 2016, Vol. 37
2016, Vol. 37文章信息
- 黄少芬, 朱瑶, 林修全, 陈铁晖, 叶莺, 钟文玲, 林曙光, 殷鹏 .
- Huang Shaofen, Zhu Yao, Lin Xiuquan, Chen Tiehui, Ye Ying, Zhong Wenling, Lin Shuguang, Yin Peng .
- 应用倾向性评分加权法估计2012-2014年福建省疾病监测系统死亡病例漏报率
- Estimation of underreporting rate of death cases in disease surveillance system of Fujian province using propensity score weighting method, 2012-2014
- 中华流行病学杂志, 2016, 37(11): 1476-1479
- Chinese journal of Epidemiology, 2016, 37(11): 1476-1479
- http://dx.doi.org/10.3760/cma.j.issn.0254-6450.2016.11.009
-
文章历史
收稿日期: 2016-05-16




2. 100050 北京, 中国疾病预防控制中心慢性非传染性疾病预防控制中心
2. National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100050, China
死因监测数据是公共卫生信息的最重要和最基本的信息之一。人群中的死亡水平、死亡原因和死亡模式是评估人群健康状况和卫生需求的依据[1-2]。监测数据完整性是其质量的一项重要指标,而发展中国家的死亡数据漏报是较常见的问题。福建省自1986年开始在部分县、市实行死亡登记报告制度,后不断调整扩大,2013年建立覆盖1 000万人口样本的疾病监测系统。为评价福建省死因监测资料的完整性,对2012-2014年福建省疾病监测系统死因监测漏报调查结果进行分析。
资料与方法1.资料来源:采用分层整群随机抽样方法,在福建省20个疾病监测点随机抽取3个乡镇(街道),每个抽中的乡镇(街道)随机抽取3个行政村(居委会),抽中村(居委会)的所有家庭均为调查家庭,调查家庭的所有户籍成员均为调查对象。收集调查村(居委会)2012年1月1日至2014年12月31日户籍人口资料以及期间发生的所有户籍人口死亡信息,由于有10个死因监测点自2013年才开始设点,调查时间为2013年1月1日至2014年12月31日。调查内容包括死者姓名、性别、身份证号、死亡年龄、死亡日期、家属联系电话及死亡原因,并通过与常规死因报告信息比对,确定是否漏报。漏报的个案需入户调查,收集婚姻状况、文化程度、职业、死亡地点、生前最高诊断单位及诊断依据、调查结局等信息。
2.质量控制:抽样由福建省疾病预防控制中心(疾控中心)统一完成,并严格控制置换比例。调查员从村或居委会、殡葬部门、户籍管理部门、计划生育部门、妇幼保健部门等多渠道获取死亡名单,通过核对、查重和补漏,保证死亡名单的完整性。判断死亡个案是否漏报,采用多变量系统自动匹配和人工匹配相结合的方式,以减少人为误差。
3.统计学分析:数据处理和统计采用SPSS 20.0软件。利用基于logistic回归模型的倾向性评分加权法对漏报率进行调整:①采用logistic回归方法对漏报率的影响因素进行分析并建立模型,分析因素包括城乡、性别、年份、年龄组和死因;采用前进法选择自变量(纳入标准是0.05,排除标准是0.10);②应用logistic回归模型预测每例死亡个案的漏报率Pi,加权系数Wi=1/(1-Pi),2012-2014年的实际死亡数
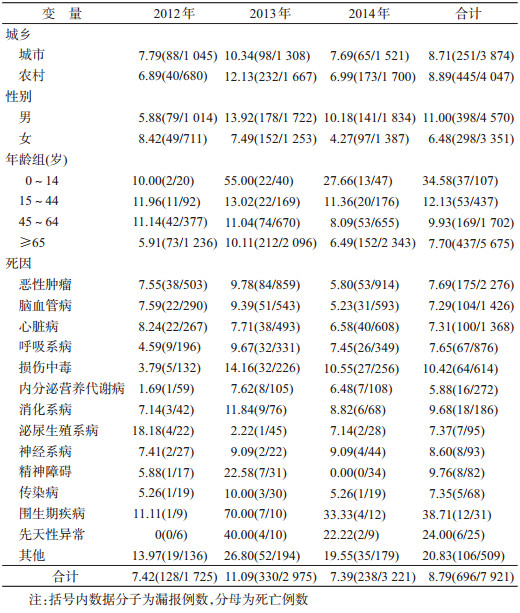
1.粗漏报率:漏报调查共覆盖180个村(居委会)1 467 236人,收集死亡个案7 921例,其中漏报696例,完成入户调查679例,失访17例。2012-2014年总粗漏报率为8.79%,其中2013年的粗漏报率最高为11.09%,2012年和2014年相近。男性粗漏报率(11.00%)高于女性(6.48%)。以0~14岁人群死亡的粗漏报率最高(34.58%),≥65岁人群最低(7.70%)。以死因为围生期疾病、先天性异常和损伤中毒的死亡人群粗漏报率较高,均>10%(表 1)。
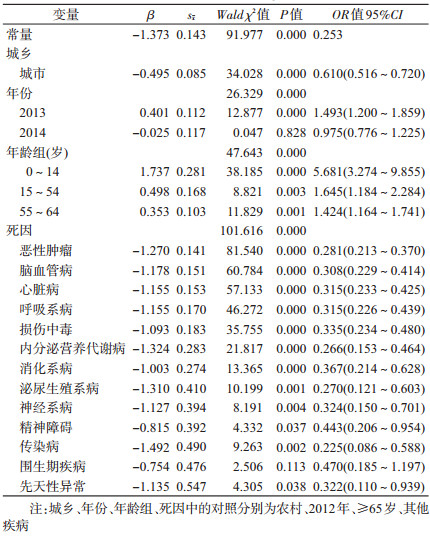
