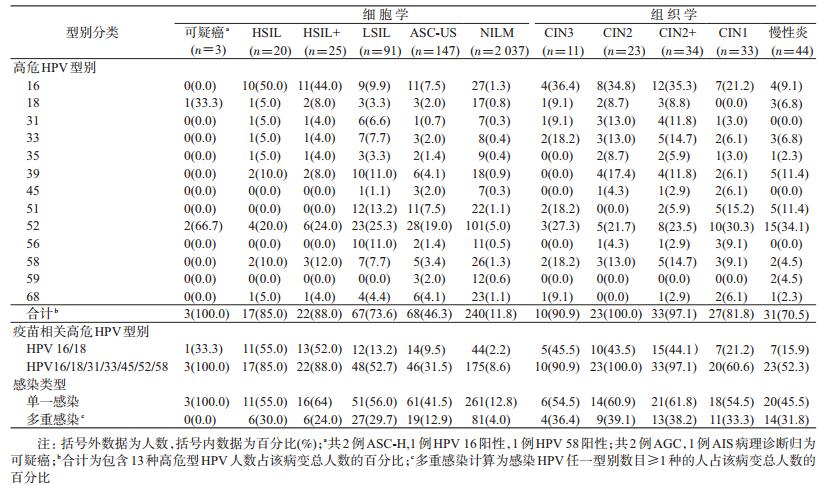
无论是细胞学还是组织学诊断,病变程度越高,高危型HPV检出率越高(均P<0.001)。如表 1所示,高度病变HSIL+(HSIL,ASC-H和可疑癌)病变标本中,HPV检出型别以HPV 16、52、58、18、39多见(HPV 18感染率同HPV 39相等);CIN2+病变标本中,HPV型别以HPV 16、52、33、58、31、39、18多见(HPV 33感染率同HPV 58相等,HPV 31感染率同HPV 39相等)。HPV 16/18二价疫苗型别在HSIL+病变人群中检出率为52.0%,CIN2+病变人群中检出率为44.1%,HPV 6/11/16/18/31/33/45/52/58九价疫苗相关高危型别检出率分别为88.0%、97.1%。
讨论本研究对柳州地区自然人群中18~45岁女性HPV感染特征进行横断面调查,结果显示,该人群HPV总感染率为22.7%(95%CI:21.0%~24.4%),高危型HPV感染率为17.3%(95%CI:16.0%~19.1%),在18~25岁和41~45岁呈现两个感染高峰,且以HPV 52、16、51、58、39为常见感染型别。高危型HPV感染率随宫颈细胞学和组织学病变严重程度增加而呈上升趋势,HPV 16/18二价和HPV 6/11/16/18/31/33/45/52/58九价疫苗相关高危型别在CIN2+病例中的检出率分别为44.1%和97.1%。
本研究报道柳州地区HPV总感染率与国内其他地区文献报道数据不完全一致:文献报道沈阳市15~59岁女性HPV总感染率为17%[12],深圳市同年龄段女性HPV总感染率为18%[13],山西省HPV感染率则为15%[8],而上海市≥18岁女性高危型HPV感染率为29.1%[14]。考虑到HPV感染率受检测方法和研究对象年龄影响,国内不同地区HPV感染率是否存在差异尚需更多可比性数据佐证。Zhao等[15]使用与本研究相同检测方法调查江苏省6 051名18~25岁女性,结果显示,HPV总感染率为18.5%(95%CI:17.6%~19.6%),略低于本研究同年龄段女性感染率(20.5%,95%CI:17.9%~23.1%,P=0.152),差异无统计学意义。同时本研究≥25岁女性人群感染率高于美国2007-2009年对40 901名>25岁女性的筛查所得的HPV阳性率(10%)(P<0.001)[16],提示我国>25岁女性感染特征与美国不同,且疾病负担更重。这种差异除了与研究对象的选择、标本采集和检测方法有关外,还与不同地区的文化、经济、性行为和生活习惯差异有关[6],然而我国广西壮族自治区柳州地区育龄女性18~25岁和41~45岁呈现双峰态势,即小年龄组HPV感染达到最高峰后持续下降,大年龄组感染率有所回升且高于美国同龄段女性[17],与Zhao等[18]报道的国内HPV感染特征一致。同时本研究中,CIN2+病变在大(≥26岁)、小(18~25岁)年龄组中未见明显差别。
高危型HPV感染型别分布在自然人群中与高度细胞学病变病例中不同。在本研究所有研究对象中,HPV 52、16、51、58、39为常见高危型HPV感染型别;在细胞学高度病变病例中,则以HPV 16、52、58、18、39多见。WHO、国际癌症研究机构(IARC)的报告指出HPV 16、18、31、58、52为全球最常见的5种型别,且HPV感染型别分布存在地区差异[19]。本研究自然人群感染型别特征与WHO、IARC数据有较大区别,且HPV 52流行率超过HPV 16,这一现象与我国台湾地区、广东省、浙江省及日本报道类似[20-21]。
本研究数据表明,无论细胞学还是组织学诊断,病变程度越严重,高危型HPV感染率越高,以HPV 16、52和58型最为常见,这一发现与既往研究一致[22]。也与WHO、IARC报道的HPV 16、52、58是发展中国家和地区高度病变中常见型别结论一致[19]。提示在柳州地区HPV 52、58等型别导致的疾病负担不可忽视,目前在中国唯一上市的疫苗为HPV 16/18型二价疫苗,急需推进九价HPV疫苗的研究,以期更为有效地预防宫颈癌的发生。
本研究采用方便抽样的方式,结论外推存在局限性,但考虑到样本量较大且年龄覆盖大部分育龄期女性,仍具备一定的代表性。
利益冲突: 无
| [1] | Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012[J]. CA Cancer J Clin, 2015, 65(2): 87–108. DOI:10.3322/caac.21262 |
| [2] | Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015[J]. CA Cancer J Clin, 2016, 66(2): 115–132. DOI:10.3322/caac.21338 |
| [3] | Walboomers JM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide[J]. J Pathol, 1999, 189(1): 12–19. DOI:10.1002/(ISSN)1096-9896 |
| [4] | Bosch FX, Lorincz A, Muñoz N, et al. The causal relation between human papillomavirus and cervical cancer[J]. J Clin Pathol, 2002, 55(4): 244–265. DOI:10.1136/jcp.55.4.244 |
| [5] | Muñoz N, Bosch FX, de Sanjosé S, et al. The causal link between human papillomavirus and invasive cervical cancer:a population-based case-control study in Colombia and Spain[J]. Int J Cancer, 1992, 52(5): 743–749. DOI:10.1002/(ISSN)1097-0215 |
| [6] | Castellsagué X. Natural history and epidemiology of HPV infection and cervical cancer[J]. Gynecol Oncol, 2008, 110(3 Suppl 2): S4–7. DOI:10.1016/j.ygyno.2008.07.045 |
| [7] | WHO Recommendations to assure the quality, safety and efficacy of recombinant human papillomavirus virus-like particle vaccines. WHO Expert Committee on Biological Standardization[Z]. 2016. http://www.who.int/biologicals/expert_committee/WHO_TRS_999_FINAL.pdf. |
| [8] | Dai M, Bao YP, Li N, et al. Human papillomavirus infection in Shanxi province, People's Republic of China:a population-based study[J]. Br J Cancer, 2006, 95(1): 96–101. DOI:10.1038/sj.bjc.6603208 |