2.死亡漏报影响因素及其危险度分析:logistic回归结果显示,在死因监测过程中,低年龄组死亡人群是漏报发生的危险因素,死者所处的年龄组越小,发生漏报的可能性越大,0~14岁死亡人群漏报的风险较≥65岁人群增加5.681倍。城市是漏报发生的保护因素,城市居民死亡漏报发生概率是农村的0.610倍。死于恶性肿瘤、脑血管病、心脏病、呼吸系病、损伤中毒、内分泌营养代谢病、消化系病、泌尿生殖系病、神经系病、精神障碍、传染病和先天性异常的漏报低于死于其他疾病者(表 2)。
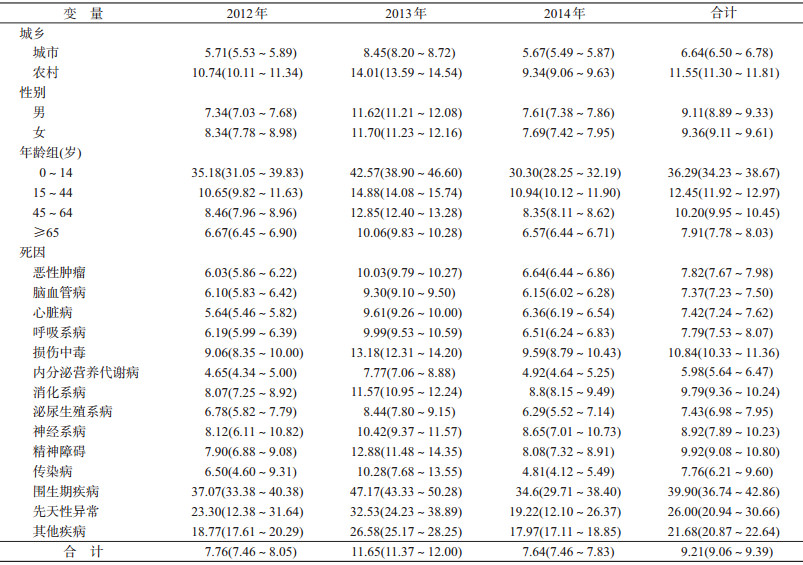
3.基于倾向性评分加权法的调整漏报率:经倾向性评分加权调整后,2012-2014年总的漏报率为9.21%(95%CI:9.06%~9.39%),各年漏报率分别是7.76%(95%CI:7.46%~8.05%)、11.65%(95%CI:11.37%~12.00%)、7.64%(95%CI:7.46%~7.83%)。城乡漏报率的差距较粗漏报率明显加大,城市死亡人群的漏报率是6.64%(95%CI:6.50%~6.78%),农村为11.55%(95%CI:11.30%~11.81%)。与粗漏报率相反,经调整后女性的漏报率(9.36%,95%CI:9.11%~9.61%)略高于男性(9.11%,95%CI:8.89%~9.33%)。分年龄组和分死因别的漏报率均较粗漏报率有所提高(表 3)。
本研究通过开展漏报调查来估计人群死亡的漏报,漏报调查的人群和常规监测人群在内部混杂因素构成上往往不同,存在抽样误差,有必要采用“标准化法”对粗漏报率进行调整。logistic回归分析显示,城乡、年份、年龄组和死因均是漏报率的影响因素,由于混杂因素较多时,无法采用传统的标准化法对漏报率进行调整。倾向评分可以将许多变量综合为一个变量,通过调整倾向评分这一个变量来使各混杂变量在两组人群中的分布趋于一致[3],一些研究也有证实[4-5]。
2012-2014年福建省疾病监测系统总的粗漏报率为8.79%,较2006-2008年漏报率(11.90%)有所下降[6]。采用倾向性评分加权法调整后,2012-2014年福建省疾病监测系统总的漏报率为9.21%,其中2013年的死亡漏报率(11.65%)明显较高,可能与2013年新增的10个疾病监测点工作基础较为薄弱有关。
分析结果还显示,农村居民死亡漏报率(11.55%)高于城市(6.64%),与文献报道一致[7-8],可能与农村监测点的报告模式落后(由村医-乡镇-疾控中心逐级报告)及当地某些社会因素相关。值得重视的是,福建省0~14岁儿童的死亡漏报率为36.29%,明显高于2009-2011年全国疾病监测点的漏报调查结果[4]。由于低年龄组人群死亡个案较少,得到的漏报率较不稳定,因此在结论推广时需慎重。0~14岁儿童死亡漏报问题一直是福建省死因监测工作的难点。其中婴儿死亡率和5岁以下儿童死亡率普遍偏低,不能如实反映实际水平,需要重点加强对低年龄组人群的死亡登记报告管理。WHO认为,要掌握每个人的出生和死亡数据,唯一的途径就是民事登记[9]。建议政府完善民事登记系统,通过法律手段确保死亡登记的强制实施;卫生部门积极协调公安、民政等部门,落实死因登记报告制度,理顺死亡证的签发和使用流程;医疗卫生机构加强常规死因监测的质量管理,提高主动监测的技术水平,多途径地收集资料,切实提高监测数据质量。
利益冲突: 无| [1] |
王艳红, 李立明, 李天霖.
《全国卫生统计年报(/鉴)》1987-2003年资料可靠性评价[J]. 中华流行病学杂志 , 2007, 28(2) : 195–198.
Wang YH, Li LM, Li TL. Evaluation on the reliability of the national health statistical yearbooks, 1987-2003[J]. Chin J Epidemiol , 2007, 28(2) : 195–198. |
| [2] | Mathers CD, Fat DM, Inoue M, et al. Counting the dead and what they died from:an assessment of the global status of cause of death data[J]. Bull World Health Organ , 2005, 83(3) : 171–177. DOI:10.1590/S0042-96862005000300009 |