| [9] | Yuan XY, Yang Y, Gu DH, et al. Prevalence of human papillomavirus infection among women with and without normal cervical histology in Shandong province, China[J]. Arch Gynecol Obstet, 2011, 283(6): 1385–1389. DOI:10.1007/s00404-010-1584-0 |
| [10] | Kleter B, Van Doorn LJ, Schrauwen L, et al. Development and clinical evaluation of a highly sensitive PCR-reverse hybridization line probe assay for detection and identification of anogenital human papillomavirus[J]. J Clin Microbiol, 1999, 37(8): 2508–2517. |
| [11] | IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Biological Agents. Lyon (FR):International Agency for Research on Cancer; 2012. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100B[M]. https://www.ncbi.nlm.nih.gov/books/NBK304348/. |
| [12] | Li LK, Dai M, Clifford GM, et al. Human papillomavirus infection in Shenyang city, People's Republic of China:A population-based study[J]. Br J Cancer, 2006, 95(11): 1593–1597. DOI:10.1038/sj.bjc.6603450 |
| [13] | Wu RF, Dai M, Qiao YL, et al. Human papillomavirus infection in women in Shenzhen city, People's Republic of China, a population typical of recent Chinese urbanisation[J]. Int J Cancer, 2007, 121(6): 1306–1311. DOI:10.1002/ijc.22726 |
| [14] | Zhang WY, Xue YZ, Chen M, et al. Prevalence of high-risk human papillomavirus infection in different cervical lesion among organized health-examination women in Shanghai, China[J]. Chin Med J, 2008, 121(16): 1578–1582. |
| [15] | Zhao FH, Zhu FC, Chen W, et al. Baseline prevalence and type distribution of human papillomavirus in healthy Chinese women aged 18-25 years enrolled in a clinical trial[J]. Int J Cancer, 2014, 135(11): 2604–2611. DOI:10.1002/ijc.28896 |
| [16] | Castle PE, Stoler MH, Wright TC Jr, et al. Performance of carcinogenic human papillomavirus (HPV) testing and HPV16 or HPV18 genotyping for cervical cancer screening of women aged 25 years and older:a subanalysis of the ATHENA study[J]. Lancet Oncol, 2011, 12(9): 880–890. DOI:10.1016/S1470-2045(11)70188-7 |
| [17] | De Sanjosé S, Diaz M, Castellsagué X, et al. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology:a Meta-analysis[J]. Lancet Infect Dis, 2007, 7(7): 453–439. DOI:10.1016/S1473-3099(07)70158-5 |
| [18] | Zhao FH, Lewkowitz AK, Hu SY, et al. Prevalence of human papillomavirus and cervical intraepithelial neoplasia in China:a pooled analysis of 17 population-based studies[J]. Int J Cancer, 2012, 131(12): 2929–2938. DOI:10.1002/ijc.27571 |
| [19] | BruniL BR, Albero G, Aldea M, et al. ICO Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report[R].(2015-12-23)[2016-08-20]. 2015. |
| [20] | Lin M, Yang LY, Li LJ, et al. Genital human papillomavirus screening by gene chip in Chinese women of Guangdong province[J]. Aust N Z J Obstet Gynaecol, 2008, 48(2): 189–194. DOI:10.1111/j.1479-828X.2008.00844.x |
| [21] | Ye J, Cheng XD, Chen XJ, et al. Prevalence and risk profile of cervical Human papillomavirus infection in Zhejiang province, southeast China:a population-based study[J]. Virol J, 2010, 7: 66. DOI:10.1186/1743-422X-7-66 |
| [22] |
李亚军, 杨明珠, 秦文芝.
不同级别宫颈病变中HPV感染状态的临床分析[J]. 中国实验诊断学, 2015, 19(1): 71–74.
Li YJ, Yang MZ, Qin WZ. Clinical analysis of human papillomavirus infection status in different grade cervical lesions[J]. Chin J Lab Diagn, 2015, 19(1): 71–74. |