| [3] |
李智文, 刘建蒙, 任爱国.
基于个体的标准化法--倾向评分加权[J]. 中华流行病学杂志 , 2010, 31(2) : 223–226.
Li ZW, Liu JM, Ren AG. Introduction to an individual-based standardization method-propensity score weighting[J]. Chin J Epidemiol , 2010, 31(2) : 223–226. DOI:10.3760/cma.j.issn.0254-6450.2010.02.024 |
| [4] | Guo K, Yin P, Wang LJ, et al. Propensity score weighting for addressing under-reporting in mortality surveillance:a proof-of-concept study using the nationally representative mortality data in China[J]. Popul Health Metr , 2015, 13 : 16. DOI:10.1186/s12963-015-0051-3 |
| [5] | Curtis LH, Hammill BG, Eisenstein EL, et al. Using inverse probability-weighted estimators in comparative effectiveness analyses with observational databases[J]. Med Care , 2007, 45(10 Suppl 2) : S103–107. DOI:10.1097/MLR.0b013e31806518ac |
| [6] |
李晓庆, 钟文玲, 林曙光.
福建省疾病监测系统2006-2008年死因监测漏报调查[J]. 现代预防医学 , 2011, 38(18) : 3778–3779.
Li XQ, Zhong WL, Lin SG. Investigation on the death under-reporting in disease monitoring system from 2006 to 2008 in Fujian[J]. Mod Prev Med , 2011, 38(18) : 3778–3779. |
| [7] |
王琳, 王黎君, 蔡玥, 等.
2006-2008年全国疾病监测系统死亡漏报调查分析[J]. 中华预防医学杂志 , 2011, 45(12) : 1061–1064.
Wang L, Wang LJ, Cai Y, et al. Analysis of under-reporting of mortality surveillance from 2006 to 2008 in China[J]. Chin J Prev Med , 2011, 45(12) : 1061–1064. DOI:10.3760/cma.j.issn.0253-9624.2011.12.002 |
| [8] |
李卫红, 杨国强.
从居民死亡漏报分析谈死因监测网络直报存在问题及对策[J]. 疾病监测 , 2006, 21(11) : 607–608.
Li WH, Yang GQ. Discussion on the problems in the direct network report system and the countermeasures based on the analysis of missing reports on the deaths among resident[J]. Dis Surveill , 2006, 21(11) : 607–608. DOI:10.3784/j.issn.1003-9961.2006.11.018 |
| [9] | Abouzahr C, Rampatige R, Lopez A, et al. When civil registration is inadequate:interim methods for generating vital statistics[J]. Pac Health Dialog , 2012, 18(1) : 215–230. |